

Abstract
Objective:
Adiponectin- one of the most important adipokines plays a pivotal role in carbohydrate and lipid metabolism and vascular biology. Changing food trend and lifestyle has tremendously affected the health status of Nepalese population. Studies have shown that between 1996 and 2006 obesity in Nepal has increased from 1.6% to 10%. Studies have been conducted in Nepal on the prevalence of obesity and its correlation with lipid profile. But based on our knowledge, this is the first study correlating adiponectin with obesity and lipid profile in Nepal. This piece of work will certainly help to assess the impact of obesity in Nepalese population.
Materials and Methods:
Fifty four obese and Thirty six normal/lean participants were included from different locations of Kathmandu Valley. Anthropometric measurements like age, BMI, Waist circumference, hip circumference, waist to hip ratio, mid thigh circumference and chest circumferences were taken from each participant. Blood glucose, lipid profile and serum adiponectin levels were measured from overnight fasting samples.
Results:
Significant differences were observed in BMI, Waist Circumference, Hip Circumference, Waist to Hip Ratio (WHR) and Chest circumference between obese and normal groups. Fasting Blood Glucose, Serum Triglyceride, HDL Cholesterol, LDL Cholesterol, Total Cholesterol/HDL ratio, Non-HDL Cholesterol and Adiponectin Levels were significant between the groups. Inverse correlations were observed between adiponectin level and BMI, Waist Circumference, Hip Circumference, Waist to Hip ratio, Chest Circumference, Fasting Blood Glucose, Triglyceride, Total Cholesterol/HDL ratio, LDL/HDL Cholesterol ratio and Non-HDL Cholesterol levels. Positive correlation was found between adiponectin and HDL Cholesterol levels.
Conclusion:
Our study showed significant inverse association of serum adiponectin with obesity and lipid profile parameters except for Serum HDL Cholesterol level in Nepalese population.
Keywords: Adiponectin, lipid profile, obesity
INTRODUCTION
Obesity is a condition of abnormal or excessive fat accumulation in adipose tissue, which may lead to health impairment.[1] Earlier, obesity was recognized as a problem of high income countries and only seen in adults, but more recently, it is seen to spread in low income countries and to children and adolescents.[2] Seemingly simple energy imbalance in obesity is driven by a complex mixture of genetic, environmental, psychosocial and cultural factors.[3] Obese people are at high risk of developing type 2 diabetes, coronary heart disease, hypertension, cancers (endometrial, breast and colon), metabolic syndrome (a combination of high blood sugar, high blood pressure, high triglycerides and high cholesterol), dyslipidemia (e.g., high total cholesterol or triglycerides), stroke, non-alcoholic fatty liver disease, gallbladder disease and gynecological problems (abnormal menses, infertility). Obesity may also accelerate cognitive decline and increase deficits in academic achievement.[4,5] The increased risk of diseases is due to the metabolic changes associated with obesity as pathogenic products are released from more larger and numerous fat cells.[6]
Adipose tissue communicates with different biological systems through expression of a large number of bioactive mediators termed as “adipokines” and thus actively participates in the regulation of various biological functions.[7] One of the most important adipokines, i.e. adiponectin has been found to be involved in multiple biological processes in the human body. It was the first adipose tissue derived peptide observed to be dysregulated in obesity.[8]
Adiponectin is a 244-amino acid-long polypeptide, collagen like protein that is exclusively secreted by adipocytes and acts as a hormone.[9] Adiponectin plays a pivotal role in carbohydrate and lipid metabolism and vascular biology.[10] It regulates various metabolic processes through its stimulatory effects on signaling pathways for 5’-adenosine monophosphate-activated protein kinase (5’- adenosine monophosphate-activated protein kinase [AMPK]) and peroxisome proliferator activated receptor gamma (PPAR-g).[11] It is a major modulator of insulin action and resistance[12] and helps in the prediction of development of type 2 diabetes.[13,14,15] Adiponectin is also found to possess substantial anti-inflammatory properties.[4] Furthermore, adiponectin is also associated with lipid metabolism causing higher values of high density lipoprotein (HDL) cholesterol and lower values of triglycerides.[16]
Changing food trend and life-style has tremendously affected the health status of Nepalese population. Studies have shown that between 1996 and 2006 obesity in Nepal has increased from 1.6% to 10%.[17] Studies have been conducted in Nepal on the prevalence of obesity and its correlation with a lipid profile. However based on our knowledge, this is the first study correlating adiponectin with obesity and lipid profile in Nepal. This piece of work will certainly help to assess the impact of obesity in Nepalese population.
