

Abstract
Background
Whether to return individual research results from cancer genetics studies is widely debated, but little is known about how participants respond to results disclosure or about its time and cost burdens on investigators.
Methods
We recontacted participants at one site of a multicenter genetic epidemiologic study regarding their CDKN2A gene test results and implications for melanoma risk. Interested participants were disclosed their results by telephone and followed for 3 months.
Results
Among 39 patients approached, 27 were successfully contacted, and 19 (70% uptake) sought results, including three with mutations. Prior to disclosure, participants endorsed numerous benefits of receiving results (mean = 7.7 of 9 posed), including gaining information relevant to their children’s disease risk. Mean psychological well-being scores did not change from baseline, and no decreases to melanoma prevention behaviors were noted. Fifty-nine percent of participants reported that disclosure made participation in future research more likely. Preparation for disclosure required 40 minutes and $611 per recontact attempt. An additional 78 minutes and $68 was needed to disclose results.
Conclusion
Cancer epidemiology research participants who received their individual genetic research results showed no evidence of psychological harm or false reassurance from disclosure and expressed strong trust in the accuracy of results. Burdens to our investigators were high, but protocols may differ in their demands and disclosure may increase participants’ willingness to enroll in future studies.
Impact
Providing individual study results to cancer genetics research participants poses potential challenges for investigators, but many participants desire and respond positively to this information.
Introduction
The debate about investigators’ responsibilities to communicate individual genetic results obtained from cancer genomics research to study participants is hindered by a lack of data. Although participants’ interest in receiving research results is well established (1, 2), the motivation behind such interest is not adequately characterized. Furthermore, the psychological and behavioral impact of receiving individual research results is unclear, and data about time and monetary demands on investigators are lacking. Calls have therefore been made to collect these data as part of ongoing clinical research (3). Research on the relationship between cyclin-dependent kinase inhibitor type 2A (CDKN2A) and melanoma susceptibility provides an instructive context to explore this issue. Numerous studies have shown an association between CDKN2A mutations and increased risk for melanoma (4). However,CDKN2A genetic testing is currently not standard clinical care, even in high-risk groups, due to concerns including wide variability in penetrance estimates, potential for negative test results to cause false reassurance, and uncertainty about the association of CDKN2A mutations with other types of cancer (5). Until these concerns are addressed, the International Melanoma Genetics Consortium has recommended that CDKN2A testing for melanoma susceptibility testing be restricted to research contexts with well-developed pretest education and genetic counseling protocols (5). Such research has shown individuals to be interested in testing (6, 7), with no evidence that susceptibility information leads to psychological distress (7, 8), and some evidence that testing can result in better compliance with screening recommendations (8, 9).
Here, we report data from a protocol that disclosed CDKN2A gene test results derived from research to individual participants of an epidemiologic study on genetic risk factors for melanoma. Specifically, we report on predisclosure attitudes toward melanoma genetic risk information and disclosure of research results, psychological and behavioral responses to disclosed information, satisfaction with the disclosure process, and time and monetary demands on investigators.
Materials and Methods
Overview and participants
A study flowchart is presented in Figure 1. Participants were sampled in 2008 from University of Michigan (U-M) participants in the Genetics, Environment and Melanoma (GEM) Study, a hospital-based study of genetic susceptibility to melanoma. Methodology and findings from the GEM Study are published elsewhere (10, 11). In short, all GEM participants at the U-M site were adults who had a first invasive primary or second and higher-order invasive or in situ melanoma identified in 2000. Because the burden and safety of disclosing individual genetic test results to research participants was relatively unknown, a limited number of GEM Study participants were sampled in this pilot study. Seven CDKN2A mutation carriers-– representing all carriers from the U-M study site-–and 32 noncarriers matched to carriers by sex, age ± 4 years, and original melanoma diagnosis (single vs. multiple primary) were targeted for recruitment. Sampled participants were younger than nonsampled GEM Study participants on average (Δ = 9.8 years, P < 0.001) but were representative on all other factors, including gender and race.
Figure 1.
