

Abstract
Background
Anterior cruciate ligament (ACL) deficiency alters 6 degrees of freedom knee kinematics, yet only anterior translation and internal rotation have been the primary measures in previous studies.
Purpose
To compare the 6 degrees of freedom knee kinematics and the graft forces after single- and double-bundle ACL reconstructions under various external loading conditions.
Study Design
Controlled laboratory study.
Methods
Ten human cadaveric knees were tested with a robotic testing system under 4 conditions: intact, ACL deficient, single-bundle reconstructed with a quadrupled hamstring tendon graft, and double-bundle reconstructed with 2 looped hamstring tendon grafts. Knee kinematics and forces of the ACL or ACL graft in each knee were measured under 3 loading conditions: an anterior tibial load of 134 N, a simulated quadriceps muscle load of 400 N, and combined tibial torques (10 N·m valgus and 5 N·m internal tibial torques) at 0°, 15°, 30°, 60°, and 90° of knee flexion.
Results
The double-bundle reconstruction restored the anterior and medial laxities closer to the intact knee than the single-bundle reconstruction. However, the internal rotation of the tibia under the simulated quadriceps muscle load was significantly decreased when compared with the intact knee after both reconstructions, more so after double-bundle reconstruction (P < .05). The entire graft force of the double-bundle reconstruction was more similar to that of the intact ACL than that of the single-bundle reconstruction. However, the posterolateral bundle graft in the double-bundle reconstructed knee was overloaded as compared with the intact posterolateral bundle.
Conclusion
The double-bundle reconstruction can better restore the normal anterior-posterior and medial-lateral laxities than the single-bundle reconstruction can, but an overloading of the posterolateral bundle graft can occur in a double-bundle reconstructed knee.
Clinical relevance
Both single-bundle and double-bundle techniques cannot restore the rotational laxities and the ACL force distributions of the intact knee.
Keywords: anterior cruciate ligament, reconstruction, single bundle, double bundle, kinematics
Double-bundle anterior cruciate ligament (ACL) reconstruction has been proposed to reproduce the 2 functional bundles of the ACL: anteromedial (AM) and posterolateral (PL).7,15,23,24,32 Despite in vitro and in vivo studies showing that double-bundle ACL reconstruction can better restore anteroposterior laxities of the intact knee,6,7,11,15,18,29,32 studies have reported no clinically significant difference between double- and single-bundle ACL reconstructions.14,24
In biomechanical studies using a robotic testing system, Petersen et al18 and Yagi et al30 indicated thata double-bundle reconstruction is able to more closely restore anterior laxity and graft forces to the intact level than the single-bundle reconstruction under an anterior tibial load. Seon et al22 also indicated that the double-bundle ACL reconstruction is more efficient in restoring anterior laxity than a single-bundle ACL reconstruction during an intraoperative evaluation. However, Markolf et al13 indicated that the double-bundle ACL reconstruction overly constrains the knee joint motion and that a single-bundle ACL reconstruction is sufficient to restore normal joint laxity. They also noted that the ACL graft in the double-bundle reconstruction carries higher force than the native ACL—especially, the PL bundle graft. A recent meta-analysis of randomized studies that compared the efficacy of double- and single-bundle ACL reconstructions found no clinically significant differences between the 2 types of ACL reconstructions in terms of anterior and rotational stabilities.14
Most of the biomechanical studies on ACL reconstruction focused on anterior laxity under an anterior tibial load or combined torques.11,18,30,31 Recent in vivo studies revealed that ACL deficiency and reconstruction affect not only anterior laxity but also medial-lateral laxity, which can alter the articular cartilage contact biomechanics.1,8,9,25 To objectively evaluate the efficacy of an ACL reconstruction, it is necessary to examine its effect on 6 degrees of freedom knee joint kinematics and graft forces under various external loads,33 especially under simulated physiologic loading conditions. A literature review indicated that no study has investigated the effect of double-bundle ACL reconstruction on the 6 degrees of freedom knee kinematics.
Therefore, the objective of this study was to compare the knee joint kinematics (anterior-posterior, internal-external, medial-lateral, and varus-valgus) and the graft forces under 3 external loading conditions after a single- and double-bundle ACL reconstruction. We hypothesized that the double-bundle ACL reconstruction can more closely restore the normal knee joint kinematics and ACL forces under various external loading conditions than the single-bundle ACL reconstruction.
MATERIALS AND METHODS
This study used 10 fresh-frozen cadaveric human knee specimens from 6 men and 4 women with an age range of 47 to 60 years. The specimens were stored at −20°C before the testing and were thawed at room temperature for 24 hours before the experiment. Specimens with history of ligament injury or previous surgery were excluded. Each knee was evaluated using a fluoroscopy and manual laxity test for arthritis and ACL injury. Specimens with either condition were eliminated from the study. We also visually inspected the intraarticular conditions through the medial parapatellar miniarthrotomy when we transected the ACL. Specimens with cartilage injury more than grade II of Outerbridge classification17 or with meniscal tears were excluded from this study. Eight specimens were used in another study.28 The femur and tibia were truncated approximately 25 cm from the joint line, with all the soft tissues around the knee intact (skin, knee ligaments, joint capsule, and musculature). To facilitate the fixation of the femur and tibia, musculature surrounding the shafts was stripped. The tibial and the femoral shafts were then secured in thick-walled aluminum cylinders using bone cement.
To study the knee biomechanics, we used a robotic testing system that can be operated under force and displacement control modes (Figure 1). Its operation has been detailed in several studies.9,18,33,34 During the experiment, we used the system to determine a passive flexion path of the ACL intact knee from 0° to 120° in 1° increments of knee flexion. A passive position is described as a position of the knee where all resultant forces and moments at the knee center were minimal (<5.0 N and <0.5 N·m, respectively). Kinematic responses of each knee were obtained at selected flexion angles of 0°, 15°, 30°, 60°, and 90° under 3 loading conditions: an anterior tibial load of 134 N, a simulated quadriceps load of 400 N, and combined torques of 10 N·m valgus and 5 N·m internal tibial torques. The quadriceps muscles were firmly attached to a rope via sutures and the rope was then passed through a pulley system mounted on the femoral clamp. To simulate quadriceps muscle load, weights (400 N) were hung on the free end of the rope9,10,33 (Figure 1). Under each knee condition, the robotic system applied a selected external load to the tibia while recording the kinematic responses and the forces in the knee joint.
