

Abstract
In 2011 census, 5.3% of the Indian population was > 65 years of age. This number has steadily grown over past few years and is steeply growing. Healthcare burden of elderly diabetics is immense and proper diagnosis and treatment alone can prevent further complications. According to the most recent surveillance data in U.S., the prevalence of diabetes among U.S. adults aged ≥65 years varies from 22 to 33%, depending on the diagnostic criteria used. In CSIR-NEERI, India, we have healthcare system wherein a fixed and limited number of patients are treated for their lifetime by qualified practitioners with negligible financial burden of the treatment costs. The patients have regular monthly follow up and hence we diagnose Diabetes and evaluate the control and diagnose micro vascular and macro vascular complications in all patients. We did retrospective analysis of all elderly patients following up in NEERI Hospital to find the exact prevalence of T2DM in elderly. It was observed that from total 585 elderly people, 178 had T2DM (30.42%- Prevalence). The sex ratio of Diabetic males to females was almost equal (1:0.97). Obesity was present in 114 people (64%). High prevalence of hypertension was found in Diabetic elderly population (80%). Comparing our prevalence rates with few other studies, it was found that our prevalence rates are quite high. The contributing factors may be urban living, with high prevalence of central obesity and Asian ethnicity, over and above, data of all patients undergoing treatment is available. We treated all diabetics with persistent values of Systolic BP > 130 mm of Hg and Diastolic values of BP > 80mm of Hg as Hypertensives, in order to achieve reduction in cardiovascular mortality and morbidity. This paper is for awareness of disease burden, in real primary care setup. It is not cross-sectional study but study with 100% inclusion of beneficiaries’. This is real world urban diabetes prevalence, also associated hypertension and central obesity prevalence.
Keywords: Elderly population, hypertension, ideal primary health care facility, male-female ratio, Obesity, prevalence of type 2 DM
INTRODUCTION
In 2011 census, 5.3% of the Indian population was >65 years of age.[1] This number has steadily grown over past few years and is steeply growing. The segment of people >80 years of age is increasing at the fastest rate. Furthermore, whereas the majority of those >65 are now between the ages of 65 years and 75 years, there will be a shift in demography over the next few decades such that the majority of the geriatric population will be ≥75 years of age.[2]
With enhancement of diagnostic and treatment facilities, with better healthcare facilities and awareness, we have a growing population of elderly people. With the rise in this population group, there is increase in the illness burden and hence, the healthcare burden of each individual. Over and above as the age advances, this is the population which is neglected worldwide. Proper evaluation of their problems, correct diagnosis and suitable treatment are the key factors in reducing the illness burden. This enhances the quality of life of the patients, which is of utmost importance.
Of all the diseases, type 2 diabetes mellitus (T2DM) is the single most disease affecting a large number of elderly populations along with Hypertension. Diabetes and its complications take a major toll on the quality of life of the elderly and the healthcare costs of the society. Diabetes further increases the risk of cardiovascular mortality in older people. The management of diabetes in elderly requires special care and attention. According to the most recent surveillance data, the prevalence of diabetes among U.S. adults aged ≥65 years varies from 22 to 33%, depending on the diagnostic criteria used.[3] The epidemic of type 2 diabetes is clearly linked to increasing rates of overweight and obesity in the U.S. population, but projections by the Centers for Disease Control and Prevention (CDC) suggest that even if diabetes incidence rates level off, the prevalence of diabetes will double in the next 20 years, in part due to the aging of the population. Other projections suggest that the number of cases of diagnosed diabetes in those aged ≥65 years will increase by 4.5-fold (compared to 3-fold in the total population) between 2005 and 2050. Older adults with diabetes have the highest rates of major lower-extremity amputation, myocardial infarction (MI), visual impairment, and end-stage renal disease of any age-group.[3] Also, there is sufficient evidence to prove that Diabetes Mellitus (DM) is strongly linked to sudden cardiac death.[4] Hence, it is necessary to screen the entire population for presence of T2DM and treat them according to the guidelines. This is practically a difficult task, but when small and fixed groups are treated by definite and same diabetes practitioners, the results can be encouraging.