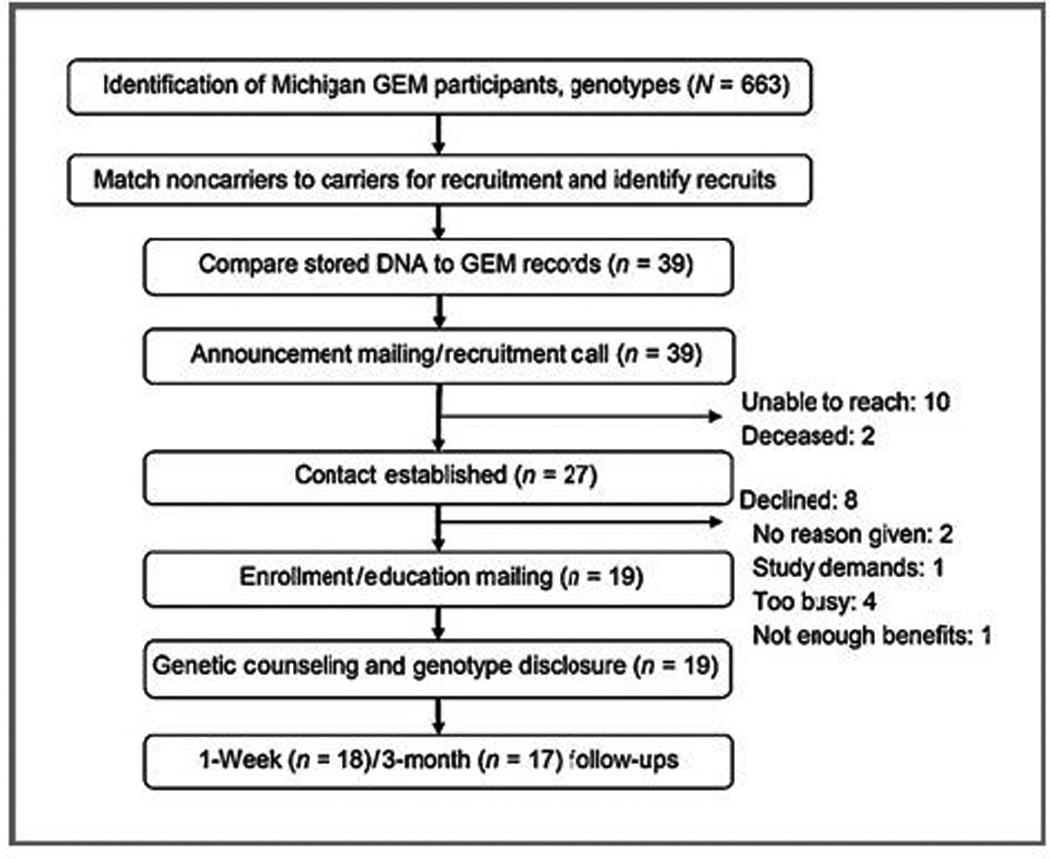
Study flowchart.
Archived DNA samples were first retested to confirm CDKN2A mutation status and contact information was updated from current medical records, if available (archived samples were missing for 3 recruits). Recruits were sent an advance mailing from the U-M GEM Study site principal investigator (S.B.G.) informing them about the study. A research assistant then called to enroll interested participants and obtain informed consent. Consent materials emphasized that GEM Study testing was not carried out in clinical laboratories, but that results may be of significance to the person’s health. On enrollment, participants were sent a baseline questionnaire and educational materials about risk factors for melanoma, including CDKN2A mutations. Educational materials were developed on the basis of the available genetic epidemiologic literature and cited a 5% risk for another melanoma among melanoma survivors and a risk of 30% to 65% risk through age 80 for melanoma among CDKN2A mutation carriers. Participants reviewed these materials with a genetic counselor via telephone (participants were given a choice of in-person or telephone consultations, and all opted for telephone). At the end of the genetic counseling session, participants were given the option of receiving their individual CDKN2A genotype information and its implications for melanoma risk. Participants who opted for disclosure received a written summary of points discussed during disclosure and recommendations for physician follow-up, if warranted by participant request or a family history suggestive of other cancer syndromes.
The impact of disclosure was assessed via a self-administered follow-up questionnaire mailed 3 months after receipt of genotype. Given that an emotional impact of genetic susceptibility information is often only seen shortly after disclosure (12–15), mood and distress was also assessed 1 week after disclosure. A detailed description of how this study protocol was developed and ethical issues addressed appears in a previous publication (16).
Measures
Demographic characteristics, family history, and test uptake
Participant demographics were obtained by self-report. Family history of melanoma was reported to the genetic counselor by participants at the beginning of the telephone genetic counseling session. Test uptake was measured by the proportion of participants who sought results among those who had been successfully reached by the study team.
Attitudes about melanoma genetic risk information and disclosure of research results
Perceived benefits, and risks and limitations of melanoma genetic risk information were assessed in the baseline questionnaire by modified scales implemented in studies of BRCA1/2 testing (17) and adapted for research on CDKN2A (8). Opinions about the obligations of investigators to recontact research participants were assessed by a single item adapted from another study (18).
Psychological responses
Participants’ melanoma risk perceptions were assessed with the open-ended item, "out of 100 people like you, how many of them do you think will develop another melanoma?" Pre- and postdisclosure psychological well-being were compared by the 5-item version of the Mental Health Index (MHI-5; ref. 19), a validated instrument with scores ranging from 0 to 100 with higher scores indicating greater well-being and scores less than 65 suggesting a possible mood disorder. Event-specific distress was assessed by the 7-item intrusion subscale of the Impact of Events Scale (IES; ref. 20), a commonly used scale in genetics research which ranges from 0 to 35 with higher scores indicating greater distress. Concern about results was measured with a single item asking participants to rate their concern about their genetic test result on a 7-point scale (1 = not at all to 7 = extremely concerned).