Figure 1.
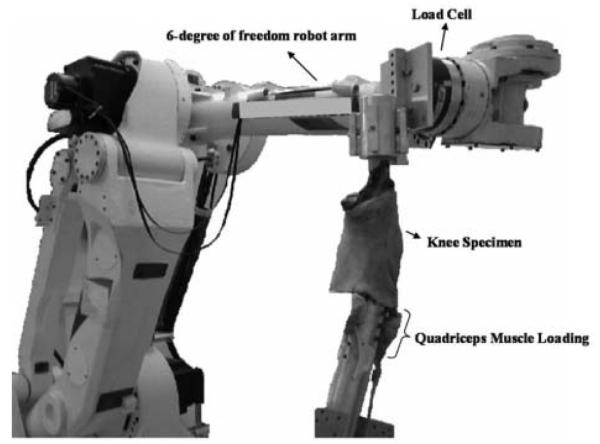
The robotic testing system with a cadaveric knee specimen installed.
The robotic testing system measures the forces experienced by the ACL and the ACL graft under the external loading conditions via the principle of superposition.21 To measure the forces, the AM and PL bundles were alternately transected at their femoral insertions through a 3-cm-long medial parapatellar miniarthrotomy at the level of the knee joint. After the transection of one bundle, the arthrotomy was repaired via sutures; the kinematics of the ACL intact knee were replayed; and the forces in the knee joint were measured. The forces in the transected bundle were calculated as the difference between the forces in the intact knee joint and the forces in the knee joint following the transection of a bundle. This procedure was repeated to measure the forces in the second bundle as well. After we determined the kinematics of the intact knee and the forces in the 2 bundles of the ACL, we tested the knee under the same loading conditions as the intact knee and measured the 6 degrees of freedom kinematics of the ACL-deficient knee.
Single-Bundle ACL Reconstruction
The ACL reconstruction was performed on the specimen while it was still installed on the robotic system. All the surgeries were performed using an arthroscopic-assisted technique by a single surgeon. The surgery began by harvesting the semitendinosus and gracilis tendons that served as the graft material for both ACL reconstructions. The graft was pretensioned on a graft preparation board (Mitek, Raynham, Massachusetts) with a 20-lb (9-kg) force. A K-wire for the tibial tunnel was placed at the center of the ACL footprint through the AM surface of the tibia at the level of the tibial tubercle via a tibial guide (Mitek) set at 55°. After 2 experienced sports surgeons confirmed a satisfactory position of the K-wire for the tunnel, the tibial tunnel was made by a cannulated reamer that matched the diameter of the prepared graft. To create the femoral tunnel, a K-wire was passed through the medial parapatellar miniarthrotomy with the knee flexed to 120° via a 6-mm offset guide (Mitek) and then placed at the 1:30 or 10:30 position, which corresponds to the center of the femoral footprint19,20 (Figure 2A). The femoral tunnel was initially reamed to the lateral cortex of the distal femur using a 4.5-mm EndoButton drill (Smith & Nephew Endoscopy, Andover, Massachusetts). Finally, a 30-mm long femoral socket was created by a cannulated reamer that matched the graft diameter. The quadrupled hamstring graft, consisting of looped semitendinosus and gracilis tendons, was then passed though the tibial tunnel into the joint and finally through the femoral socket and secured with an EndoButton CL (Smith & Nephew Endoscopy). The distal end of the graft was finally secured in the tibial tunnel by a tibial Intrafix system (Mitek) with 40 N of axial graft tension. After repairing the arthrotomy and the skin in layers by sutures, we determined kinematic responses and ACL graft force of the knee under the 3 loading conditions (anterior tibial load, simulated quadriceps muscle load, and combined torques).
Figure 2.

Schematic drawings of our surgical techniques including tunnel position in single-bundle (A) and double-bundle (B) anterior cruciate ligament reconstructions. AM, anteromedial; PL, posterolateral; C-ACL, center of anterior cruciate ligament; C-AM, center of anteromedial bundle; C-PM, center of posterolateral bundle.
Double-Bundle ACL Reconstruction
Before the double-bundle ACL reconstruction was performed, the tunnels of the single-bundle reconstruction were filled with bone cement, which facilitated in retesting of the same specimen for 2 ACL reconstructions. The hamstring tendons that were used for single-bundle ACL reconstruction were prepared as a looped semitendinosus graft for the AM bundle and a looped gracilis graft for the PL bundle. The double-bundle ACL reconstruction was performed by using a separate tunnel for each bundle on the tibia and femur.4,6,22,23 Two K-wires for the tibial tunnels were placed at the centers of the AM and PL bundle footprints as confirmed by 2 surgeons using a tibial guide (Mitek) set at 55° for the PL tunnel and at 45° for the AM tunnel. On the tibial cortex, the PL tunnel entry point started anterior to the superficial medial collateral ligament, and the AM tunnel started proximal and central from the PL tunnel entry point. After reaming the tibial tunnels with a cannulated reamer that matched the grafts diameters, we placed the femoral tunnels for the AM and PL bundles at the centers of their respective anatomical footprints through the parapatellar miniarthrotomy under arthroscopic guide using K-wires and cannulated reamers of the same size as the tibial tunnel diameters (Figure 2B). The PL and AM bundle grafts were passed through the tibial tunnels into the femoral tunnel and secured with 2 EndoButtons CL. After the fixation of the AM graft at 60° of flexion by an interference screw (Mitek) with a diameter that matched that of the tunnel with 20 N of axial graft tension, the PL graft was fixed at full extension with 20 N of axial graft tension using a 7-mm diameter interference screw in all cases. The arthrotomy and skin were then repaired by sutures, and the kinematics, entire ACL graft force, and AM and PL graft forces of the double-bundle reconstructed knee were determined using the same protocol as described in the intact knee. The figures showing the tunnel positions for the single- and double-bundle ACL reconstructions are presented in the appendix (available at http://ajs.sage-pub.com/supplemental/).