In Council of Scientific and Industrial Research-National Environmental Engineering Research Institute (CSIR-NEERI), India, we have healthcare system wherein we treat a limited and fixed population. The burden of healthcare cost is born by Institute and negligible to the patient. We have two qualified Physicians and one Family Practitioner treating these patients. All the patients follow up with us right from the day they enter into this institution until thereafter for lifetime. Since the facility is free for patients, all prescriptions are taken from these doctors and very rarely outside medical facility is used. This assures continuous follow up. In addition, we arrange regular camps 2-3 times in a year to diagnose diabetes, to evaluate the control and diagnose micro vascular and macro vascular complications.
AIM
To find prevalence of T2DM in all elderly population (≥60 years of age) taking treatment at NEERI Hospital.
Secondary aims
To find the sex ratio of diabetic elderly population,
To find association with central obesity,
To find association with hypertension.
MATERIALS AND METHODS
Retrospective analysis of all elderly patients following up in NEERI Hospital was done. Elderly population was defined as people more than 60 years. of ages on May 1, 2013. Prevalence of T2DM was calculated. T2DM was diagnosed according to American Diabetes Association Guidelines: Fasting Plasma Glucose ≥ 126 mg/dl (fasting for at least 8 hours), 2-hour Plasma glucose ≥ 200 mg/dl and/or glycosylated hemoglobin ≥ 6.5% or patients on antidiabetic medication. No. of males and females were noted. No. of patients with central obesity were noted. Central obesity was considered if abdominal circumference at umbilicus in supine position was >90 cm for males and >80 cm for females. Associated hypertension was evaluated. Systolic blood pressure (BP) >130 mm of Hg and Diastolic BP > 80 mm of Hg were considered abnormal for diabetic patients.
Patients come to the hospital for monthly check ups and monthly medicines. During these visits, risk stratification of the patients, close monitoring of their symptoms, signs and lab values are done as per recommendations. Moreover, we regularly conduct 2-3 camps every year to diagnose diabetes, to evaluate the control and diagnose micro vascular and macro vascular complications. We get annual health checkup of all patients, especially of those who are at high risk. We have such a system, that all patients have 100% follow up, and therefore, we do not miss a single case of diabetes.
Statistical method
The prevalence of the elderly population was calculated using the direct standardization method. Multiple logistic regression analysis was conducted to look for the association of various parameters (categorical) with diabetes.
RESULTS
There are a total of 585 elderly people following up at NEERI Hospital. Out of these, 178 have been diagnosed till date to have T2DM. Thus, the prevalence rate of T2DM in elderly population is 30.42%.
Out of these, 90 (50.56%) are males and 88 (49.43%) are females. Thus almost equal numbers of both the sexes are affected, the ratio being-(1:0.97). One hundred and fourteen patients (64.04%) have central obesity. Eighty percent patients had associated hypertension.
DISCUSSION
Rising geriatric population, almost 5.3% of the entire population is a major concern to health economists.[1] High geriatric population means a higher number of patients with various chronic diseases and increasing percentage of lifetime health care costs are accounted for this population. As our population lives longer and medical advances continue to develop, individuals will have a greater chance of developing diseases that occur more commonly during later life; many individuals will also live with chronic illnesses such as diabetes for many more years than might be possible at present.[2]