Behavioral responses
Sharing of information was assessed at follow-up by asking participants whether they had told others their melanoma risk estimate or CDKN2A genetic test results. Participants who indicated that they had done so were asked to specify with whom information was shared. Baseline health behaviors were assessed by asking participants to rate the frequency of 4 protective behaviors practiced when "outside on a sunny summer day for more than one hour." Response options included never, seldom, sometimes, nearly always, and always. Baseline health behaviors were also assessed by asking participants to report how many times they had conducted a skin self-examination in the previous 2 months. Health behavior changes following results disclosure were assessed by asking participants to indicate whether they had increased, decreased, or did not change the frequency with which they performed 8 preventive behaviors examined in other studies of melanoma prevention (21), including wearing a wide-brimmed hat when in the sun, using sunscreen of SPF 15 or more when in the sun, and performing skin self-examinations.
Satisfaction and trust
Overall satisfaction with the disclosure process was assessed by examining the mean of 4 items asking participants to rate their satisfaction (1= not at all to 7 = extremely satisfied) with the following: information, explanations, reassurance, and help in decision making. Participants also rated how disclosure affected their willingness to take part in genetic research in the future. In addition, participants reported how (e.g., telephone vs. in-person) and when they would have preferred to receive their test results. Finally, participants were asked their perceptions about the accuracy of the genetic test result and their trust in the research team to give accurate information.
Demands on investigators
Time spent on protocol preparation (review of GEM Study and medical records and confirmation of genotypes) and creation of genetic counseling materials was estimated by the study personnel responsible for completing each step. Time spent on recontacting participants and disclosure components (education, genetic counseling, results disclosure, and follow-up) was tracked throughout the study. The cost of genotype confirmation varied by mutation status: $350 to confirm the presence of a mutation and $700 to confirm the absence of a mutation. The expense of designing and printing the educational brochure was calculated by amortizing the $3,050 total cost across 330 projected disclosures from the 663 total eligible Michigan GEM Study participants. Personnel costs were calculated on the basis of annual salaries of $63,000 for a genetic counselor (22) and $30,000 for a research assistant (23), plus 30% benefits. All other costs were determined through a poststudy audit.
Results
Sample demographics, family history, and test uptake
Participant demographic characteristics are summarized in Table 1. Of the 39 GEM Study participants targeted for enrollment, 12 (31%) could not be reached: 2 had died since their GEM Study participation (confirmed with a review of the National Death Index) and contact information on another 10 was outdated and the patients could not be traced. Of the remaining 27 recruits, 19 (70%) agreed to participate, including 3 CDKN2A mutation carriers. Four of those declining participation cited being too busy, one was uncomfortable with study demands, and one stated that the benefits were not worth the effort. Two others declined without providing reasons.
Table 1.
Demographics of participants who opted for disclosure (N = 19)
| n (%) | |
|---|---|
| Sex | |
| Male | 9 (47) |
| Female | 10 (53) |
| Age | |
| 30–39 | 2 (11) |
| 40–49 | 3 (16) |
| 50–59 | 9(47) |
| 60–69 | 5 (26) |
| Married | 16 (84) |
| Has children | 16 (84) |
| White, non-Hispanic | 19 (100) |
| College degree or higher | 15 (79) |
| Employment status | |
| Part-time or full-time | 11 (58) |
| Retired | 7 (37) |
| Household income | |
| <$70,000 | 3 (16) |
| $70,000–$99,999 | 8 (42) |
| ≥$100,000 | 8 (42) |
| Has insurance | |
| Health insurance | 18 (94) |
| Life insurance | 16 (84) |
| Disability insurance | 7 (37) |
Each mutation carrier and 4 of 16 (25%) of the noncarriers reported a family history of melanoma. All enrolled participants ultimately agreed to melanoma risk and CDKN2A genotype disclosure. Eighteen disclosures occurred between November 2008 and March 2009, with the final one occurring in June 2009.
Attitudes about melanoma genetic risk information and disclosure of research results
Predisclosure attitudes toward genetic information were favorable. On average, participants endorsed (i.e., rated being at least "a little" important) 7.7 of 9 (SD = 1.7) reasons for and 3.5 of 9 (SD = 1.8) reasons against seeking test results. Four reasons for seeking test results were rated as "very" or "extremely" important by more than half of the participants, with "to give information about possible risks to my children" most strongly endorsed. In fact, all 16 participants with children rated that item at least "somewhat" important. Only 3 of 9 reasons for not receiving results were rated as very or extremely important by any participants (Table 2).
Table 2.