The study was designed for a within-subjects analysis of knee kinematics under the 4 conditions: intact, ACL deficient, single-bundle ACL reconstructed, and double-bundle ACL reconstructed. A 2-way repeated measures analysis of variance was used to detect statistically significant differences in the kinematic responses and the ACL or ACL graft forces of the knee under the different knee conditions at selected flexion angles. When significant differences were found, post hoc comparisons were made using the Student-Newman-Keuls test. Differences were considered statistically significant at P < .05.
RESULTS
Kinematics and Forces Under the Anterior Tibial Load
The anterior tibial translation of the ACL-deficient knee under the anterior tibial load was significantly greater than that of the intact knee at all selected flexion angles (P < .05) (Figure 3). The anterior tibial translations after single-bundle ACL reconstruction significantly improved when compared with the ACL-deficient knee at all selected flexion angles (P < .05). However, these anterior tibial translations after single-bundle ACL reconstruction were significantly greater than those of the intact knee at all selected flexion angles with a maximal difference of 4.2 ± 2.3 mm at 30° of flexion (P < .05) (Figure 3). After double-bundle reconstruction, anterior tibial translations were closely restored to the intact level at all selected flexion angles with a maximum difference of 1.6 ± 2.2 mm at 30° of flexion (P > .05). These translations were significantly different from those of the single-bundle ACL reconstructed knee at all selected flexion angles (P < .05) (Figure 3).
Figure 3.
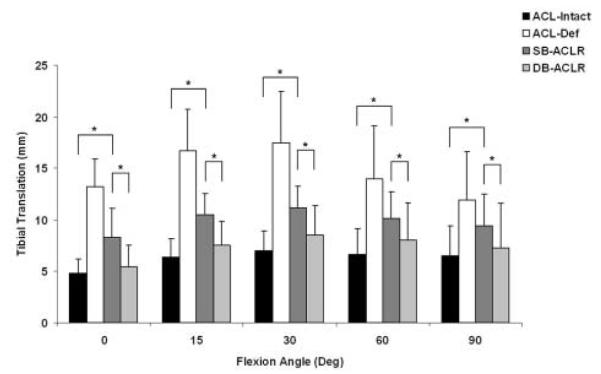
Anterior translation of the tibia under the anterior tibial load in the 4 conditions. The anterior cruciate ligament–deficient condition shows significant difference from the 3 other conditions at all angles. *P < .05. Error bars represent standard deviation. ACL, anterior cruciate ligament; def, deficient; SB, single bundle; DB, double bundle; ACLR, anterior cruciate ligament reconstruction.
Table 1 shows the entire forces of the intact ACL and ACL grafts of the single- and double-bundle reconstructions under the anterior tibial load. The average entire graft forces of the single-bundle ACL reconstruction were significantly lower than those of the intact knee at all selected flexion angles with a maximum difference of 55 ± 52 N at 15° of knee flexion (P < .05). On the contrary, the average entire ACL graft forces of the double-bundle reconstruction were not significantly different from those of the intact ACL at all selected flexion angles with a maximal difference of 29 ± 37 N at 30° of knee flexion (P > .05). Significant differences in the ACL graft forces of the single- and double-bundle ACL reconstruction were found at 0°, 15°, and 90° of knee flexion (P < .05). The forces in the AM bundle graft of the double-bundle reconstructed knee were significantly lower than those of the intact AM bundle at all selected flexion angles (P < .05), whereas, the PL bundle graft of the double-bundle reconstruction carried significantly higher forces than those of the intact PL bundle from 30° to 90° of flexion (P < .05).
TABLE 1.
Anterior Cruciate Ligament and Graft Forces (N) Under the 3 Loading Conditions at Select Flexion Anglesa
| Intact ACL |
SB ACLR |
DB ACLR |
||||||
|---|---|---|---|---|---|---|---|---|
| Loading Condition | Flexion Angle | Entire | AM | PL | Entire | Entire | AM Graft | PL Graft |
| Anterior tibial load | 0° | 146 ± 34 | 104 ± 45 | 48 ± 18 | 92 ± 36b | 123 ± 28c | 64 ± 30b | 74 ± 38 |
| 15° | 155 ± 41 | 119 ± 50 | 39 ± 25 | 100 ± 39b | 132 ± 21c | 75 ± 36b | 67 ± 33 | |
| 30° | 157 ± 44 | 139 ± 43 | 26 ± 17 | 109 ± 59b | 128 ± 36 | 84 ± 52b | 56 ± 28b | |
| 60° | 109 ± 40 | 105 ± 40 | 9 ± 7 | 63 ± 42b | 82 ± 22 | 57 ± 39b | 35 ± 22b | |
| 90° | 91 ± 34 | 89 ± 29 | 8 ± 6 | 44 ± 30b | 72 ± 28c | 60 ± 31b | 25 ± 17b | |
| Simulated quadriceps load | 0° | 91 ± 48 | 63 ± 38 | 39 ± 21 | 45 ± 31b | 60 ± 22b | 34 ± 21 | 37 ± 15 |
| 15° | 124 ± 54 | 85 ± 54 | 44 ± 34 | 55 ± 32b | 84 ± 38b | 36 ± 15b | 55 ± 26 | |
| 30° | 103 ± 49 | 73 ± 50 | 44 ± 40 | 47 ± 47b | 65 ± 37b | 22 ± 16b | 47 ± 26 | |
| 60° | 39 ± 33 | 32 ± 32 | 19 ± 10 | 17 ± 21b | 19 ± 13b | 7 ± 7b | 16 ± 9 | |
| 90° | 18 ± 19 | 16 ± 17 | 8 ±5 | 14 ± 11 | 17 ± 13 | 4 ± 2b | 16 ± 14 | |
| Combined tibial torques | 0° | 100 ± 44 | 68 ± 39 | 38 ± 22 | 68 ± 62 | 82 ± 43 | 27 ± 12b | 58 ± 43b |
| 30° | 109 ± 64 | 84 ± 49 | 31 ± 30 | 71 ± 48 | 91 ± 39 | 28 ± 18b | 67 ± 39b | |
ACL, anterior cruciate ligament; SB, single bundle; DB, double bundle; ACLR, ACL reconstruction; AM, anteromedial; PL, posterolateral.