MATERIALS AND METHODS
Study population
In this study, a total number of 90 participants were included from different locations of Kathmandu Valley. Out of these, 54 of the participants were obese while 36 of the participants were normal/lean. All participants were asked for the history of diabetes, hormonal disorders, liver diseases, renal diseases and other chronic diseases. Those suspected of any disorders as indicated above were excluded.
Anthropometric measurements
After the patient consent, the height and weight of each candidate was taken in upright standing position without shoes. Height was measured using a measuring with accuracy of 0.5 cm and weight, on a digital glass scale, with an accuracy of 0.1 kg.
Body mass index (BMI) was calculated as weight in kilogram (Kg) divided by height squared (m2). According to the World Health Organization guidelines for Asians the individuals, both for men and women, having BMI < 18.5 (kg/m2) were termed as underweight, 18.5-22.9 (Kg/m2) as normal, 23-24.9 (Kg/m2) as overweight and ≥25 (kg/m2) as obese.[18]
Similarly, waist and hip circumferences were taken in the standing position (over a light garment) following normal expiration and waist being defined as the narrowest circumference between the costal margin and the iliac crest and hip as the widest circumference between the waist and the thigh. Waist to hip ratio (WHR) was calculated as waist circumference divided by hip circumference. Similarly, chest circumference was measured over a thin garment at the mid portion of the chest.
Sample collection
After an overnight fast of at least 12 h, blood samples were collected from the antecubital vein of each participant. Samples were collected in plain vials, allowed to clot, centrifuged at 3000 rpm for 10 min and serum separated. Separated serum samples were preserved at −20°C until assays were run.
Biochemical analysis
Blood glucose level was measured using the glucose oxidase peroxidase method (Systemic Reagent for Humastar 600, Human, Germany). The lipid profile was performed using CHOD-PAP method (Systemic Reagent for Humastar 600, Human, Germany). The low density lipoprotein (LDL) was calculated using the Friedewald formula.[19] All the biochemical tests were run in the fully autoanalyzer (Humastar 600, Human, Germany). The serodos and serodos plus were used as the quality control samples and autocal as the standard to calibrate the tests. Both internal and external quality assurance tools were employed routinely to ensure the quality of test results.
Adiponectin was measured using human adiponectin ELISA kit (EIA-4820, DRG Instrument GmbH, Germany) with sensitivity of <0.185 ng/ml.
Ethical clearance
Ethical clearance for the study was taken from Nepal Health Research Council, Nepal as per the Helsinki declaration of 1975.
Statistical analysis
All the statistical analysis were performed using IBM SPSS Statistics (version 19) software, IBM Corporation, USA. All tests of statistical significance were two sided with 95% confidence intervals.
RESULTS
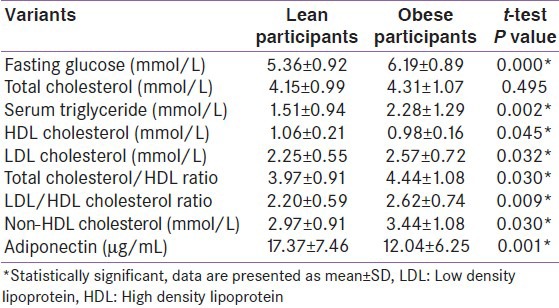
Among the normal/lean participants, 15 (41.6%) were male while 21 (58.4%) were female. Meanwhile, 30 (53.5%) male and 24 (46.5%) female participants were included as obese cases. Anthropometric indices in the participants are presented in Table 1. Statistically significant differences were observed in BMI, waist circumference, hip circumference, WHR and chest circumference between obese and normal groups. Biochemical parameters between obese and normal groups are presented in Table 2. Fasting blood glucose, serum triglyceride, HDL cholesterol, LDL cholesterol, total cholesterol/HDL ratio, non-HDL cholesterol and adiponectin levels were statistically significant between the groups.
Table 1.