Benefits, risks and limitations of test results rated "very" or "extremely" important prior to disclosure
| n (%) | |
|---|---|
| Benefits | |
| To give information about possible risks to my children's health | 14 (74) |
| To help researches learn more about melanoma | 13 (68) |
| To inform how I might purse perventive measures | 11(58) |
| Curiosity | 9 (47) |
| To put my mind at ease if I found out I was not at increased risk for another melanoma or a recurrence of melanoma | 7 (37) |
| To know if I should prepare my family for my possible illness | 5 (26) |
| To inform how and when I take care of my personal affairs | 3 (16) |
| To inform arrangements for medical care later in life | 1 (5) |
| Risks and limitations | |
| It could make me worry about my children's risk of getting melanoma | 2 (11) |
| This testing does not give me a definite "Yes or no" answer about my risk for another melanoma | 2 (11) |
| The results could affect my health insurance | 1 (5) |
| The results might upset my loved ones | 0 (0) |
| It would be too upsetting to find out I'm at increased risk for another melanoma | 0 (0) |
| The results could change how people look at act toward me | 0 (0) |
| The results could affect my employment | 0 (0) |
| My family does not think it is a good idea | 0 (0) |
| The procedure would be too burdensome | 0 (0) |
NOTE: Response options includes ”not at all," "a little," "somewhat, " "very, " and "extremely. "
Beliefs about investigators’ obligations to recontact research participants are presented in Table 3. Fifteen participants (79%) reported that researchers had some obligation to recontact research participants, and 3 others (17%) felt that recontact could be established under certain conditions, but only through a healthcare professional.
Table 3.
Predisclosure attitudes of perticipants about the obligations of researchers to recontact research participants
| n (%) | |
|---|---|
| Yes. Regularly, even if no new discoveries are made | 3 (16) |
| Yes, when any new discoveries are made | 6 (32) |
| Yes, but only when new discoveries are made that pertain directly to the recontacted patient | 6 (32) |
| No, but ask my primary care physician/internist/dermatologist to recontact me | 2 (11) |
| No, I will contact the genetics provider if I want more information | 1 (5) |
| No, research participants should never be recontacted with new information | 0 (0) |
| Researchers have no obligations | 1 (5) |
Psychological responses to disclosure
Mean risk perceptions for the 3 mutation carriers were high at both baseline and 3 months: 56.7% (SD = 11.5%) and 60.0% (SD = 21.8%), respectively. Mean risk perceptions for noncarriers were lower and had wide distributions: 21.7% (SD = 21.5%) at baseline and 18.6% (SD = 20.0%) at 3 months. At both time points, mutation carriers perceived their risks for another melanoma to be higher than noncarriers (baseline: t = 2.70, P = 0.02; follow-up: t = 3.21, P < 0.01). Paired t tests showed no significant pre- and postdisclosure changes to risk perceptions for either mutation carriers (t =0.19, P =0.87) or noncarriers (t = 0.90, P = 0.38).
Data suggested no significant psychological harm from disclosure. MHI-5 scores, presented in Figure 2, averaged 83 at baseline and at both follow-ups (scores <65 indicate a possible mood disorder), excluding one participant who was given a clinical diagnosis of metastatic melanoma just after his results disclosure (MHI-5 scores: 88 at baseline, 36 at 1 week, and 20 at 3 months). Event-specific distress was low, with IES scores averaging 2.2 at 1 week and 1.0 at 3 months. However, mutation carriers reported greater subjective concern about test results than noncarriers (x = 4.7 vs. 1.7, t = 5.4, P < 0.01).
Figure 2.
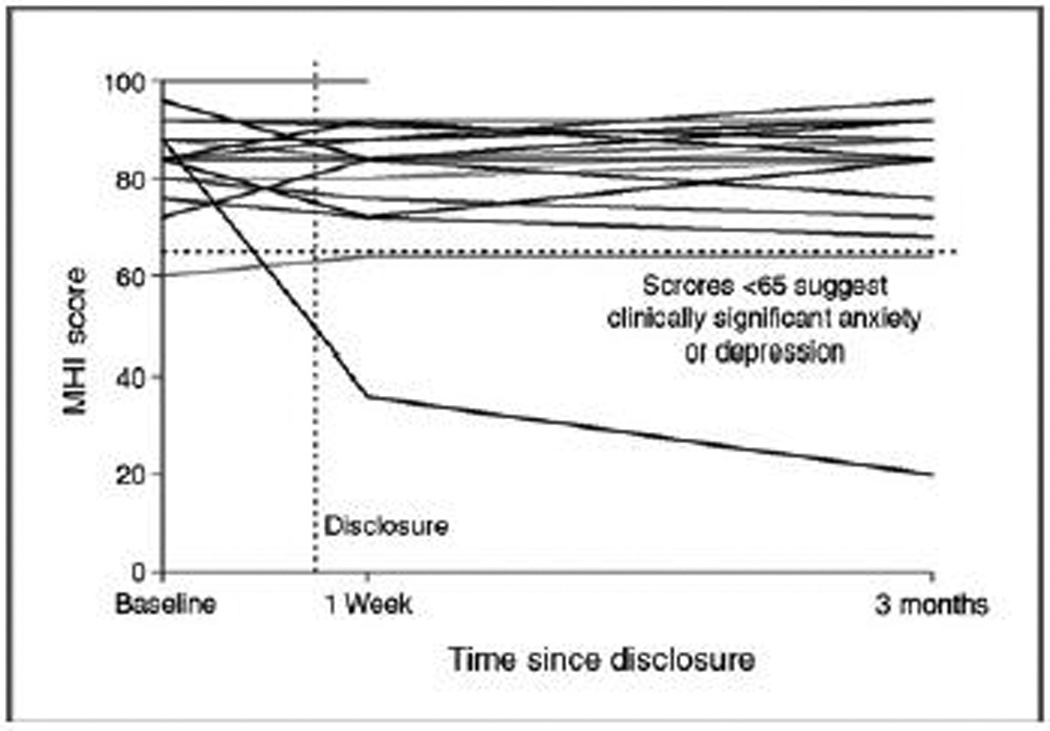
MHI-5 scores of individual participants before and after disclosure. Higher scores indicate better mental well-being.