Statistically significant difference compared with corresponding bundles of intact anterior cruciate ligament condition (P<.05).
Statistically significant difference compared with corresponding bundles of single-bundle anterior cruciate ligament reconstruction condition (P<.05).
Kinematics and Forces Under the Simulated Quadriceps Muscle Load
Under the simulated quadriceps muscle load, the anterior tibial translations of the ACL-deficient knee were significantly greater than those of the intact knee from 0° to 30° of flexion (P < .05) (Figure 4). These increased anterior translations of the tibia were significantly reduced after the single-bundle ACL reconstruction but not to the intact level (P < .05). The range of these differences between the anterior tibial translations of single-bundle ACL-reconstructed knee and the intact knee were 2.1 ± 1.8 mm at 0° to 3.1 ± 2.2 mm at 15° of flexion. The double-bundle ACL reconstruction reduced the anterior tibial translation of the ACL-deficient knee to the intact knee level at all selected flexion angles (P > .05). The anterior tibial translations after double-bundle reconstruction were significantly lower than after single-bundle reconstruction from 0° to 30° of flexion (P < .05) (Figure 4).
Figure 4.
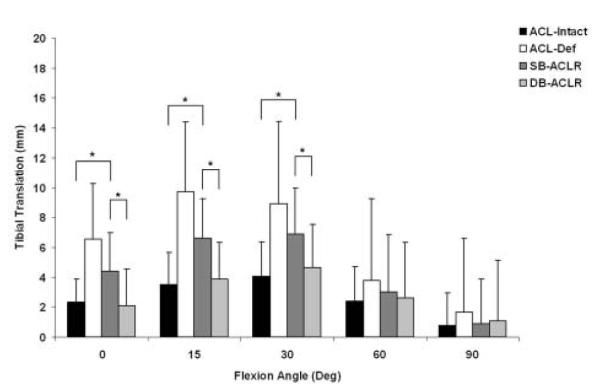
Anterior translation of the tibia under the simulated muscle load in the 4 conditions. The anterior cruciate ligament–deficient knee was significantly different from the other 3 conditions from 0° to 30°. *P < .05. Error bars represent standard deviation. ACL, anterior cruciate ligament; def, deficient; SB, single bundle; DB, double bundle; ACLR, anterior cruciate ligament reconstruction.
The ACL deficiency resulted in a medial shift of the tibia from 0° to 30° of flexion with a maximal difference of 0.8 ± 1.1 mm at 0° of flexion as compared with the ACL-intact knee (P < .05) (Table 2). Both single- and double-bundle ACL reconstructions reduced the increased medial shift of the ACL-deficient knee with no significant difference when compared to the intact knee (P > .05). However, on average, the double-bundle ACL reconstruction reduced the medial shift more than the single-bundle reconstruction with no significant difference between the 2 groups (P > .05). The internal tibial rotation under the simulated quadriceps muscle load significantly decreased after the single-bundle reconstruction as compared with intact knee at 15° of flexion (P < .05) (Figure 5). However, significantly less internal tibial rotation was observed after double-bundle ACL reconstruction from 0° to 30° of flexion as compared with the intact knee (P < .05). Furthermore, the double-bundle reconstruction showed significantly less internal rotation compared with the single-bundle reconstruction at 0° of flexion (P < .05). The ACL deficiency slightly increased valgus rotation under the simulated quadriceps muscle load as compared with the ACL-intact knee without any statistical significance at 0°, 30°, 60°, and 90° of flexion. The valgus rotations of the single- and double-bundle ACL reconstructions were similar to those of the intact knee at all selected flexion angles (P > .05) (Table 2).
TABLE 2.
Kinematic Responses of the Tibia Under the Simulated Quadriceps Muscle Load in 4 Conditionsa
| Flexion Angle | Intact ACL | Deficient ACL | SB ACLR | DB ACLR | |
|---|---|---|---|---|---|
| Medial (+) / lateral (−) mm | 0° | 0.1 ± 0.6 | 0.9 ± 1.3b | 0.5 ± 1.3 | −0.1 ± 0.9c,d |
| 15° | 0.6 ± 0.9 | 1.4 ± 2.7 | 0.9 ± 1.9 | 0.2 ± 1.2c | |
| 30° | 0.6 ± 1.3 | 0.9 ± 3.5 | 0.8 ± 2.5 | 0.2 ± 1.7 | |
| 60° | 0.3 ± 1.3 | 0.2 ± 2.0 | 0.4 ± 1.7 | 0.3 ± 1.2 | |
| 90° | 0.1 ± 0.6 | 0.1 ± 0.8 | 0.1 ± 0.8 | 0.03 ± 0.5 | |
| Valgus (+) / varus (−) ° | 0° | 0.4 ± 0.7 | 0.5 ± 1.0 | 0.6 ± 0.9 | 0.1 ± 0.9d |
| 15° | 1.3 ± 0.8 | 2.0 ± 1.8b | 1.9 ± 1.4b | 1.2 ± 1.1c,d | |
| 30° | 1.7 ± 1.1 | 2.2 ± 1.8 | 2.4 ± 1.8 | 1.7 ± 1.4d | |
| 60° | 1.2 ± 0.7 | 1.5 ± 1.3 | 1.5 ± 1.0 | 1.3 ± 0.9 | |
| 90° | 0.8 ± 0.6 | 1.1 ± 1.4 | 1.0 ± 0.7 | 1.0 ± 1.0 |
ACL, anterior cruciate ligament; SB, single bundle; DB, double bundle; ACLR, ACL reconstruction.
Statistically significant difference compared with intact anterior cruciate ligament condition (P<.05).
