

Abstract
Background:
With objective of health systems strengthening, as visualized under National Rural Health Mission (NRHM); one key strategic intervention is up-gradation of health service delivery facilities so as to provide sustainable quality care with accountability and people's participation, which required the development of a proper management structure called Rogi Kalyan Samitis (RKS). It is the State's attempt to make health everyone's business by de-mystifying health-care delivery at district and sub-district levels with reference to facility based health-care delivery by encouraging citizen's participation in management bodies.
Objective:
The study was an attempt to define ‘functional Health Systems’ with a focus on strategic issues concerning RKS operations.
Materials and Methods:
A mixed-method, multi-site, collective case study approach was adopted. In-depth interviews of key-stakeholders were conducted. Qualitative data were analyzed thematically and coded inductively.
Results:
RKS is yet to bring out quality component to the health services being provided through facilities. This can be attributed to structural and managerial weakness in the system; however, certainly NRHM has been consistent in creating a road-map for benefitting local community and their participation through RKS.
Conclusion:
The progress of the RKS can further be enhanced by giving due priority to critical areas. Furthermore, the results emphasize an urgent need for devising strategies and actions to overcome significant systemic constraints as highlighted in the present study.
Keywords: Accountability, health everyone's business, health systems, mixed-method, people's participation, Rogi Kalyan Samitis, structural and managerial weakness
Introduction
Health sector reform under the National Rural Health Mission (NRHM), aims at increasing functional, administrative and financial autonomy of various field units.(1) Under NRHM, up-gradation of health service delivery facilities for better community participation and accountability is strategized as a vehicle of flexible funding by the government to help raise the quality of care, by making the health service delivery system more responsive to meet people's needs with equitable access. This required the development and functioning of proper management structure, which was called Rogi Kalyan Samitis (RKS). RKS is state's attempt to make “health everyone's business” by de-mystifying health-care delivery at district and sub-district levels especially with reference to facility based health- care delivery systems and encouraging citizen's participation in the management bodies.(2,3)
RKS is now constituted as a registered society under the Societies Registration Act of government of each state, which lays down detail guidelines for registering the Samiti.(4) In Maharashtra, RKS comprises of two bodies-governing body (GB), which is responsible for policy formulation and decision making while executive body (EB) for implementing these decisions. There exists a charter/guideline of RKS which includes a set of well-defined roles and responsibilities of each committee in order to make RKS fully operational in the state.(5) The District Program Managing unit (DPMU) functions as a support system under the NRHM to assist GB and EB on functioning of RKS in the district.(6)
We aimed to analyze operational aspects and challenges of RKS under health systems strengthening.
Materials and Methods
Study design
Mixed method, multi-site, collective case study.
The cases
Three RKS, i.e., one RKS at district level and two at block levels.
Study locale
The district of Pune was selected for study after interactions with District Program Manager (DPM) revealed that, RKS were set up in all the health service delivery facilities.
Study subjects
DPM, Block Program Manager (BPM)/Taluka Health Officer (THO), RKS Members belonging to EB at District Hospital and selected Community Health Center/Rural Hospital (CHC/RH) at block levels, beneficiaries of the out-patient department (OPD) and in-patient department (IPD).
Sampling frame-work
All the study subjects were selected for in depth interviews.
The number of members of EB to be interviewed in depth was restricted to 03 from each facility under study as it was observed that, the level of data saturation was achieved after this.
Two CHCs/RH were selected as either high performing or low performing according to their reported performance at DPMU. High performing CHC/RH means adhering to RKS Charter and closely following the well-defined set of roles and responsibilities, whereas low performing CHC/RH lacked in these areas. The names of these CHCs/RH are anonymized, and they would be mentioned as high performing and low performing CHC/RH.
A total of 10% of patients from OPD, and 20% of patients from IPD were selected randomly at each CHC/RH. The inclusion criteria for respondents were patients 18 years and above.
Informed consent was taken from every official selected for the study beforehand; with the agreement of maintaining his confidentiality.