Behavioral responses to disclosure
All but one participant (94%) shared information from the risk disclosure session with others by the 3-month follow-up. Among those who shared information, results were shared most often with a spouse or other family member (94%). A substantial proportion also shared results with friends (38%) or a health professional (31%).
Most participants reported melanoma prevention behaviors prior to disclosure. The number of participants reporting at baseline that they "always" or "nearly always" practiced the queried melanoma prevention behaviors on sunny summer days was 4 (21%) for wearing long-sleeved shirts, 10 (53%) for staying in the shade, 12 (63%) for wearing wide-brimmed hats, and 15 (79%) for using sunscreen. Twelve participants (63%) reported having conducted a skin self-examination within the previous 2 months. Few health behavior changes were reported at the 3-month follow-up. No participants reported changes to sun exposure between 10 AM and 4 PM, wearing long sleeve shirts or long pants when in the sun, or visits to tanning salon. One participant (6%) reported using a wide-brimmed hat more often when in the sun, 1 (6%) reported increasing the frequency of physician skin examinations, 2 (12%) reported increased sunscreen use, and 4 (24%) reported performing skin self examinations more frequently. No decreases to preventive behaviors were reported.
Satisfaction and trust
Satisfaction with disclosure was high. Participants rated the protocol an average of 6.1 on a 7-point scale at the 3-month follow-up, and the majority of participants (59%) asserted that their participation made it more likely that they would participate in research in the future. Eleven participants (65%) stated that telephone was their preferred method of disclosure, and another 2 (12%) claimed no preferred method but stated that telephone was acceptable. Three participants (18%) would have preferred receiving results via a letter, and 1 (6%) would have preferred a visit to the clinic. Four (24%) would have preferred receiving results after the study had been reviewed by other researchers, 6 (35%) wanted them as soon as individual genotypes were determined, 1 (6%) wanted results as soon as results had been published, 5 (29%) wanted results as soon as the study was finished and analyzed, and 1 (6%) was "fine with the way things were handled."
Despite being informed that testing had been conducted in a laboratory that was not CLIA-certified, participants believed the results to be accurate at the 3-month follow-up. Average level of trust in the results was 6.1 on a 7-point scale, and average level of trust in researchers to give accurate information was 6.2 on a 7-point scale. However, one mutation carrier stated that he would be seeking future confirmatory testing.
Demands on investigators
Time demands averaged 161 minutes per completed disclosure. An average of 40 minutes was spent on each of the 39 GEM Study participants we attempted to recontact, plus an additional 78 minutes for each of the 19 participants who agreed to receive results. The financial costs associated with our protocol averaged $1,322 per completed disclosure. An average of $611 was spent on each of the 39 GEM Study participants we tried to recontact, plus an additional $68 for each of the 19 participants who agreed to receive results (Table 4).
Table 4.
Costs of preparation and disclosure
| Preparation Component | Cost/attempt ($) | SD ($) | Disclosure component | Cost/participant ($) | SD ($) |
|---|---|---|---|---|---|
| Personnela (RA, 40 min/attempt) | 13.05 | 5.03 | Personnela (GC, 78 min/participant) | 53.49 | 7.73 |
| Genotype confirmationb | 592.31 | 214.76 | Education mallingc | 13.21 | 2.88 |
| Recontact malling | 5.49 | 2.18 | Follow-up malling | 1.05 | 0.00 |
| Total per attempted recontact | 610.85 | 214.39 | Total per participant | 67.75 | 7.99 |
Based on annual salaries of $30,000 for a research assistant (RA) and $63,000 for a genetic counselor (GC), +30% benefits.
$350 to confirm the presence of a mutation,$700 to confirm the absence of a mutation. Archived DNA was missing for 3 GEM study subjects we attempted to recontact.
Includes $3,050 amortized across 330 projected disclosures from 663 total michigan GEM study subjects for design and printing of an educational brochure.