Statistically significant difference compared with anterior cruciate ligament-deficient condition (P<.05).
Statistically significant difference compared with single-bundle anterior cruciate ligament reconstruction condition (P<.05).
Figure 5.
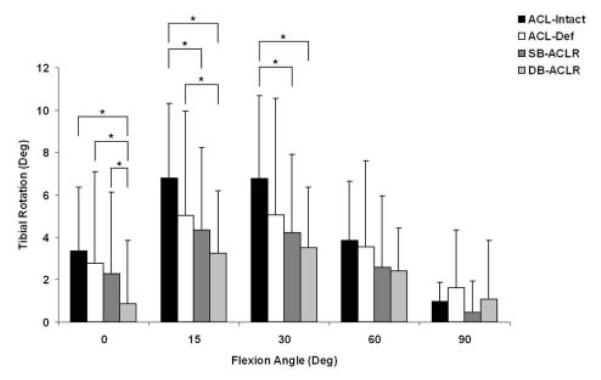
Internal rotations of the tibia under the muscle load in the 4 conditions. *P < .05. Error bars represent standard deviation. ACL, anterior cruciate ligament; def, deficient; SB, single bundle; DB, double bundle; ACLR, anterior cruciate ligament reconstruction.
Under the simulated muscle load, the single- and double-bundle reconstructions resulted in significantly lower ACL graft forces than those of the intact ACL from 0° to 60° of flexion (P < .05) (Table 1). In the double-bundle reconstructed knees, the forces in the AM graft were significantly lower than those of the intact AM bundle from 15° to 90° of knee flexions, but the forces in the PL graft were similar to those of the intact PL bundle at all selected flexion angles (P > .05) (Table 1).
Kinematics and Forces Under Combined Valgus and Internal Tibial Torques
In response to the combined torques, the anterior tibial translation of the ACL-deficient knee significantly increased when compared with the intact knee by 3.5 ± 2.5 mm at 0° of flexion and 3.7 ± 3.0 mm at 30° (P < .05) (Table 3). The anterior tibial translation of the single-bundle ACL reconstruction was significantly greater than that of the intact knee at 0° and 30° of flexion (P < .05). The double-bundle ACL reconstruction restored the anterior tibial translation to the intact level at both 0° and 30° of flexion (P > .05). The internal tibial rotations of the single- and double-bundle reconstructions were similar to those of the intact knee at 0° and 30° of flexion (P > .05) (Table 3). However, the double-bundle reconstruction showed significantly less internal rotation than the single-bundle reconstruction and ACL-deficient knee at 0° of flexion (P < .05).
TABLE 3.
Kinematic Responses of the Tibia Under Combined Valgus and Internal Torques in 4 Conditions
| Flexion Angle | Intact ACL | Deficient ACL | SB ACLR | DB ACLR | |
|---|---|---|---|---|---|
| Anterior (+) / posterior (−) mm | 0° | −0.1 ± 2.4 | 3.3 ± 4.6b | 2.0 ± 3.7b,c | 0.6 ± 3.1c,d |
| 30° | 0.8 ± 3.5 | 4.5 ± 6.0b | 3.1 ± 4.4b | 1.4 ± 3.9c,d | |
| Internal (+) / external (−) ° | 0° | 11.1 ± 4.0 | 13.0 ± 5.0 | 12.7 ± 5.2 | 9.9 ± 4.5c,d |
| 30° | 19.2 ± 6.1 | 19.5± 6.9 | 19.1 ± 6.7 | 18.2 ± 6.1 |
ACL, anterior cruciate ligament; SB, single bundle; DB, double bundle; ACLR, ACL reconstruction.
Statistically significant difference compared with intact anterior cruciate ligament condition (P<.05).
Statistically significant difference compared with deficient anterior cruciate ligament condition (P<.05).
Statistically significant difference compared with single-bundle anterior cruciate ligament reconstruction condition (P<.05).
No significant differences were found between the forces of the intact ACL and the forces in the ACL grafts of the single- and double-bundle ACL reconstructions at 0° and 30° of flexion (P > .05) (Table 1). However, the PL graft of the double-bundle reconstruction showed significantly higher forces and the AM graft showed significantly lower forces than those of corresponding bundles of the intact knee at 0° and 30° of knee flexions (P < .05) (Table 1).
DISCUSSION
In this study, we compared the tibial translations, rotation kinematics, and graft forces of the knee after single- and double-bundle ACL reconstructions with those of the intact knee using cadaveric specimens under 3 external loads. The double-bundle ACL reconstruction was able to more closely restore the anterior and medial tibial translations of the intact knees than the single-bundle ACL reconstruction, but it more overly constrained the internal tibial rotation of the knee joint. Even though the entire ACL graft forces of the double-bundle ACL reconstruction were closer to those of the intact knee than the single-bundle ACL reconstruction, the PL graft of the double-bundle ACL reconstruction had significantly higher forces than those of the intact PL bundle.
Consistent with other studies that compared the knee kinematics between the single- and double-bundle reconstructions under the anterior tibial or combined torques,11,13,29-31 this study demonstrated that single-bundle ACL reconstruction improved the anterior tibial translations of an ACL-deficient knee at all flexion angles to a clinically satisfactory level but could not restore them to the intact level. However, the double-bundle ACL reconstruction restored the anterior tibial translations to the intact knee level at all selected flexion angles under the anterior tibial load and combined torques, as reported in published studies.18,30,31 Mae et al11 and Markolf et al13 reported, however, that the double-bundle ACL reconstruction over-corrected the anterior tibial translation when compared with the intact and single-bundle reconstructed knees. The discrepancy between these studies may be due to the differences in the surgical techniques and initial graft-tensioning protocols used. Mae et al11 used a single tibial tunnel and fixed both the grafts at the same flexion angle (30°) for the double-bundle ACL reconstruction. Markolf et al13 tensioned the AM graft to restore the anterior translation to within 1 mm of the intact knee at 30° of flexion and then tensioned the PL graft with either the same force as in the AM graft or 30 N of additional tension than that used for the AM graft. In our study, we used 40 N of initial graft tension for the single-bundle ACL reconstruction and 20 N of initial tension for each graft in the double-bundle ACL reconstruction. We fixed the 2 grafts at different flexion angles (AM at 60° and PL at 0°) by a commonly used protocol in the literature.4,6,23 However, further investigations into double-bundle ACL reconstruction are necessary to achieve optimal graft fixation angle and initial tension to restore normal knee kinematics.