This study was conducted over a period of 7 months (from August 2011 to February 2012).
Data collection methods
Primary data were collected through semi-structured interviews, researcher's observations, field notes, and quantitative data.
Secondary data were collected from the documented records and reports available at the facilities under study.
Data analysis
Qualitative data were analyzed thematically. The interviews were read word by word; data were extracted and then coded inductively by the authors.
Data were triangulated by combining responses from interviews with the researcher's observations and obtained documentary data.
Results and Findings
Even after repeated visits, researchers were denied facilitation of interaction with authorities/stakeholders at District Hospital. Medical Superintendent (Clinical) who is also the secretary of GB of RKS at DH prohibited the researchers to interact with members of EB though he failed to justify his act. Researchers were sent to the clerk from where they managed to obtain information related to previous years expenditure conducted under RKS grant. Hence, researchers were unable to obtain complete data related to functioning of RKS at this health facility.
Organization of RKS
Organization and activities conducted under RKS is determined on the basis of data taken from the respective health facility. Criteria used are whether the health facility under study abides by guidelines provided by Government.(7)
Table 1 represents the performance of health facilities. Events such as the formation of GB and EB, their composition, frequency of meetings, outreach activities, biomedical waste management, etc., has been taken into organizational consideration in high performing CHC/RH. However, there is no provision of all the above services that aim to achieve patient welfare at low performing CHC/RH and district hospital. RKS was yet to develop and display charter of citizen's health rights at low performing CHC/RH and DH.
Table 1.
Details of organization and activities conducted under RKS at health facilities under study
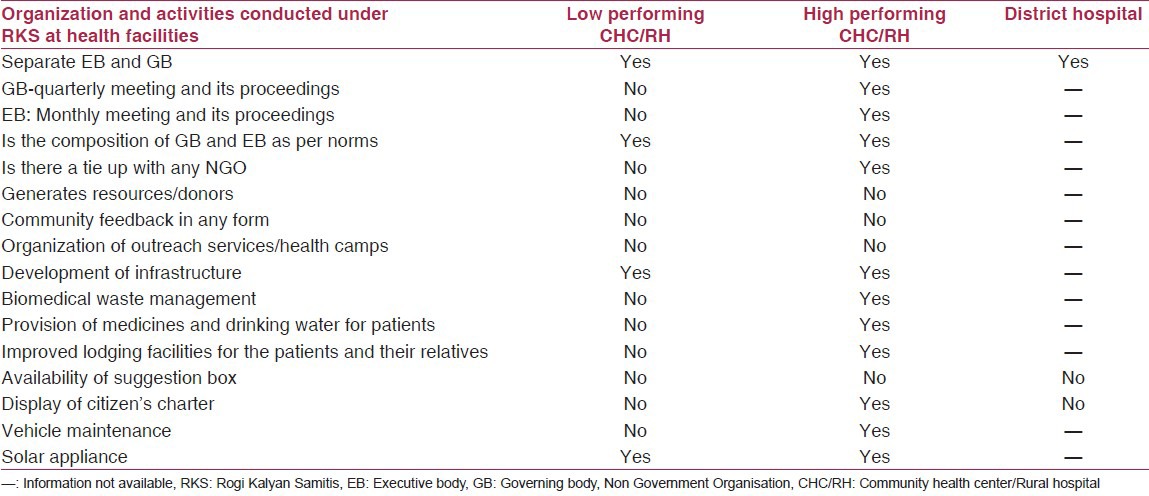
Compliance with citizen's charter is to be ensured through setting up of grievance redressal mechanism, which seems to be the missing link in operationalization of RKS.
RKS guidelines
Guidelines are available with DPMU and at high performing CHC/RH, which are not the case for low performing CHC/RH and DH. From conversation, it was clear that the Medical Superintendent at low performing CHC/RH was unaware of the guidelines. Also, secretary of GB at DH denied working of RKS as per guidelines, though he refused to reveal reasons for the same. Medical Superintendent at DH mentioned “why should we follow the guidelines right from the district hospital to the Primary Health Centers (PHC), when nobody follows RKS guidelines?”