Discussion
This study is among the first to provide data about the impact of disclosing individual genetic results from cancer research. Despite the small number of GEM Study participants in the study, several themes are evident. First, most participants we were able to reach wanted to learn their individual genetic test results. More than two thirds of such participants chose to learn more about CDKN2A,and all of them ultimately opted to receive their individual genetic test results. Despite being told that results would not change clinical recommendations for skin examinations, participants perceived both clinical utility (e.g., informing prevention measures) and personal utility (e.g., psychological relief) in the information. Moreover, parents seemed to appreciate learning about the potential implications of the information for their children due to shared genes. All participants with children rated the benefit, "to give information about possible risks to my children’s health" as at least somewhat important, and nearly all participants shared information with another family member. Similar to other studies of recontact and disclosure (18), participants perceived benefits not only for themselves but also for their families by making them aware of possible risks to their health.
Participants also did not seem to exhibit adverse psychological or behavioral effects following results disclosure. No short-term psychological harm was evident, echoing findings from other studies of CDKN2A genetic testing (7, 8) and of genetic susceptibility testing in general (13, 14, 24). Postdisclosure satisfaction ratings were high, and most participants stated that they felt more willing to participate in genetic research in the future as a result of disclosure. In addition, the information did not seem to decrease melanoma screening behaviors. The potential for psychological harm (25), and the potential for negative results to lead to "false reassurance," is a concern about disclosure of individual research results in general (25) and of CDKN2A genetic testing specifically (26). Our results do not support such concerns.
At the same time, disclosure seemed to have little impact on motivating participants to adopt more prevention behaviors, even among those identified to be CDKN2A mutation carriers. The lack of evidence for behavior change is somewhat surprising given that more than half of participants endorsed "to inform how I might pursue preventive measures" as a very or extremely important benefit of testing, although participants were explicitly told that their results did not change clinical recommendations for prevention. The lack of changes to health behaviors may be explained by the general lack of changes to melanoma risk perceptions. Preventive health behaviors are often driven by risk perceptions (27), and melanoma risk perceptions did not change for most participants because predisclosure risk perceptions were already close to calculated risk estimates incorporating CDKN2A genotypes for both mutation carriers and noncarriers. Of note, all mutation carriers had a family history of melanoma, whereas the majority of noncarriers did not. Prior to disclosure as part of our study, participants’ melanoma risk perceptions were likely already shaped by family histories of melanoma, which reflected their actual CDKN2A genotypes.
This study is also among the first to provide data about the burdens to investigators of disclosing individual genetic test results derived from research. Overall, our protocol required more than 2 hours 30 minutes and more than $1,300 per completed disclosure to execute. It is important to keep in mind that this protocol represents a thoughtfully prepared, careful approach to testing disclosure and genetic counseling. Given the dearth of empirical data on recontact and disclosure protocols, we were conservative in many choices. The most expensive step-–the confirmation of genotypes-–might be considered optional (28, 29), and time and money could be saved by using publicly available educational materials rather than custom-designing them. Other disclosure strategies, such as web-based communications developed in the context of biobanking (30), could further reduce burdens on investigators. Finally, we recontacted both mutation carriers and noncarriers. Disclosure may arguably be required only in the cases where mutations are identified. Investigators may choose to develop recontact and disclosure protocols given the constraints of their time and budgets.
A number of limitations should be noted. The small sample size limits our ability to make inferences from the data, and the sample we enrolled may not have been representative of the initial study population. The lack of diversity in our study is understandable given that melanoma predominantly affects non-Hispanic whites; however, findings about results disclosure may not generalize to other ethnic groups. Study participants also tended to be more educated, have larger household incomes, and were more likely to be insured than the U. S. population at large, and results were disclosed to a population that had already been diagnosed with melanoma. Findings may not generalize to individuals with lower socioeconomic status or asymptomatic individuals with no personal experience with cancer. Behavioral responses may be subject to seasonal effects, as the vast majority of disclosures occurred in the late fall and winter months with follow-ups occurring in spring months. Finally, institutional capacity at our site permitted us to create a team with expertise in clinical genetics, genetic counseling, bioethics, health psychology, and health behavior. The expertise of our team allowed us to make specific recommendations for additional clinical follow-up, if warranted or requested. Researchers lacking the same access to interdisciplinary expertise may need to seek institutional partners to implement a similar protocol.
Nevertheless, our results underscore the need to consider the issue of disclosure when designing the initial epidemiologic study. Participant preferences about whether, when, and how to disclose individual research results can vary greatly and would be best addressed at the point of enrollment during informed consent. Should results disclosure be warranted, researchers and their institutions will need to budget time and finances, and they will need to consider effective means of maintaining contact with research participants over time.
The proliferation of genome-wide association studies and the increasing reach of full-genome sequencing increase the likelihood of discovering clinically relevant information during epidemiologic research (31), information which may create an obligation to recontact research participants and disclose individual research results. Disclosure poses substantial challenges, but participants want the information for both clinical and nonclinical reasons and for both familial and individual purposes. Moreover, there may be benefits for participants and investigators alike, as our respondents asserted that results disclosure will make them more likely to participate in future studies. If so, disclosing individual research results may not only be ethically warranted, but may also provide long-term gains for institutions through the reenrollment of participants in new cancer studies and enhancement of public trust of and satisfaction with the research enterprise.