Anthropometric indices in normal/lean and obese subjects
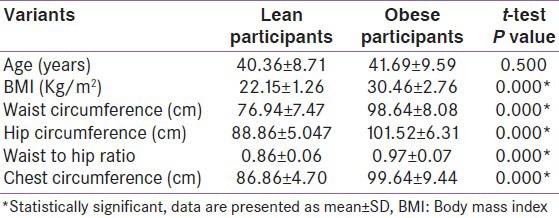
Table 2.
Biochemical parameters in normal/lean and obese subjects
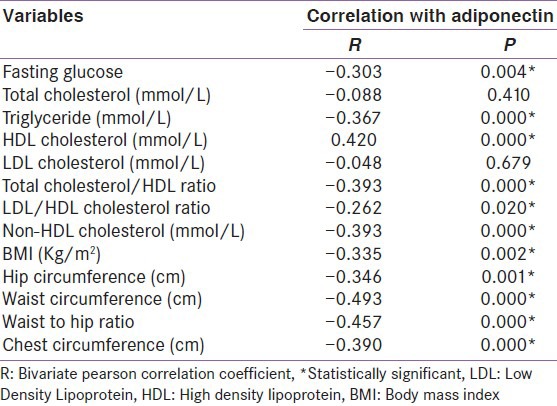
The Pearson correlation coefficient test was used to determine the correlations between the serum adiponectin levels and anthropometric characteristics and biochemical variables among groups [Table 3]. The results indicated significant inverse correlations between adiponectin level and BMI (R = −0.335; P = 0.002), waist circumference (R = −0.493; P = 0.000), hip circumference (R = −0.346; P = 0.001), WHR (R = −0.457; P = 0.000), chest circumference (R = −0.390; P = 0.000), fasting blood glucose (R = −0.303; P = 0.004), triglyceride (R = −0.367; P = 0.000), total cholesterol/HDL ratio (R = −0.393; P = 0.000), LDL/HDL cholesterol ratio (R = −0.262; P = 0.020) and non-HDL cholesterol (R = −0.393; P = 0.000) levels. A significant positive correlation was found between adiponectin and HDL cholesterol (R = 0.420; P = 0.000) levels.
Table 3.
Correlation of serum adiponectin with anthropometric and biochemical parameters
A multivariate linear regression analysis with the serum adiponectin level as the dependent variable showed a significant inverse association with BMI (β = −0.323; P = 0.002), waist circumference (β = −0.495; P = 0.000), hip circumference (β = −0.346; P = 0.001), WHR (β = −0.457; P = 0.000) and chest circumference (β = −0.390; P = 0.000). Furthermore, serum adiponectin level was inversely related to serum triglyceride (β = −0.311; P = 0.003), total cholesterol/HDL ratio (β = −0.393; P = 0.000) and non-HDL cholesterol (β = −0.393; P = 0.000) levels. Serum HDL cholesterol level was significantly and positively related to serum adiponectin level (β = 0.411; P = 0.000) [Figure 1].
Figure 1.
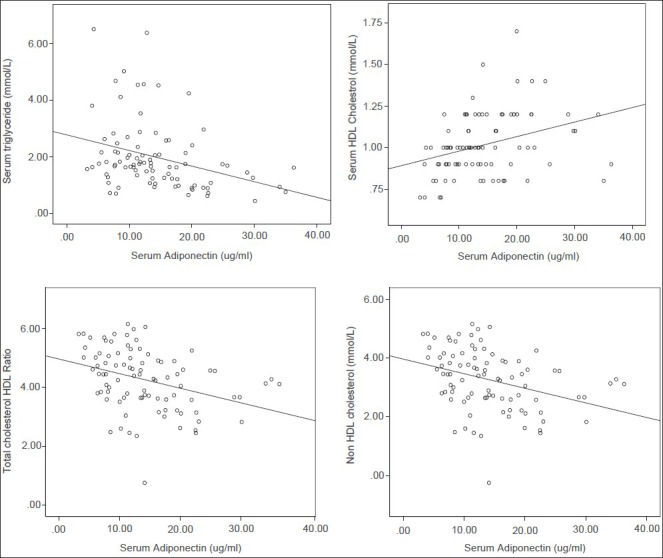
Correlations between serum adiponectin and serum lipid parameters
DISCUSSION
No published data has been found on serum adiponectin levels in Nepalese population. Hence, the present study focuses on the adiponectin level in obese and lean participants and its correlation with lipid profile. One of the studies carried out in healthy Japanese population showed a positive association of adiponectin with HDL cholesterol and inverse association with triglycerides and LDL cholesterol.[20] Similarly, a positive relationship of adiponectin with HDL cholesterol and a negative relationship with triglycerides have been reported in many studies.[21,22,23] A recent study[24] found adiponectin to be associated with HDL cholesterol and triglycerides in both lean and obese adolescents. In agreement to these findings our results demonstrated that adiponectin is inversely associated with total cholesterol (not statistically significant), triglycerides, LDL cholesterol and non-HDL cholesterol. Meanwhile, its positive association with HDL cholesterol was found.