At high performing CHC/RH, the Medical Superintendent mentioned that guidelines were briefed by him to the committee members. However, no photo-copies of any reading material/guidelines related to RKS were provided to members at any of these health facilities.
Functioning of RKS
Meetings
In high performing CHC/RH frequency of meetings was regular and according to guidelines i.e., the frequency of meetings of GB was once in 3 months whereas, meetings of EB were conducted on a monthly basis.
In low performing CHC/RH and DH, it was difficult for the stakeholders to elaborate on documentation details pertaining to the attendance of members attending the meeting and their outcome decision. The THO of low performing CHC/RH admitted that the meetings were not conducted on a regular basis. At high performing CHC/RH, attendance of members attending the meeting was recorded in an updated meeting register and signature of RKS members were obtained across their respective names.
Meeting agenda for the financial year 2010-11
Finding at low performing CHC/RH was that Medical Superintendent decides agenda in advance, and the committee was held only for formal approval of pre-decided issues whereas in high performing CHC/RH the agenda to be executed was unanimously decided by the RKS members in the meetings. As quoted by the Medical Superintendent at low performing CHC/RH “all the powers to carry out expenditure from RKS fund should be given to the Medical Superintendent. What is the need to conduct meetings and increase the load of unnecessary documentation?”
Interactions with members of RKS revealed that; meetings and agenda were organized in democratic style in high performing CHC/RH whereas; the same were conducted in autocratic style at low performing CHC/RH.
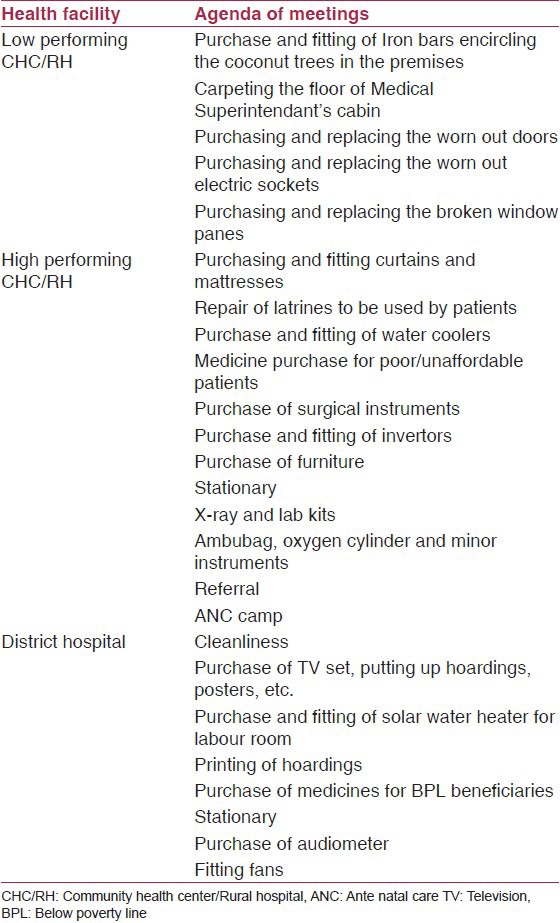
Table 2 infers that, the committees are more concerned with purchasing basic material requirements, repairing and beautification at low performing CHC/RH. High performing CHC/RH reveals setting up of an agenda, which addresses community health needs by the provision of medicine, drinking water facilities, and organization of outreach services. Though the documented agenda set of the DH reflects expenses to be made towards patient welfare, i.e., IEC material and appliances; it is not clear whether the expenditure was carried out under the decided heads as the researchers could not observe any development made in this health facility.
Table 2.
List of the agenda of meetings held in the financial year 2010-11
Capacity building and training
None of the stakeholders could elaborate on the importance of capacity building.