According to the most recent surveillance data, the prevalence of diabetes among U.S. adults aged ≥65 years varies from 22 to 33%, depending on the diagnostic criteria used.[3] Postprandial hyperglycemia is a prominent characteristic of type 2 diabetes in older adults, contributing to observed differences in prevalence depending on which diagnostic test is used. Using the A1C or fasting plasma glucose diagnostic criteria, as is currently done for national surveillance, one-third of older adults with diabetes are undiagnosed. The epidemic of type 2 diabetes is clearly linked to increasing rates of overweight and obesity in the U.S. population, but projections by the CDC suggest that even if diabetes incidence rates level off, the prevalence of diabetes will double in the next 20 years, in part due to the aging of the population.[3] Other projections suggest that the number of cases of diagnosed diabetes in those aged ≥65 years will increase by 4.5-fold (compared to 3-fold in the total population) between 2005 and 2050.[1]
In a study from South Indian area, prevalence rates of T2DM and impaired glucose tolerance (IGT) were surveyed. In urban areas, 211 (23.7%) had diabetes, and 101 (12.4%) had IGT. In the rural area, 56 (9.9%) had diabetes, and 82 (14.9%) had IGT. In rural South India, the age-adjusted rates for known diabetes in the middle-aged and elderly subjects were unexpectedly high, considering the poor socioeconomic circumstances, decreased health awareness and decreased access to medical facilities.[5,6]
In a study conducted in Trivandrum, the capital city of Kerala State, overall prevalence of T2DM was found to be 16.3%. This is comparable to the prevalence of diabetes among Indians residing in Singapore. The prevalence is even higher among people of Indian origin in Fiji. These data suggest that increasing life-expectancy (as in Kerala State) and changes in lifestyle and nutrition may result in substantially higher incidence of diabetes in India than currently established.[7]
Data from the 2011 National Diabetes Fact Sheet in U.S. (released January 26, 2011) states that amongst people with age 65 years or older 26.9% of all people have diabetes.[8]
The overall 10-year incidence of diabetes and Impaired fasting glucose was 9.3% and 15.8%, respectively, in a study conducted in Australia to find 10-year incidence of Diabetes in older Australians.[9]
Participants with metabolic syndrome in community-based study of prevalence of T2DM from California, using World Health Organization (WHO) Criteria, the results of age group 50-89 years. were as follows: 16.5% males and 12.7% females.[10]
In another study from Denmark, T2DM was prevalent in 10% at age 70 years and 12% at age 80 years (WHO Criteria)[11] in 1982 study.
In yet another study from Finland, 33.8% men and 37.9% women were found to have abnormal glucose tolerance according to WHO Criteria.[12]
In a Swedish study, prevalence of T2DM by WHO criteria was 7.6% in men and 4.0% in women respectively.[13] But this was older study [Figure 1].
Figure 1.
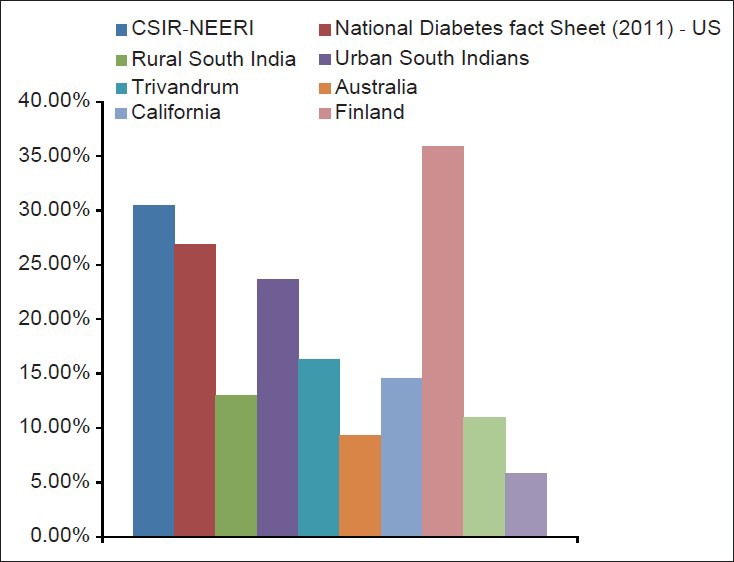
Comparative data of prevalence of T2DM in elderly
The differences in the prevalence rates at various places could be due to difference in the ethnicity,[14] the lifestyle of the patients and the population screened. In our case, prevalence rates are high due to ethnicity, urban lifestyle, central obesity, and the fact that all the geriatric patients who take treatment at our hospital are screened for Diabetes.
Hence, we can see that, on screening all the patients in a community, the prevalence rates of diagnosis of T2DM increase. The more the number of people, are diagnosed to have T2DM, the better will be their management and hence secondary prevention of complications.
In our study, the prevalence of Diabetes in elderly males and females was almost similar. This proves that when a complete surveillance is done, the sex difference in prevalence of Diabetes in elderly is negligible. The difference in the ratio of male sex to female sexing other studies may be due to less number of females being included in the study. Also, one more reason for high female prevalence rates in our population is that, many of these females are widows whose husbands have expired due to cardiovascular causes, both related and unrelated to DM.