Hepatic lipase may be a modulator between adiponectin and lipoproteins. This enzyme has been found to be inversely associated with adiponectin;[25] hence, decreased HDL cholesterol has been found in hypoadiponectinemia. This role is supported by findings that overproduction of catalytically active human hepatic lipase in the liver in mice led to decreased HDL cholesterol.[26] Similarly, it has been shown that the increase of HDL cholesterol is directly related to the adiponectin increase and inversely to the amount of weight loss.[27] High concentration of small dense LDL is another lipid disorder related to hipoadiponectinemia.[28]
Adiponectin has been proposed to protect against cardiovascular disease. It may be partially explained by its effects on lipid metabolism, particularly through HDL cholesterol (by removing cholesterol from foam cells, by inhibiting the oxidation of LDL and by anti-inflammatory and antithrombotic properties).[29] Furthermore, adiponectin has direct positive effects in the endothelium (endothelial dysfunction and infiltration, plaque instability) and in the myocardium (pathological cardiac remodeling and ischemic injury) effects.[8,30] It mediates its anti-inflammatory effect through the nuclear factor-κB pathway,[31] down regulates adhesion molecule expression on endothelial cells and enhances lipid clearance in numerous animal models.[32] In accord with such observations, exogenous adiponectin administration protects against development of atherosclerosis in apolipoprotein E–deficient mice.[33] It gets accumulated in myocardial tissue that has been damaged by ischemia/reperfusion injury[34] and protects myocardium by inhibiting inducible nitric oxide synthase and NADPH-oxidase expression and resultant oxidative stress[35] while it may protect against myocardial ischemia/reperfusion injury through AMPK and cyclooxygenase-2-dependent mechanisms.[36]
In addition, study carried out in obese adult females of Tehran showed an inverse relationship of adiponectin to fat distribution indices (waist, hip circumference and WHR).[37] Accordingly our findings confirmed the negative association of adiponectin with BMI, waist circumference, hip circumference and WHR.
In line with our findings, studies by Möhlig et al.[38] and Brame et al.[39] have shown the inverse relation of adiponectin with fasting glucose. In support of our findings study suggests that adiponectin stimulates β-oxidation and glucose uptake in skeletal muscle via phosphorylation and activation of AMPK.[40] While in liver, adiponectin decreases gluconeogenesis by attenuating the expression levels of phosphoenolpyruvate carboxykinase and glucose 6-phosphatase, leading to reduced levels of glucose.[31] The acute glucose-lowering effect of adiponectin is mediated through activation of AMPK and transducer of regulated cAMP Response Element Binding CREB (CREB) activity-2. Adiponectin also activates PPAR-α, thereby stimulating fatty acid oxidation and decreasing triglycerides content in the liver.[41]
CONCLUSION
Our study showed a significant inverse association of serum adiponectin with obesity and lipid profile parameters except for serum HDL cholesterol level in Nepalese population as elsewhere.
ACKNOWLEDGMENTS
The authors would like to thank Nobel College and Kathmandu Model Hospital.