Formal training for health systems and support systems functionaries is yet to be strategized. The DPM said “training sessions are organized periodically from the state level, which includes a component on RKS.” However, the DPM could not furnish any such documented records related to previously organized training sessions.
Similarly, on being interviewed THOs, Medical Superintendent and members of both the blocks declined that any training sessions have been conducted. All of them felt the need of training sessions to be organized as they felt that these sessions would help them to perform effectively. As quoted by the Taluka Health Officer/Block Program Manager of low performing block, “we do not get satisfactory answers for our difficulties from our superiors, for executing the RKS scheme in our block. Hence, periodic training sessions will certainly empower us!”
Finance management
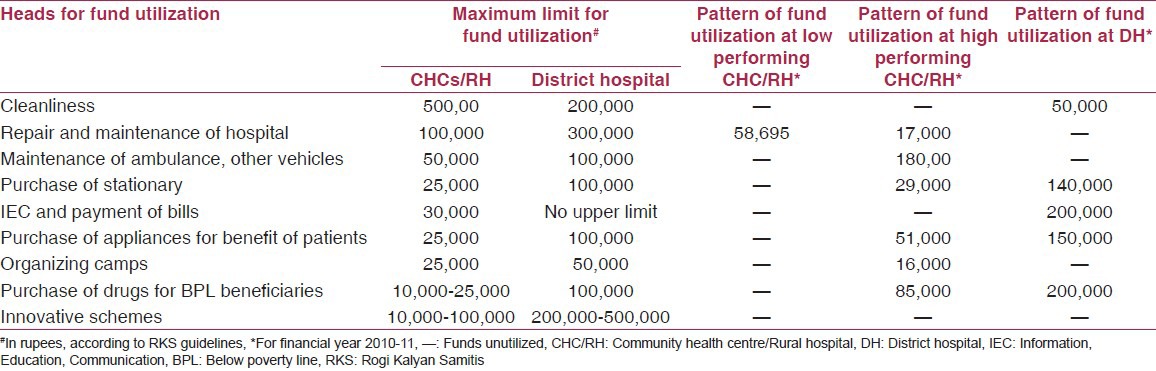
Table 3 depicts that, regardless of consistency in fund allocation, high performing CHC/RH, low performing CHC/RH, and DH have failed to utilize funds according to the RKS guidelines for budget expenditure.(8) In low performing CHC, fund has been under-utilized under one head of repair and maintenance (Rs. 58,695); whereas, the maximum limit is Rs. 100,000. Rest of the funds is left unutilized. In high performing CHC/RH and DH, funds are left unutilized in areas like organization of outreach services and innovative schemes for welfare of the community. Fund utilization has exceeded under heads such as purchase of stationary (Rs. 140,000), purchase of appliances (Rs. 150,000), and drugs for below the poverty line beneficiaries (Rs. 200,000) whereas, the maximum limit is up to Rs. 100,000 only for each head under discussion.
Table 3.
Fund utilization pattern at health facilities
Monitoring system
As quoted by DPM, “appropriate monitoring system is yet to be operationalized in the District. Though the periodic progress is monitored by the GB at some health facilities in the District; much of it needs to be documented.”
A fully operational monitoring system is essential to initiate mid-course correctiveness for improvement and monitoring progress of RKS.
Strengths and concerns about RKS as perceived by key stakeholders
The major strengths of RKS as commonly perceived by stakeholders were community participation and availability of funds at the level of devolution. Whereas, the concerns were lack of capacity building strategies, involvement of people from a political background leading to lack of consensuses among members and excess documentation.
Community perceptions
Out of total 28 respondents (8 IPD and 20 OPD) none were aware about the existence of the RKS in low performing CHC/RH. Yet except for two respondents none complained about the quality of services being provided through this health-care facility.
One patient said “we are poor people, yet we are receiving these services. We have to be satisfied as we do not have any better option due to our inability to bear the costs of health- care services.”