Acknowledgments
We thank Jill Cooper, MPH, for her assistance in creating materials and the study database, and Monica Marvin, MS, CGC, for her assistance on protocol development and results disclosure.
Grant Support
This study was funded by awards from the Clinical/Translational Resource Allocation Committee of the University of Michigan Comprehensive Cancer Center (supported by NIH grant P30CA46592) and the University of Michigan. The GEM study was supported by NCICA98018 (S.B. Gruber). The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Footnotes
Disclosure of Potential Conflicts of Interest
No potential conflicts of interest were disclosed.
References
- 1.Shalowitz DI, Miller FG. Communicating the results of clinical research to participants: attitudes, practices, and future directions. PLoS Med. 2008;5:e91. doi: 10.1371/journal.pmed.0050091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Keogh LA, Southey MC, Maskiell J, Young MA, Gaff CL, Kirk J, et al. Uptake of offer to receive genetic information about BRCA1 and BRCA2 mutations in an Australian population-based study. Cancer Epidemiol Biomarkers Prev. 2004;13:2258–2263. [PubMed] [Google Scholar]
- 3.Partridge AH, Winer EP. Sharing study results with trial participants: time for action. J Clin Oncol. 2009;27:838–839. doi: 10.1200/JCO.2008.20.0865. [DOI] [PubMed] [Google Scholar]
- 4.Udayakumar D, Tsao H. Melanoma genetics: an update on riskassociated genes. Hematol Oncol Clin North Am. 2009;23:415–429. doi: 10.1016/j.hoc.2009.03.011. [DOI] [PubMed] [Google Scholar]
- 5.Kefford R, Bishop JAN, Tucker M, Bressac-de Paillerets B, BianchiScarra G, Bergman W, et al. Genetic testing for melanoma. Lancet Oncol. 2002;3:653–654. doi: 10.1016/s1470-2045(02)00894-x. [DOI] [PubMed] [Google Scholar]
- 6.Kasparian NA, Meiser B, Butow PN, Soames Job RF, Mann GJ. Anticipated uptake of genetic testing for familial melanoma in an Australian sample: an exploratory study. Psychooncology. 2007;16:69–78. doi: 10.1002/pon.1052. [DOI] [PubMed] [Google Scholar]
- 7.de Snoo FA, Riedijk SR, van Mil AM, Bergman W, ter Huurne JA, Timman R, et al. Genetic testing in familial melanoma: uptake and implications. Psychooncology. 2008;17:790–796. doi: 10.1002/pon.1377. [DOI] [PubMed] [Google Scholar]
- 8.Kasparian NA, Meiser B, Butow PN, Simpson JM, Mann GJ. Genetic testing for melanoma risk: a prospective cohort study of uptake and outcomes among Australian families. Genet Med. 2009;11:265–278. doi: 10.1097/GIM.0b013e3181993175. [DOI] [PubMed] [Google Scholar]
- 9.Aspinwall LG, Leaf SL, Dola ER, Kohlmann W, Leachman SA. CDKN2A/p16 genetic test reporting improves early detection intentions and practices in high-risk melanoma families. Cancer Epidemiol Biomarkers Prev. 2008;17:1510–1519. doi: 10.1158/1055-9965.EPI-08-0010. [DOI] [PubMed] [Google Scholar]
- 10.Begg CB, Hummer AJ, Mujumdar U, Armstrong BK, Kricker A, Marrett LD, et al. A design for cancer case-control studies using only incident cases: experience with the GEM study of melanoma. Int J Epidemiol. 2006;35:756–764. doi: 10.1093/ije/dyl044. [DOI] [PubMed] [Google Scholar]
- 11.Berwick M, Orlow I, Hummer AJ, Armstrong BK, Kricker A, Marrett LD, et al. The prevalence of CDKN2A germ-line mutations and relative risk for cutaneous malignant melanoma: an international populationbased study. Cancer Epidemiol Biomarkers Prev. 2006;15:1520–1525. doi: 10.1158/1055-9965.EPI-06-0270. [DOI] [PubMed] [Google Scholar]
- 12.Heshka JT, Palleschi C, Howley H, Wilson B, Wells PS. A systematic review of perceived risks, psychological and behavioral impacts of genetic testing. Genet Med. 2008;10:19–32. doi: 10.1097/GIM.0b013e31815f524f. [DOI] [PubMed] [Google Scholar]
- 13.Douma KFL, Aaronson NK, Vasen HFA, Bleiker EMA. Psychosocial issues in genetic testing for familial adenomatous polyposis: a review of the literature. Psychooncology. 2008;17:737–745. doi: 10.1002/pon.1357. [DOI] [PubMed] [Google Scholar]