The amount of internal tibial rotation of the ACL-deficient knee and single- and double-bundle ACL-reconstructed knees was not significantly different from that of the intact knee under the combined torques. These results are comparable with those of previous studies.3,5 The double-bundle ACL reconstruction caused an overconstraint in internal tibial rotation under the combined torques as compared with the single-bundle reconstruction at 0° of flexion. However, the magnitudes of differences in the internal tibial rotation among all the knee conditions were less than 3.5°. These data suggest that combined torques may not be an efficient loading to evaluate the axial rotational efficacy of an ACL reconstruction.
Quadriceps muscle load can produce anterior tibial translation and internal tibial rotation from 0° to 30° of flexion.9,33 Therefore, the simulated physiological loading condition could be an effective method to evaluate the efficacy of various ACL reconstructions. In this study, when compared with the single-bundle reconstruction, the double-bundle reconstruction closely restored the anterior tibial translation under the simulated quadriceps muscle load to the intact knee level. Anterior cruciate ligament deficiency caused a decrease in internal tibial rotation as compared with the intact knee condition. Owing to the complex interdependence of 6 degrees of freedom kinematics, we could not precisely identify the cause of this decrease in the internal tibial rotation. This overconstraint may have been an attribute of the coupled motions observed during the simulated quadriceps muscle loading. Similar to the ACL-deficient condition, the single-bundle ACL reconstruction in our study significantly reduced the internal tibial rotation under the simulated quadriceps muscle load as compared with the intact knee. These decreases in the internal tibial rotations following single-bundle ACL reconstruction are consistent with reports in the literature.2,12,25,26,33 The double-bundle ACL reconstruction overconstrained the internal tibial rotation as well but more so than single-bundle reconstruction, especially at low flexion angles. Overconstraint of tibial internal rotation after an ACL reconstruction could be caused by various factors, such as the amount of initial graft tension, as well as the tunnel locations.2,12 The altered rotational kinematics may cause loading of the articular cartilage at abnormal locations. Further studies should quantify the effect of ACL reconstruction on the cartilage contact pressure. These findings indicate that an optimal tensioning protocol and tunnel location may be needed to improve the observed overconstraint of internal tibial rotation while still maintaining the efficiency in restoration of anterior tibial translation.
It is well known that ACL deficiency alters not only the anterior translation and internal rotation but also the medial-lateral translation and varus-valgus rotations.8,9 However, no studies have quantified the medial-lateral or varus-valgus kinematics after the single- and double-bundle ACL reconstructions. In this study, we noted that the ACL-deficient knee resulted in a medial shift of the tibia from 0° to 30° of flexion under the muscle load. This shift was better restored by the double-bundle reconstruction than the single-bundle reconstruction. These results suggest that double-bundle ACL reconstruction may have an advantage over single-bundle ACL reconstruction to restore the medial-lateral translation under the physiologic quadriceps muscle load. Such restoration of normal knee kinematics may reduce alterations in the normal cartilage contact locations in the joint due to the altered medial-lateral kinematics.9
Our data demonstrate that the entire graft forces of double-bundle ACL reconstruction are more similar to those of the intact knee than single-bundle ACL reconstruction under all 3 loading conditions, which is consistent with studies in the literature.27,30 However, our force data of the individual bundles show that the PL and AM grafts of the double-bundle reconstruction carry significantly higher and lower forces, respectively, than do the corresponding individual bundles of the intact knee. Consistent with this study is that by Markolf et al,13 who also reported an overloading of the PL graft and its failure at 0° of flexion. The high forces of the PL graft in the double-bundle reconstruction may be a cause of the rupture of the PL graft in the clinical setting, which has been reported.16 These data suggest that the PL graft may need to be fixed with a lower initial tension (<20 N) to prevent overloading of the PL graft and its failure.
The current study has its limitations. We did not evaluate the effect of different graft tensions and graft fixation angles. However, the grafts for both reconstructions were fixed on the basis of commonly used tension and fixation angle protocols in the clinical setting.4,6,23 Future studies should investigate the effect of initial graft tension and fixation angles in the double-bundle ACL reconstruction on the knee kinematics and graft forces. Second, we filled the tunnels that were created for the single-bundle ACL reconstruction with bone cement for the subsequent double-bundle ACL reconstruction, which enabled us to use the same specimens to test both reconstruction techniques. Other studies have used this protocol, and it has been demonstrated to have no significant effect on the outcomes.18,30,34 Tunnel location may affect the kinematic responses of the knee. In this study, we used a tunnel placed at the 10:30 position for our single-bundle ACL reconstruction, and we did not evaluate the efficacy of ACL reconstruction with different tunnel locations. Although this position is commonly used in the clinical setting, more investigation is needed to determine the tunnel position that can achieve optimal outcomes. This is also a time-zero study, and no graft-tunnel healing has been considered. Future studies should investigate the effect of double-bundle ACL reconstruction on the knee kinematics and graft forces of patients during daily functional activities. We measured the knee kinematics and forces of the ACL and ACL grafts from 0° to 90° of flexion; therefore, we could not evaluate the possible posterior cruciate ligament impingement that may occur beyond 90° of flexion. Finally, owing to the limitations of the robotic testing system, we could not completely achieve the high physiological loads and hence evaluate the efficacy of the reconstructions at these large loads. Nonetheless, the sub-physiological loading provided us with some valuable trends and critical information for the progression of ACL reconstruction.