Footnotes
Source of Support: Nobel College
Conflict of Interest: None declared
REFERENCES
- 1.Garrow JS. Obesity and Related Diseases. London: Churchill Livingstone; 1988. pp. 1–16. [Google Scholar]
- 2.Kopelman PG. Obesity as a medical problem. Nature. 2000;404:635–43. doi: 10.1038/35007508. [DOI] [PubMed] [Google Scholar]
- 3.Swinburn BA, Sacks G, Hall KD, McPherson K, Finegood DT, Moodie ML, et al. The global obesity pandemic: Shaped by global drivers and local environments. Lancet. 2011;378:804–14. doi: 10.1016/S0140-6736(11)60813-1. [DOI] [PubMed] [Google Scholar]
- 4.Singh-Manoux A, Czernichow S, Elbaz A, Dugravot A, Sabia S, Hagger-Johnson G, et al. Obesity phenotypes in midlife and cognition in early old age: The Whitehall II cohort study. Neurology. 2012;79:755–62. doi: 10.1212/WNL.0b013e3182661f63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Burkhalter TM, Hillman CH. A narrative review of physical activity, nutrition, and obesity to cognition and scholastic performance across the human lifespan. Adv Nutr. 2011;2:201S–6. doi: 10.3945/an.111.000331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bray GA. Medical consequences of obesity. J Clin Endocrinol Metab. 2004;89:2583–9. doi: 10.1210/jc.2004-0535. [DOI] [PubMed] [Google Scholar]
- 7.Frayn KN, Karpe F, Fielding BA, Macdonald IA, Coppack SW. Integrative physiology of human adipose tissue. Int J Obes Relat Metab Disord. 2003;27:875–88. doi: 10.1038/sj.ijo.0802326. [DOI] [PubMed] [Google Scholar]
- 8.Ouchi N, Kihara S, Arita Y, Maeda K, Kuriyama H, Okamoto Y, et al. Novel modulator for endothelial adhesion molecules: Adipocyte-derived plasma protein adiponectin. Circulation. 1999;100:2473–6. doi: 10.1161/01.cir.100.25.2473. [DOI] [PubMed] [Google Scholar]
- 9.Kadowaki T, Yamauchi T, Kubota N, Hara K, Ueki K, Tobe K. Adiponectin and adiponectin receptors in insulin resistance, diabetes, and the metabolic syndrome. J Clin Invest. 2006;116:1784–92. doi: 10.1172/JCI29126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Chandran M, Phillips SA, Ciaraldi T, Henry RR. Adiponectin: More than just another fat cell hormone? Diabetes Care. 2003;26:2442–50. doi: 10.2337/diacare.26.8.2442. [DOI] [PubMed] [Google Scholar]
- 11.Rabe K, Lehrke M, Parhofer KG, Broedl UC. Adipokines and insulin resistance. Mol Med. 2008;14:741–51. doi: 10.2119/2008-00058.Rabe. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Weyer C, Funahashi T, Tanaka S, Hotta K, Matsuzawa Y, Pratley RE, et al. Hypoadiponectinemia in obesity and type 2 diabetes: Close association with insulin resistance and hyperinsulinemia. J Clin Endocrinol Metab. 2001;86:1930–5. doi: 10.1210/jcem.86.5.7463. [DOI] [PubMed] [Google Scholar]
- 13.Cruz M, García-Macedo R, García-Valerio Y, Gutiérrez M, Medina-Navarro R, Duran G, et al. Low adiponectin levels predict type 2 diabetes in Mexican children. Diabetes Care. 2004;27:1451–3. doi: 10.2337/diacare.27.6.1451. [DOI] [PubMed] [Google Scholar]
- 14.Daimon M, Oizumi T, Saitoh T, Kameda W, Hirata A, Yamaguchi H, et al. Decreased serum levels of adiponectin are a risk factor for the progression to type 2 diabetes in the Japanese Population: The Funagata study. Diabetes Care. 2003;26:2015–20. doi: 10.2337/diacare.26.7.2015. [DOI] [PubMed] [Google Scholar]
- 15.Krakoff J, Funahashi T, Stehouwer CD, Schalkwijk CG, Tanaka S, Matsuzawa Y, et al. Inflammatory markers, adiponectin, and risk of type 2 diabetes in the Pima Indian. Diabetes Care. 2003;26:1745–51. doi: 10.2337/diacare.26.6.1745. [DOI] [PubMed] [Google Scholar]