42 out of 50 (20 OPD and 30 IPD) i.e., 84% respondents were aware of the existence of RKS in high performing CHC.
Nearly 72% agreed upon availability of drinking water and clean toilet facility.
Nearly 76% knew about availability of free referral services.
The patients availing indoor services reported satisfactory diet facility and also agreed that medicines were always made available to them.
A total of 94% respondents seemed to be extremely satisfied with the facilities provided.
Discussion
In the context of decentralized decision-making, RKS is a strategy to improve the quality of management responses and thereby facilitate strengthening of health systems as well as health outcomes. This was reflected through developments made in infrastructure and improvements experienced by beneficiaries who approved provision of quality health-care through high performing CHC/RH.
Study revealed that, inadequate support systems for capacity building and training are constraints, which weaken the public-health system.(9,10,11) Failure to build managerial capacities will result in inadequacies in building of technical expertise at level of devolution where the money has been decentralized. Financial management capacity of health facilities, related to management of flexible funds needs to be strengthened; as utilization of funds is not being undertaken as per mandates indicated in guidelines.(9,12) This reflects managerial failure of the support systems resulting in operational challenges of RKS model at district level.
Regular meetings are yet to be conducted in accordance with guidelines resulting in decisions to be taken autocratically at the level of devolution; thus, deviating from the purpose of establishing such Samitis.
Though the GB of each RKS is mandated to act as a monitoring body also; a fully operating monitoring system is yet to be functional. An appropriate monitoring system engaging support systems and health systems functioning can contribute to functionality by providing supportive supervision and better updating of mandatory registers observe mid-course corrective measures at all levels of health facilities delaying, which the mandates of the RKS will remain a distant reality.(9,13)
Compliance of Citizen's charter is ensured through grievance redressal mechanism, as per the guidelines. However, this mechanism is yet to be fully functional; which reveals structural and functional defect in managerial mechanisms, which gives a picture that these health facilities are still functioning in isolation of the need of local communities.(3,9,11,14)
Health system strengthening requires a holistic view and approach in its management. Figure 1 represents that RKS strategy is based on the following building blocks, which contribute to strengthen health systems:
Figure 1.
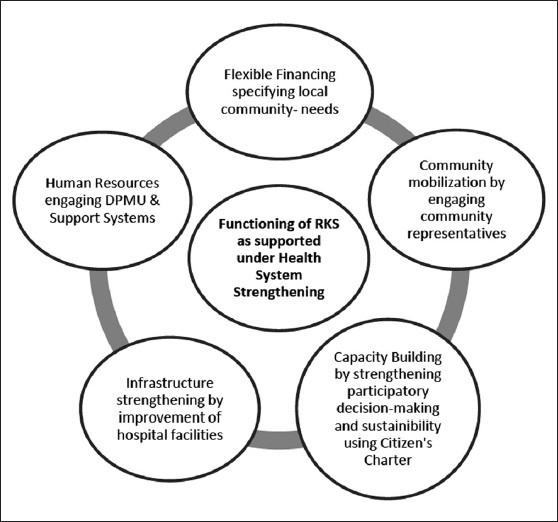
Thematic representation of Rogi Kalyan Samitis through functional health systems
Support systems capacity needs to be coordinated with functional health system by adequate supervision, monitoring and motivation of RKS members.
Financial management and adequate accountability of reporting and documentation.
Effective community participation through social mobilization and partnerships.
Capacity building for systems strengthening.