In summary, we found that the double-bundle ACL reconstruction can more closely restore the anterior and medial knee laxities of the intact knee than the single-bundle ACL reconstruction under different external loads. However, both ACL reconstructions overconstrained the internal tibial rotation—especially, the double-bundle reconstruction at low flexion angles under simulated quadriceps muscle load. Although the ACL graft forces in double-bundle reconstruction were closer to the intact ACL forces than the ACL graft forces of the single-bundle reconstruction, the double-bundle reconstruction may overload the PL graft, which could cause a graft failure. Therefore, to improve the double-bundle ACL reconstruction, the tensioning strategy of the AM and PL bundles may need to be investigated to restore normal knee kinematics and graft forces.
Supplementary Material
Acknowledgments
One or more authors has declared a potential conflict of interest: Support was received from the National Institutes of Health (R01AR055612), the Department of Orthopaedic Surgery of Massachusetts General Hospital, and DePuy Mitek, Raynham, Massachusetts.
REFERENCES
- 1.Andriacchi TP, Briant PL, Bevill SL, Koo S. Rotational changes at the knee after ACL injury cause cartilage thinning. Clin Orthop Relat Res. 2006;442:39–44. doi: 10.1097/01.blo.0000197079.26600.09. [DOI] [PubMed] [Google Scholar]
- 2.Brady MF, Bradley MP, Fleming BC, Fadale PD, Hulstyn MJ, Banerjee R. Effects of initial graft tension on the tibiofemoral compressive forces and joint position after anterior cruciate ligament reconstruction. Am J Sports Med. 2007;35(3):395–403. doi: 10.1177/0363546506294363. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Diermann N, Schumacher T, Schanz S, Raschke MJ, Petersen W, Zantop T. Rotational instability of the knee: internal tibial rotation under a simulated pivot shift test. Arch Orthop Trauma Surg. 2009;129(3):353–358. doi: 10.1007/s00402-008-0681-z. [DOI] [PubMed] [Google Scholar]
- 4.Fu FH, Shen W, Starman JS, Okeke N, Irrgang JJ. Primary anatomic double-bundle anterior cruciate ligament reconstruction: a preliminary 2-year prospective study. Am J Sports Med. 2008;36(7):1263–1274. doi: 10.1177/0363546508314428. [DOI] [PubMed] [Google Scholar]
- 5.Gadikota HR, Seon JK, Kozanek M, et al. Biomechanical comparison of single-tunnel-double-bundle and single-bundle anterior cruciate ligament reconstructions. Am J Sports Med. 2009;37(5):962–969. doi: 10.1177/0363546508330145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Jarvela T. Double-bundle versus single-bundle anterior cruciate ligament reconstruction: a prospective, randomize clinical study. Knee Surg Sports Traumatol Arthrosc. 2007;15(5):500–507. doi: 10.1007/s00167-006-0254-z. [DOI] [PubMed] [Google Scholar]
- 7.Kondo E, Yasuda K, Azuma H, Tanabe Y, Yagi T. Prospective clinical comparisons of anatomic double-bundle versus single-bundle anterior cruciate ligament reconstruction procedures in 328 consecutive patients. Am J Sports Med. 2008;36(9):1675–1687. doi: 10.1177/0363546508317123. [DOI] [PubMed] [Google Scholar]
- 8.Li G, Moses JM, Papannagari R, et al. Anterior cruciate ligament deficiency alters the in vivo motion of the tibiofemoral cartilage contact points in both the anteroposterior and mediolateral directions. J Bone Joint Surg Am. 2006;88(8):1826–1834. doi: 10.2106/JBJS.E.00539. [DOI] [PubMed] [Google Scholar]
- 9.Li G, Papannagari R, DeFrate LE, Yoo JD, Park SE, Gill TJ. The effects of ACL deficiency on mediolateral translation and varusvalgus rotation. Acta Orthop. 2007;78(3):355–360. doi: 10.1080/17453670710013924. [DOI] [PubMed] [Google Scholar]
- 10.Li G, Rudy TW, Sakane M, Kanamori A, Ma CB, Woo SL. The importance of quadriceps and hamstring muscle loading on knee kinematics and in-situ forces in the ACL. J Biomech. 1999;32(4):395–400. doi: 10.1016/s0021-9290(98)00181-x. [DOI] [PubMed] [Google Scholar]
- 11.Mae T, Shino K, Miyama T, et al. Single- versus two-femoral socket anterior cruciate ligament reconstruction technique: biomechanical analysis using a robotic simulator. Arthroscopy. 2001;17(7):708–716. doi: 10.1053/jars.2001.25250. [DOI] [PubMed] [Google Scholar]
- 12.Mae T, Shino K, Nakata K, Toritsuka Y, Otsubo H, Fujie H. Optimization of graft fixation at the time of anterior cruciate ligament reconstruction, part I: effect of initial tension. Am J Sports Med. 2008;36(6):1087–1093. doi: 10.1177/0363546508314433. [DOI] [PubMed] [Google Scholar]
- 13.Markolf KL, Park S, Jackson SR, McAllister DR. Anterior-posterior and rotatory stability of single and double-bundle anterior cruciate ligament reconstructions. J Bone Joint Surg Am. 2009;91(1):107–118. doi: 10.2106/JBJS.G.01215. [DOI] [PubMed] [Google Scholar]
- 14.Meredick RB, Vance KJ, Appleby D, Lubowitz JH. Outcome of single-bundle versus double-bundle reconstruction of the anterior cruciate ligament: a meta-analysis. Am J Sports Med. 2008;36(7):1414–1421. doi: 10.1177/0363546508317964. [DOI] [PubMed] [Google Scholar]
- 15.Muneta T, Koga H, Mochizuki T, et al. A prospective randomized study of 4-strand semitendinosus tendon anterior cruciate ligament reconstruction comparing single-bundle and double-bundle techniques. Arthroscopy. 2007;23(6):618–628. doi: 10.1016/j.arthro.2007.04.010. [DOI] [PubMed] [Google Scholar]
