

Abstract
Sialectasis is an uncommon medical condition of the salivary glands. Conservative treatments of sialectasis include repeated aspiration, compression, dilation of the papilla and stent placement. This is the first reported case that we know of, using marsupialisation for distal sialectasis. Our case highlights the diagnostic and therapeutic challenges posed by sialectasis and demonstrates the efficacy of marsupialisation for distally based sialectasis when conservative treatments fail.
Background
Sialectasis is an uncommon condition of the salivary glands which involves dilation of a salivary duct. Ductal dilation is a chronic process and occurs most often secondary to obstruction by sialoliths, but may also be caused by strictures or stenosis. Additional reports suggest that masseter hypertrophy may also play an aetiological role.1 Most often, this condition affects the parotid gland and largely spares the submandibular gland. Idiopathic sialectasis of the Stensen's duct is extremely rare and there is very little in literature describing the aetiology and management of this condition. We present the case of a patient with idiopathic sialectasis of the Stensen's duct that was refractory to conservative treatment and effectively treated with intraoral marsupialisation.
Case presentation
A 43-year-old woman, with an 11-year history of a painless left-sided parotid mass, presented to our institution for evaluation. She noticed the mass incidentally during her first pregnancy and denied any preceding trauma, surgery, sialoliths, chronic parotitis or xerostomia. She reported that the mass would occasionally increase in size without any obvious cause and that the increase was not related to eating. The increase in size was associated with some discomfort, which was relieved with aggressive massage and compresses. She denied any history of erythema, warmth, fever, pain or other symptoms of infection at the site of the swelling. Her history included numerous therapeutic and diagnostic fine-needle aspiration (FNA), biopsies and imaging studies. She reported a significant decrease in the size of the mass after FNA was performed, but this did not completely relieve the swelling which would increase again at a later time.
Investigations
A physical examination revealed a large, 3 cm, intraoral palpable mass that was grossly visible on the external left cheek and submucosally intra-orally (figure 1). An in-office ultrasound corroborated our examination and revealed an anechoic mass with posterior acoustic enhancement which was present anterior to the masseter muscle. There was no obvious proximal ductal dilation of Stensen's duct or parotid gland inflammation. These findings were consistent with focal sialectasia of the left parotid duct. We attempted to pass a lacrimal probe through the papilla of left parotid duct into the fluid collection but were unable to cannulate the duct to any significant degree.
Figure 1.

Physical examination intraorally.
Differential diagnosis
The differential diagnosis is broad and can include sialocele, underlying sialolithiasis, stricture or mucus plugging. The diffuse form of sialectasis usually presents with a tube-like swelling in the cheek following the route of the Stensen's duct and may be diagnosed using sialography, ultrasonography and CT2 3 which will reveal a dilated Stensen's duct without any obvious cause of obstruction. The focal form of sialectasis may present with a soft ballotable facial mass with minimal proximal dilation of the affected duct.
Treatment
An in-office diagnostic sialoendoscopy using a 1.1 mm sialendoscope was performed and revealed a firm fixed stenosis in the distal aspect of the main parotid duct, approximately 1 cm into the ductal system. We attempted to place a guide wire through and dilate the stenosis, but could not with any reliability enter the cavity. We were able to drain a minimal amount of fluid into the oral cavity with external pressure after the procedure but the mass persisted. The patient returned to clinic 3 days later with symptoms of worsening cheek swelling, erythema, tenderness and excruciating pain in the left cheek. An FNA evacuated purulent material from the site of the swelling, and the patient was treated with oral clindamycin until her infective symptoms resolved. A follow-up MRI study revealed a well-defined cystic structure arising from the left Stensen's duct and continuing up to the second molar (figure 2).
Figure 2.