- 16.Hotta K, Funahashi T, Arita Y, Takahashi M, Matsuda M, Okamoto Y, et al. Plasma concentrations of a novel, adipose-specific protein, adiponectin, in type 2 diabetic patients. Arterioscler Thromb Vasc Biol. 2000;20:1595–9. doi: 10.1161/01.atv.20.6.1595. [DOI] [PubMed] [Google Scholar]
- 17.Balarajan Y, Villamor E. Nationally representative surveys show recent increases in the prevalence of overweight and obesity among women of reproductive age in Bangladesh, Nepal, and India. J Nutr. 2009;139:2139–44. doi: 10.3945/jn.109.112029. [DOI] [PubMed] [Google Scholar]
- 18.Australia, Melbourne: Health Communications; 2000. WHO/IASO/IOTF. The Asia-Pacific perspective: redefining obesity and its treatment. ISBN 0-9577082-1-1. Available from: http://www.who.int/nutrition/publications/bmi_asia_strategies.pdf . [Google Scholar]
- 19.Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972;18:499–502. [PubMed] [Google Scholar]
- 20.Yamamoto Y, Hirose H, Saito I, Tomita M, Taniyama M, Matsubara K, et al. Correlation of the adipocyte-derived protein adiponectin with insulin resistance index and serum high-density lipoprotein-cholesterol, independent of body mass index, in the Japanese population. Clin Sci (Lond) 2002;103:137–42. doi: 10.1042/cs1030137. [DOI] [PubMed] [Google Scholar]
- 21.Chan DC, Watts GF, Ng TW, Uchida Y, Sakai N, Yamashita S, et al. Adiponectin and other adipocytokines as predictors of markers of triglyceride-rich lipoprotein metabolism. Clin Chem. 2005;51:578–85. doi: 10.1373/clinchem.2004.045120. [DOI] [PubMed] [Google Scholar]
- 22.Tschritter O, Fritsche A, Thamer C, Haap M, Shirkavand F, Rahe S, et al. Plasma adiponectin concentrations predict insulin sensitivity of both glucose and lipid metabolism. Diabetes. 2003;52:239–43. doi: 10.2337/diabetes.52.2.239. [DOI] [PubMed] [Google Scholar]
- 23.Cnop M, Havel PJ, Utzschneider KM, Carr DB, Sinha MK, Boyko EJ, et al. Relationship of adiponectin to body fat distribution, insulin sensitivity and plasma lipoproteins: Evidence for independent roles of age and sex. Diabetologia. 2003;46:459–69. doi: 10.1007/s00125-003-1074-z. [DOI] [PubMed] [Google Scholar]
- 24.Martin LJ, Woo JG, Daniels SR, Goodman E, Dolan LM. The relationships of adiponectin with insulin and lipids are strengthened with increasing adiposity. J Clin Endocrinol Metab. 2005;90:4255–9. doi: 10.1210/jc.2005-0019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Schneider JG, von Eynatten M, Schiekofer S, Nawroth PP, Dugi KA. Low plasma adiponectin levels are associated with increased hepatic lipase activity in vivo. Diabetes Care. 2005;28:2181–6. doi: 10.2337/diacare.28.9.2181. [DOI] [PubMed] [Google Scholar]
- 26.Dichek HL, Brecht W, Fan J, Ji ZS, McCormick SP, Akeefe H, et al. Overexpression of hepatic lipase in transgenic mice decreases apolipoprotein B-containing and high density lipoproteins. Evidence that hepatic lipase acts as a ligand for lipoprotein uptake. J Biol Chem. 1998;273:1896–903. doi: 10.1074/jbc.273.4.1896. [DOI] [PubMed] [Google Scholar]
- 27.Geloneze B, Pereira JA, Pareja JC, Lima MM, Lazarin MA, Souza IC, et al. Overcoming metabolic syndrome in severe obesity: Adiponectin as a maker of insulin sensitivity and HDL-cholesterol improvements after gastric bypass. Arq Bras Endocrinol Metabol. 2009;53:293–300. doi: 10.1590/s0004-27302009000200022. [DOI] [PubMed] [Google Scholar]