Conclusion
A review of RKS functioning has revealed that this can become a viable and operationally feasible model by building capacities of RKS members and support systems for effectiveness in RKS functioning, contributing to reporting and documentation of challenges and scopes, bringing out transparency, accountability and partnerships can contribute to transform a community led sustainable RKS instead of bureaucratic led non-participatory approach. This will ensure community led partnerships for scaling up of local specific innovations and sustainable RKS strategies on benefiting health services meaningfully to the local community.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.National Rural Health Mission, Department of Health and Family Welfare, Government of Orissa; 2008. [Last accessed on 2012 Dec 23]. Operational Guideline for Utilisation of Untied Fund, Annual Maintenance Grant and RKS Grant. Available from: http://www.angul.nic.in/UFAMG-RKS.pdf . [Google Scholar]
- 2.Madhya Pradesh: Department of Public Health and Family Welfare; 2010. [Last accessed on 2012 Dec 23]. Rogi Kalyan Samiti Charter. Available from: http://www.mp.gov.in/health/rks/rks-english.pdf . [Google Scholar]
- 3.New Delhi: Ministry of Health and Family Welfare, Government of India, Nirman Bhavan; [Last accessed on 2012 Dec 21]. National Rural Health Mission: Framework for Implementation (2005-2012) Available from: jknrhm.com/Guideline/Frame-Work.pdf. [Google Scholar]
- 4.National Rural Health Mission, Health and Family Welfare Department. Government of India; 2010. [Last accessed on 2012 Dec 21]. Performance Audit. Available from: http://www.agpunjab.gov.in/reports/2010/civil_chap2.pdf . [Google Scholar]
- 5.Rogi Kalyan Samiti. Health Sector Decentralization in Madhya Pradesh. 2004. [Last accessed on 2012 Dec 21]. Available from: http://www.sitesources.worldbank.org/INTINDIA/Resources/rks.pdf .
- 6.National Rural Health Mission, Ministry of Health and Family Welfare, Government of India; 2005. [Last accessed on 2012 Dec 21]. Institutional setup at State and District Level. Available from: http://www.mohfw.nic.in/NRHM state and district health mission-institutional setup.htm . [Google Scholar]
- 7.National Rural Health Mission, Ministry of Health and Family Welfare, Government of India; 2005-2012. [Last accessed on 2012 Dec 21]. Guidelines for constitution of Rogi Kalyan Samitis. Available from: http://mohfw.nic.in/nrhm/guidelines . [Google Scholar]
- 8.National Rural Health Mission: Rugna Kalyan Samiti Annual Maintenance Grant, Untied Funds, Village Health Nutrition and Sanitation Committee, Government of Maharashtra; 2005-2012. pp. 51–6. [Google Scholar]
- 9.Ministry of Health and Family Welfare, Government of India; 2010. [Last accessed on 2012 Dec 21]. Fourth Common Review Mission Report-Maharashtra. Available from: http:// www.mohfw.nic.in . [Google Scholar]
- 10.Government of India, New Delhi: National Rural Health Mission, Ministry of Health and Family Welfare, Nirman Bhavan; 2011. [Last accessed on 2012 Dec 21]. Fifth Common Review Mission Main Report. Available from: http://www.mohfw.nic.in/NRHM/CRM/CRM_files/Fifth_CRM.htm . [Google Scholar]
- 11.Rogi Kalyan Samiti an Innovative Project for the Management of Public Hospitals through Community Participation in the state of Madhya Pradesh, India. [Last accessed on 2012 Dec 21]. Available from: http://www.nihfw.org/WBI/docs/India Flagship session/../RKS.pdf .
- 12.New Delhi: National Institute of Health and Family Welfare; 2008-2009. [Last accessed on 2012 Dec 21]. A Rapid Appraisal of Functioning of Rogi Kalyan Samiti in the Districts of Nainital and Uddham Singh Nagar, Uttarakhand. Available from: http://www.nihfw.org/pdf/RAHIII%20Reports/Uttarakhand.pdf . [Google Scholar]
- 13.National Rural Health Mission (2005-2012) Mission Document. 2005-2012. [Last accessed on 2012 Dec 21]. Available from: http://www.mohfw.nic.in/NRHM/Documents/Mission_Documents.pdf .
- 14.Community Participation. National Rural Health Mission, Government of India. 2009-2010. [Last accessed on 2012 Dec 21]. Available from: http://www.cag.gov.in/html/reports/civil/2009_8_PA/chap_3.pdf .