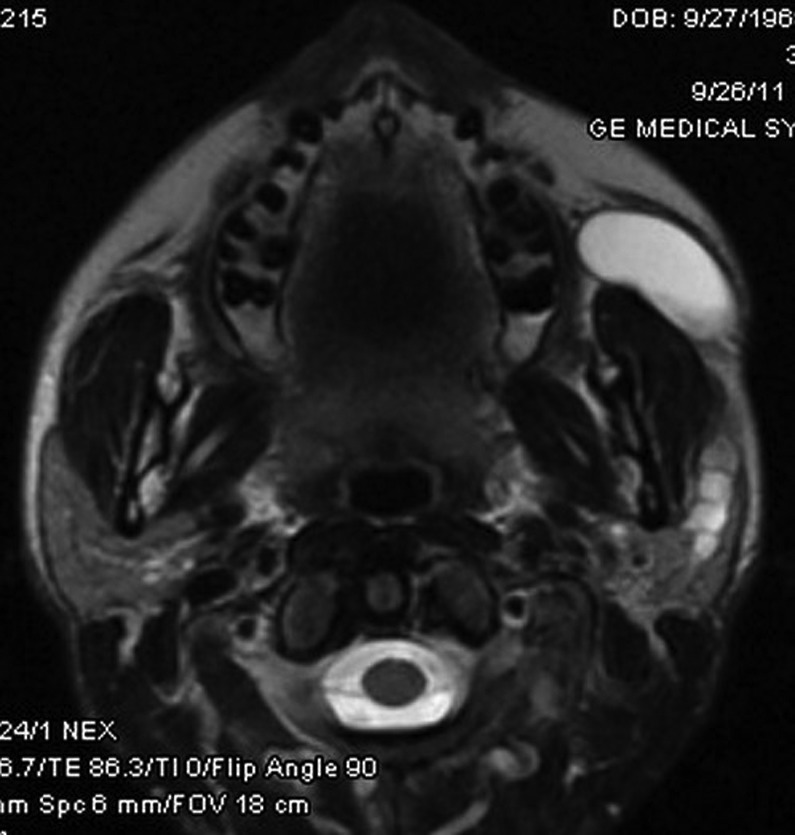
Sialectasis MRI.
After resolution of the infection, we decided to bring the patient to the operating room for marsupialisation of the fluid collection with salivary stent insertion under general anaesthesia. Once the mass was displaced anteriorly using bimanual pressure, submucosal tissue flaps were dissected superiorly and inferiorly to expose the collection. Interrupted sutures of 4–0 Vicryl were then placed from the buccal mucosal edge through the cyst wall anterior to posterior, to the superior flap as well as inferior flap in order to anchor the mass to the buccal mucosa. The mass was then entered through a horizontal incision and drained of saliva. Marsupialisation was then completed by suturing the anterior and posterior aspects of the cyst wall to the buccal mucosa. A 4 mm nasal endoscope was inserted into the cavity to confirm patency and a sterile nasopharyngeal airway was sutured into place with 3–0 prolene sutures in order to stent the opening (figure 3). The stent was removed on postoperative day 7.
Figure 3.

Nasal trumpet stent.
Outcome and follow-up
The patient had an unremarkable postoperative course without any recurrence of symptoms. She maintained normal facial nerve function throughout the course of this case. At 2.5 months after surgery the patient had some minor swelling of the cheek. Physical examination demonstrated mild stenosis of the neo-ostium, which was addressed by dilation under local anaesthesia with a tapered dilator. It is currently 2.5 years after marsupialisation and the patient is without concerns or issues.
Discussion
Focal sialectasis, which is defined as a dilation of a salivary duct, is a rare entity affecting the salivary glands. The disease process is thought to occur as a result of chronic obstruction with dilation. Repeated dilation can lead to a weakening of the ductal wall, which can be either focal or diffuse and results in permanent dilation and enlargement of the ductal calibre.
Conservative treatment of sialectasis—such as repeated aspiration, compression, dilation of the papilla and stent placement—may not result in the successful resolution of this condition. When conservative treatment fails—as in the case described here—a more aggressive surgical management may be indicated for distal sialectasis.
A search of the relevant literature does reveal a few reports of more aggressive management. In one case report, a patient who developed sialectasis of Stensen's duct following sialolithotomy underwent excision of the dilated portion of the duct with stent placement and suturing of the ductal orifice to the buccal mucosa with excellent postoperative results.4 A second case report described a similar procedure in a patient with idiopathic sialectasis with comparable results.5 Though both studies demonstrate the efficacy of duct excision, we believed that simple marsupialisation with large-calibre stenting would achieve equivalent results and that ductal resection was not necessary.