- 14.Green RC, Roberts JS, Cupples LA, Relkin NR, Whitehouse PJ, Brown T, et al. A randomized trial of APOE genotype disclosure for risk of Alzheimer's disease: the REVEAL Study. N Engl J Med. 2009;361:245–254. doi: 10.1056/NEJMoa0809578. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Rew L, Kaur M, McMillan A, Mackert M, Bonevac D. Systematic review of psychosocial benefits and harms of genetic testing. Issues Ment Health Nurs. 2010;31:631–645. doi: 10.3109/01612840.2010.510618. [DOI] [PubMed] [Google Scholar]
- 16.Roberts JS, Shalowitz DI, Christensen KD, Everett JN, Kim SY, Raskin L, et al. Returning individual research results: development of a cancer genetics education and risk communication protocol. J Empir Res Hum Res Ethics. 2010;5:17–30. doi: 10.1525/jer.2010.5.3.17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lerman C, Narod S, Schulman K, Hughes C, Gomez-Caminero A, Bonney G, et al. BRCA1 testing in families with hereditary breastovarian cancer. A prospective study of patient decision making and outcomes. JAMA. 1996;275:1885–1892. [PubMed] [Google Scholar]
- 18.Griffin CA, Axilbund JE, Codori AM, Deise G, May B, Pendergrass C, et al. Patient preferences regarding recontact by cancer genetics clinicians. Fam Cancer. 2007;6:265–273. doi: 10.1007/s10689-007-9117-0. [DOI] [PubMed] [Google Scholar]
- 19.Rumpf H-J, Meyer C, Hapke U, John U. Screening for mental health: validity of the MHI-5 using DSM-IV Axis I psychiatric disorders as gold standard. Psychiatry Res, 2001;105:243–253. doi: 10.1016/s0165-1781(01)00329-8. [DOI] [PubMed] [Google Scholar]
- 20.Horowitz M, Wilner N, Alvarez W. Impact of Event Scale: a measure of subjective stress. Psychosom Med. 1979;41:209–218. doi: 10.1097/00006842-197905000-00004. [DOI] [PubMed] [Google Scholar]
- 21.Mujumdar UJ, Hay JL, Monroe-Hinds YC, Hummer AJ, Begg CB, Wilcox HB, et al. Sun protection and skin self-examination in melanoma survivors. Psychooncology, 2009;18:1106–1115. doi: 10.1002/pon.1510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Smith M, Freivogel M, Parrott S. Professional Status Survey 2008. Chicago, IL: National Society of Genetic Counselors, Inc; 2009. [Google Scholar]
- 23.Weinstein MC, Siegel JE, Gold MR, Kamlet MS, Russell LB. Recommendations of the panel on cost-effectiveness in health and medicine. JAMA. 1996;276:1253–1258. [PubMed] [Google Scholar]
- 24.Beran TM, Stanton AL, Kwan L, Seldon J, Bower JE, Vodermaier A, et al. The trajectory of psychological impact in BRCA1/2 genetic testing: does time heal? Ann Behav Med. 2008;36:107–116. doi: 10.1007/s12160-008-9060-9. [DOI] [PubMed] [Google Scholar]
- 25.Bookman EB, Langehorne AA, Eckfeldt JH, Glass KC, Jarvik GP, Klag M, et al. Reporting genetic results in research studies: summary and recommendations of an NHLBI working group. Am J Med Genet A. 2006;140:1033–1040. doi: 10.1002/ajmg.a.31195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kefford RF, Bishop JAN, Bergman W, Tucker MA. Counseling and DNA testing for individuals perceived to be genetically predisposed to melanoma: a consensus statement of the Melanoma Genetics Consortium. J Clin Oncol. 1999;17:3245–3251. doi: 10.1200/JCO.1999.17.10.3245. [DOI] [PubMed] [Google Scholar]
- 27.Rosenstock IM. Historical origins of the Health Belief Model. Health Educ Monogr. 1974;2:328–335. [Google Scholar]
- 28.Fernandez CV, Kodish E, Shurin S, Weijer C. Offering to return results to research participants: attitudes and needs of principal investigators in the Children's Oncology Group. J Pediatr Hematol Oncol. 2003;25:704–708. doi: 10.1097/00043426-200309000-00006. [DOI] [PubMed] [Google Scholar]
- 29.Shalowitz DI, Miller FG. Disclosing individual results of clinical research: implications of respect for participants. JAMA. 2005;294:737–740. doi: 10.1001/jama.294.6.737. [DOI] [PubMed] [Google Scholar]
- 30.McGuire AL, Beskow LM. Informed consent in genomics and genetic research. Annu Rev Genomics Hum Genet. 2010;11:361–381. doi: 10.1146/annurev-genom-082509-141711. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Cooper DN, Chen J-M, V Ball E, Howells K, Mort M, Phillips AD, et al. Genes, mutations, and human inherited disease at the dawn of the age of personalized genomics. Hum Mutat. 2010;31:631–655. doi: 10.1002/humu.21260. [DOI] [PubMed] [Google Scholar]