Obesity was found in 64% patients in our study. With advancing age, lean body mass decreases and percent adiposity increases, but there may be little or no change intotal body weight. Hence, it is necessary to look for central obesity and not Body Mass Index, which may not depict true obesity. Aging is associated with sarcopenia, referred to as the universal and involuntary decline in skeletal muscle mass. This result in loss of muscle strength and contributes to the eventual inability of the elderly individual to carry out tasks of daily living. A major mechanism of insulin action is facilitating glucose uptake by the muscle. A reduction in lean body mass means the eventual inability to adipose glucose, reduced metabolically active lean tissue mass, and reduced physical activity.[7,15]
Hypertension is well-recognized as an insulin-resistant state. Hypertension is a common comorbidity among persons with diabetes and its prevalence increases with advancing age. In people with type 2 diabetes, hypertension is a major risk factor for cardiovascular disease. Elderly patients with hypertension and DM have a higher mortality risk than similarly aged controls without DM. The United Kingdom Prospective Diabetes Study blood-pressure trial demonstrated the benefits of more intensive BP control in individuals with type 2 diabetes. Those persons randomized to tight BP control (mean treated BP 144/82 mmHg) with an angiotensin-converting enzyme (ACE) inhibitor or beta-blocker had a 24% relative risk reduction in diabetes-related end points, 32% fewer diabetes-related deaths, and 44% fewer strokes compared with those in the less-tight control arm (mean treated BP 157/87 mmHg). Hence, detection of hypertension amongst the diabetics and maintaining its control is essential for reducing the cardiovascular mortality of these patients.[16,17] We have 80% elderly diabetic patients who are treated for hypertension. Keeping stricter criteria, we tend to treat more patients and thus reduce their cardiovascular mortality.
CONCLUSION
Thus, the prevalence rate of T2DM in elderly population is 30.42%. Almost equal numbers of both the sexes are affected, the ratio being-(1:0.97). 64.04% have central obesity. Eighty percent patients had associated hypertension.
The health burden of elderly diabetics is immense. The associated complications complicate the matters. Both the life span and quality of life are affected badly. There is enhanced workload on the medicare system.
But in a system like ours, wherein a fixed and limited number of patients are treated for their lifetime by qualified practitioners with negligible financial burden of the treatment costs, the scenario is quite different. The high prevalence of elderly diabetics, i.e., 30.42%, in our set up is probably due to higher rates of detection, ethnicity, lifestyle, and obesity. Duration of diabetes is not in preview of this paper, but many of these diabetics have been diagnosed to have diabetes since long.
Like many other studies showing importance of Primary Healthcare provision and healthcare outcomes of beneficiaries and reduction in the treatment cost,[18,19,20] the salient features to follow from this study are:
A fixed and limited group to follow lifetime for their chronic illness with a specific trained and qualified practitioner.
To screen and treat early, monitoring closely the high risk population.
This paper is for awareness of disease burden, in real primary care setup. It is not cross-sectional study but study with 100% inclusion of beneficiaries’. This is real world urban diabetes prevalence, also associated hypertension and central obesity prevalence.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Census Population, Census of India, Government of India Portal. 2011 [Google Scholar]
- 2.Gambert SR, Pinkstaff S. Emerging epidemic. Diabetes in older adults: Demography, economic impact, and pathophysiology. Diabetes Spectr. 2006;19:221–8. [Google Scholar]
- 3.Kirkman SM, Briscoe VJ, Clark N, Florez H, Haas LB, Halter JB, et al. Diabetes in older adults: A consensus report © 2012 by the American Diabetes Association and the American Geriatrics Society. doi: 10.1111/jgs.12035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bergner DW, Goldberger JJ. Diabetes Mellitus and sudden cardiac death: What are the data? Cardiol J. 2010;17:117–29. [PubMed] [Google Scholar]