Beyond conservative treatment and marsupialisation, our surgical options included open ductal exploration and parotidectomy. These methods have all been described in the context of sialoceles that are secondary to sharp penetrating trauma.6 7 We felt that ductal exploration was not indicated in the case of our patient for several reasons. First, diagnostic sialoendoscopy allowed direct visualisation of the ductal system and revealed near complete stenosis, which could not be cannulated with the sialendoscope or a wire guide. We did not feel that creating a blind channel into the cyst with the sialendoscope would be safe given the risk of perforation through the duct and into the parenchyma. Second, MRI corroborated these findings and did not demonstrate ductal or parenchymal disruption, nor did it show evidence of inflammation that would indicate remote glandular tissue injury. Lastly, our patient denied any obvious trauma—specifically penetrating trauma—and had a relatively benign course with minimal symptoms. After considering these points, we concluded that open ductal exploration would be unnecessarily aggressive in this case.
A retrospective review of seven patients with congenital dilation of the Stensen's duct found superficial parotidectomy with excision of the Stensen's duct to be an effective method of treatment.8 We did not elect to perform a parotidectomy for this patient for several reasons. Both superficial and partial parotidectomies can be associated with sialocele formation when compared to complete or near complete parotidectomies.9 Additionally, superficial parotidectomy carries certain risks to the facial nerve as well as the great auricular nerve, with associated motor and sensory deficits, respectively. It was thought that there may be a significant risk of facial nerve injury, especially in the presence of inflammatory fibrosis of the gland and adhesion of the facial nerve to glandular tissue.8 Other potential complications of parotidectomy include Frey's syndrome and poor cosmetic scarring. After consideration of these risks, we decided that the benefits of a parotidectomy were not significant enough to warrant pursuing this as a treatment option.
In this particular case, the sialectasis was present at the anterior aspect of the masseter muscle and could be palpated intraorally. For this reason, we felt that marsupialisation would offer the best long-term solution to the patient’s problem and resolve the facial swelling without risks associated with open surgery. A more proximally located sialectasis would not be amenable to transoral marsupialisation given the poor access around the masseter muscle.
Learning points.
Idiopathic sialectasia of the parotid ductal system is a rare condition and can be challenging to treat, based on the location of the pathology.
Ultrasound examination can be combined with sialoendoscopy to provide a global picture of the salivary gland system, and can allow for effective treatment planning.
Compared to ductal exploration, marsupialisation is a minimally invasive and reliable procedure for treating sialectasis.
Footnotes
Contributors: ASJ contributed in conception and design or analysis and interpretation of the data, revising it critically for important intellectual content and finally approvingthe version to be published. SL contributed in analysis and interpretation of the data, revising it critically for important intellectual content and drafting the version to be published.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Shojaku H, Shojaku H, Shimizu M, et al. MR sialographic evaluation of sialectasia of Stensen's duct: comparison with X-ray sialography and ultrasonography. Radiat Med 2000;2013:143–5 [PubMed] [Google Scholar]
- 2.Mandel L. The grossly dilated Stensen's duct: case reports. J Oral Maxillofac Surg 2007;2013:2089–94 [DOI] [PubMed] [Google Scholar]
- 3.Ngu RK, Brown JE, Whaites EJ, et al. Salivary duct strictures: nature and incidence in benign salivary obstruction. Dentomaxillofac Radiol 2007;2013:63–7 [DOI] [PubMed] [Google Scholar]
- 4.Baurmash HD. Sialectasis of Stensen's duct with an extraoral swelling: a case report with surgical management. J Oral Maxillofac Surg 2007;2013:140–3 [DOI] [PubMed] [Google Scholar]
- 5.Yoon YH, Rha KS, Choi JW, et al. Sialectasis of Stensen's duct: an unusual cause of recurrent cheek swelling. Eur Arch Otorhinolaryngol 2009;2013:573–6 [DOI] [PubMed] [Google Scholar]
- 6.Lewkowicz AA, Hasson O, Nahlieli O. Traumatic injuries to the parotid gland and duct. J Oral Maxillofac Surg 2002;2013:676–80 [DOI] [PubMed] [Google Scholar]
- 7.Canosa A, Cohen MA. Post-traumatic parotid sialocele: report of two cases. J Oral Maxillofac Surg 1999;2013:742–5 [DOI] [PubMed] [Google Scholar]
- 8.Wang Y, Yu GY, Huang MX, et al. Diagnosis and treatment of congenital dilatation of Stensen's duct. CORD Conf Proc 2011;2013:1682–6 [DOI] [PubMed] [Google Scholar]
- 9.Witt RL. The incidence and management of siaolocele after parotidectomy. Otolaryngol Head Neck Surg 2009;2013:871–4 [DOI] [PubMed] [Google Scholar]