- 16.Otsubo H, Shino K, Nakamura N, Nakata K, Nakagawa S, Koyanagi M. Arthroscopic evaluation of ACL grafts reconstructed with the anatomical two-bundle technique using hamstring tendon autograft. Knee Surg Sports Traumatol Arthrosc. 2007;15(6):720–728. doi: 10.1007/s00167-006-0274-8. [DOI] [PubMed] [Google Scholar]
- 17.Outerbridge RE. The etiology of chondromalacia patellae. J Bone Joint Surg Br. 1961;43:752–757. doi: 10.1302/0301-620X.43B4.752. [DOI] [PubMed] [Google Scholar]
- 18.Petersen W, Tretow H, Weimann A, et al. Biomechanical evaluation of two techniques for double-bundle anterior cruciate ligament reconstruction: one tibial tunnel versus two tibial tunnels. Am J Sports Med. 2007;35(2):228–234. doi: 10.1177/0363546506294468. [DOI] [PubMed] [Google Scholar]
- 19.Rue JP, Ghodadra N, Bach BR., Jr Femoral tunnel placement in single-bundle anterior cruciate ligament reconstruction: a cadaveric study relating transtibial lateralized femoral tunnel position to the anteromedial and posterolateral bundle femoral origins of the anterior cruciate ligament. Am J Sports Med. 2008;36(1):73–79. doi: 10.1177/0363546507311093. [DOI] [PubMed] [Google Scholar]
- 20.Rue JP, Lewis PB, Parameswaran AD, Bach BR., Jr Single-bundle anterior cruciate ligament reconstruction: technique overview and comprehensive review of results. J Bone Joint Surg Am. 2008;90(suppl 4):67–74. doi: 10.2106/JBJS.H.00651. [DOI] [PubMed] [Google Scholar]
- 21.Sakane M, Fox RJ, Woo SL, Livesay GA, Li G, Fu FH. In situ forces in the anterior cruciate ligament and its bundles in response to anterior tibial loads. J Orthop Res. 1997;15(2):285–293. doi: 10.1002/jor.1100150219. [DOI] [PubMed] [Google Scholar]
- 22.Seon JK, Park SJ, Lee KB, Yoon TR, Seo HY, Song EK. Stability comparison of anterior cruciate ligament between double- and single-bundle reconstructions. Int Orthop. 2009;33(2):425–429. doi: 10.1007/s00264-008-0530-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Siebold R, Dehler C, Ellert T. Prospective randomized comparison of double-bundle versus single-bundle anterior cruciate ligament reconstruction. Arthroscopy. 2008;24(2):137–145. doi: 10.1016/j.arthro.2007.11.013. [DOI] [PubMed] [Google Scholar]
- 24.Streich NA, Friedrich K, Gotterbarm T, Schmitt H. Reconstruction of the ACL with a semitendinosus tendon graft: a prospective randomized single blinded comparison of double-bundle versus single-bundle technique in male athletes. Knee Surg Sports Traumatol Arthrosc. 2008;16(3):232–238. doi: 10.1007/s00167-007-0480-z. [DOI] [PubMed] [Google Scholar]
- 25.Tashman S, Collon D, Anderson K, Kolowich P, Anderst W. Abnormal rotational knee motion during running after anterior cruciate ligament reconstruction. Am J Sports Med. 2004;32(4):975–983. doi: 10.1177/0363546503261709. [DOI] [PubMed] [Google Scholar]
- 26.Tashman S, Kolowich P, Collon D, Anderson K, Anderst W. Dynamic function of the ACL-reconstructed knee during running. Clin Orthop Relat Res. 2007;454:66–73. doi: 10.1097/BLO.0b013e31802bab3e. [DOI] [PubMed] [Google Scholar]
- 27.Wu C, Noorani S, Vercillo F, Woo SL. Tension patterns of the anteromedial and posterolateral grafts in a double-bundle anterior cruciate ligament reconstruction. J Orthop Res. 2009;27(7):879–884. doi: 10.1002/jor.20822. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Wu JL, Seon JK, Gadikota HR, et al. In situ forces in the anteromedial and posterolateral bundles of the anterior cruciate ligament under simulated functional loading conditions. Am J Sports Med. 2010;38(3):558–563. doi: 10.1177/0363546509350110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Yagi M, Kuroda R, Nagamune K, Yoshiya S, Kurosaka M. Double-bundle ACL reconstruction can improve rotational stability. Clin Orthop Relat Res. 2007;454:100–107. doi: 10.1097/BLO.0b013e31802ba45c. [DOI] [PubMed] [Google Scholar]
- 30.Yagi M, Wong EK, Kanamori A, Debski RE, Fu FH, Woo SL. Biomechanical analysis of an anatomic anterior cruciate ligament reconstruction. Am J Sports Med. 2002;30(5):660–666. doi: 10.1177/03635465020300050501. [DOI] [PubMed] [Google Scholar]
- 31.Yamamoto Y, Hsu WH, Woo SL, Van Scyoc AH, Takakura Y, Debski RE. Knee stability and graft function after anterior cruciate ligament reconstruction: a comparison of a lateral and an anatomical femoral tunnel placement. Am J Sports Med. 2004;32(8):1825–1832. doi: 10.1177/0363546504263947. [DOI] [PubMed] [Google Scholar]
- 32.Yasuda K, Kondo E, Ichiyama H, Tanabe Y, Tohyama H. Clinical evaluation of anatomic double-bundle anterior cruciate ligament reconstruction procedure using hamstring tendon grafts: comparisons among 3 different procedures. Arthroscopy. 2006;22(3):240–251. doi: 10.1016/j.arthro.2005.12.017. [DOI] [PubMed] [Google Scholar]
- 33.Yoo JD, Papannagari R, Park SE, DeFrate LE, Gill TJ, Li G. The effect of anterior cruciate ligament reconstruction on knee joint kinematics under simulated muscle loads. Am J Sports Med. 2005;33(2):240–246. doi: 10.1177/0363546504267806. [DOI] [PubMed] [Google Scholar]
- 34.Zantop T, Diermann N, Schumacher T, Schanz S, Fu FH, Petersen W. Anatomical and nonanatomical double-bundle anterior cruciate ligament reconstruction: importance of femoral tunnel location on knee kinematics. Am J Sports Med. 2008;36(4):678–685. doi: 10.1177/0363546508314414. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.