- 28.Lara-Castro C, Fu Y, Chung BH, Garvey WT. Adiponectin and the metabolic syndrome: Mechanisms mediating risk for metabolic and cardiovascular disease. Curr Opin Lipidol. 2007;18:263–70. doi: 10.1097/MOL.0b013e32814a645f. [DOI] [PubMed] [Google Scholar]
- 29.Barter PJ, Puranik R, Rye KA. New insights into the role of HDL as an anti-inflammatory agent in the prevention of cardiovascular disease. Curr Cardiol Rep. 2007;9:493–8. doi: 10.1007/BF02938394. [DOI] [PubMed] [Google Scholar]
- 30.Szmitko PE, Teoh H, Stewart DJ, Verma S. Adiponectin and cardiovascular disease: State of the art? Am J Physiol Heart Circ Physiol. 2007;292:H1655–63. doi: 10.1152/ajpheart.01072.2006. [DOI] [PubMed] [Google Scholar]
- 31.Ouchi N, Kihara S, Arita Y, Okamoto Y, Maeda K, Kuriyama H, et al. Adiponectin, an adipocyte-derived plasma protein, inhibits endothelial NF-kappaB signaling through a cAMP-dependent pathway. Circulation. 2000;102:1296–301. doi: 10.1161/01.cir.102.11.1296. [DOI] [PubMed] [Google Scholar]
- 32.Wang Y, Xu A, Knight C, Xu LY, Cooper GJ. Hydroxylation and glycosylation of the four conserved lysine residues in the collagenous domain of adiponectin. Potential role in the modulation of its insulin-sensitizing activity. J Biol Chem. 2002;277:19521–9. doi: 10.1074/jbc.M200601200. [DOI] [PubMed] [Google Scholar]
- 33.Yamauchi T, Kamon J, Waki H, Imai Y, Shimozawa N, Hioki K, et al. Globular adiponectin protected ob/ob mice from diabetes and ApoE-deficient mice from atherosclerosis. J Biol Chem. 2003;278:2461–8. doi: 10.1074/jbc.M209033200. [DOI] [PubMed] [Google Scholar]
- 34.Shibata R, Sato K, Kumada M, Izumiya Y, Sonoda M, Kihara S, et al. Adiponectin accumulates in myocardial tissue that has been damaged by ischemia-reperfusion injury via leakage from the vascular compartment. Cardiovasc Res. 2007;74:471–9. doi: 10.1016/j.cardiores.2007.02.010. [DOI] [PubMed] [Google Scholar]
- 35.Tao L, Gao E, Jiao X, Yuan Y, Li S, Christopher TA, et al. Adiponectin cardioprotection after myocardial ischemia/reperfusion involves the reduction of oxidative/nitrative stress. Circulation. 2007;115:1408–16. doi: 10.1161/CIRCULATIONAHA.106.666941. [DOI] [PubMed] [Google Scholar]
- 36.Shibata R, Sato K, Pimentel DR, Takemura Y, Kihara S, Ohashi K, et al. Adiponectin protects against myocardial ischemia-reperfusion injury through AMPK- and COX-2-dependent mechanisms. Nat Med. 2005;11:1096–103. doi: 10.1038/nm1295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Mamaghani F, Zarghami N, Maleki MJ, Pourhassan-Moghaddam M, Hosseinpanah FC. Variation of adiponectin levels in normal and obese subjects: Possible correlation with lipid profiles. Int J Endocrinol Metab. 2009;3:170–8. [Google Scholar]
- 38.Möhlig M, Wegewitz U, Osterhoff M, Isken F, Ristow M, Pfeiffer AF, et al. Insulin decreases human adiponectin plasma levels. Horm Metab Res. 2002;34:655–8. doi: 10.1055/s-2002-38248. [DOI] [PubMed] [Google Scholar]
- 39.Brame LA, Considine RV, Yamauchi M, Baron AD, Mather KJ. Insulin and endothelin in the acute regulation of adiponectin in vivo in humans. Obes Res. 2005;13:582–8. doi: 10.1038/oby.2005.62. [DOI] [PubMed] [Google Scholar]
- 40.Yamauchi T, Kamon J, Minokoshi Y, Ito Y, Waki H, Uchida S, et al. Adiponectin stimulates glucose utilization and fatty-acid oxidation by activating AMP-activated protein kinase. Nat Med. 2002;8:1288–95. doi: 10.1038/nm788. [DOI] [PubMed] [Google Scholar]
- 41.Kadowaki T, Yamauchi T. Adiponectin and adiponectin receptors. Endocr Rev. 2005;26:439–51. doi: 10.1210/er.2005-0005. [DOI] [PubMed] [Google Scholar]