- 5.Ramachandran A, Snehalatha C, Shyamala P, Vijay V, Viswanathan M. High prevalence of NIDDM and IGT in an elderly south Indian population. Diabetes Care. 1994;17:1190–2. doi: 10.2337/diacare.17.10.1190. [DOI] [PubMed] [Google Scholar]
- 6.Ramachandran A, Snehalatha C, Kapur A, Vijay V, Mohan V, Das AK, et al. Diabetes Epidemiology Study Group in India (DESI): Highprevalence of diabetes and impaired glucose tolerance in India: National Urban Diabetes Survey. Diabetologia. 2001;44:1094–101. doi: 10.1007/s001250100627. [DOI] [PubMed] [Google Scholar]
- 7.Kesavadev JD, Short KR, Nair KS. Diabetes in old age: An emerging epidemic. J Assoc Physicians India. 2003;51:1083–94. [PubMed] [Google Scholar]
- 8.Data from the 2011 National diabetes fact sheet released Jan 26, 2011. J Assoc Physicians India. 2003:51. [Google Scholar]
- 9.Cugati S, Wang JJ, Rochtchina E, Mitchell P. Ten-year incidence of diabetes in older Australians: The blue mountains eye study. Med J Aust. 2007;186:131–5. doi: 10.5694/j.1326-5377.2007.tb00836.x. [DOI] [PubMed] [Google Scholar]
- 10.Wingard DL, Sinsheimer P, Barrett-Connor EL, McPhillips JB. Community-based study of prevalence of NIDDM in older adults. Diabetes Care. 1990;13(Suppl 2):3–8. [Google Scholar]
- 11.Agner E, Thorsteinsson B, Eriksen M. Impaired glucose tolerance and diabetes mellitus in elderly subjects. Diabetes Care. 1982;5:600–4. doi: 10.2337/diacare.5.6.600. [DOI] [PubMed] [Google Scholar]
- 12.Mykkanen L, Laakso M, Uusitupa M, Pyorala K. Prevalence of diabetes and impaired glucose tolerance in elderly subjects and their association with obesity and family history of diabetes. Diabetes Care. 1990;13:1099–105. doi: 10.2337/diacare.13.11.1099. [DOI] [PubMed] [Google Scholar]
- 13.Ohlson LO, Larsson B, Eriksson H, Svardsudd K, Welin L, Tibblin G. Diabetes mellitus in Swedish middle-aged men: The study of men born in 1913 and 1923. Diabetologia. 1987;30:386–93. doi: 10.1007/BF00292539. [DOI] [PubMed] [Google Scholar]
- 14.McBean AM, Li S, Gilbertson DT, Collins AJ. Differences in diabetes prevalence, incidence, and mortality among the elderly of four racial/ethnic groups: Whites, blacks, hispanics, and Asians. Diabetes Care. 2004;27:2317–24. doi: 10.2337/diacare.27.10.2317. [DOI] [PubMed] [Google Scholar]
- 15.Wilson PW, Kannel WB. Obesity, diabetes, and risk of cardiovascular disease in the elderly. Am J Geriatr Cardiol. 2002;11:119–23,125. doi: 10.1111/j.1076-7460.2002.00998.x. [DOI] [PubMed] [Google Scholar]
- 16.ACCF/AHA 2011 Expert Consensus Document on Hypertension in the Elderly a Report of the American College of Cardiology Journal of the American College of Cardiology by the American College of Cardiology Foundation and the American Heart Association, Foundation Task Force on Clinical Expert Consensus Documents Developed in Collaboration With the American Academy of Neurology, American Geriatrics Society, American Society for Preventive Cardiology, American Society of Hypertension, American Society of Nephrology, Association of Black Cardiologists, and European Society of Hypertension., expert consensus document. 2011:57. doi: 10.1016/j.jacc.2011.01.008. [DOI] [PubMed] [Google Scholar]
- 17.Katz P, Gilbert J. Diabetes and cardiovascular disease among older adults: An update on the evidence. Geriatr Aging. 2008;11:509–14. [Google Scholar]
- 18.Wright RA. Community-oriented primary care. The cornerstone of health care reform. JAMA. 1993;269:2544–7. [PubMed] [Google Scholar]
- 19.Shetty S, Secnik K, Oglesby AK. Relationship glycemic control to total diabetes-related costs for managed care health plan members with type 2 diabetes. J Manag Care Pharm. 2005;11:559–64. doi: 10.18553/jmcp.2005.11.7.559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Chang CH, Stukel TA, Flood AB, Goodman DC. Primary care physical workforce and medicare beneficiaries’ health outcomes. JAMA. 2011;305:2096–104. doi: 10.1001/jama.2011.665. [DOI] [PMC free article] [PubMed] [Google Scholar]