

Abstract
Femoral head fractures associated with acetabular fractures are usually treated by an open method. After a closed reduction of a hip dislocation, open reduction and internal fixation of acetabular fractures usually depend on the type of acetabular fracture. Acetabular fractures associated with femoral head fractures, torn labrums, or osteochondral fractures are often managed simultaneously by a posterior approach. The patient in this study was referred to us because of pain and limited motion after open reduction and internal fixation of an acetabular fracture. Postoperative computed tomography showed remnant osteochondral fragments located in the cotyloid fossa. Using hip arthroscopy, we found a torn labrum and multiple osteochondral fragments in the cotyloid fossa. The avulsed torn labrum was reattached with 2 anchors through the midanterior portal. Osteochondral fragments were curetted and removed. This article reviews the treatment of the torn labrum and multiple fragments after acetabular fracture reduction. The patient recovered immediately and had a satisfactory outcome. We conclude that hip arthroscopy is a valuable option for treating femoral head fracture dislocations associated with acetabular fractures.
Fractures of the femoral head associated with posterior dislocation of the hip are uncommon.1,2 They occur as a shearing injury as the flexed hip is driven across the posterior wall of the acetabulum during dislocation. Small inferior fragments of the femoral head tend to be free of soft-tissue attachments, whereas larger fragments are frequently still connected to the acetabulum by the ligamentum teres.3 Pipkin4 classified these fractures according to their morphology and their relation to femoral neck or acetabular fractures. Treatment of isolated femoral head fractures after posterior hip dislocation has been controversial. However, appropriate treatment of these fractures is of prime importance to help prevent the development of post-traumatic osteoarthritis.5
Pipkin type I and II fractures are treated by excision in the case of displaced small osteochondral fragments. Large displaced fracture fragments are internally fixed by redislocation. In the case of associated acetabular posterior wall fractures (Pipkin type IV), there are various ways to manage the acetabular and femoral head fractures. The management of these associated fractures depends on their size and location. Generally, a posterior approach is used that allows for simultaneous management of posterior wall fractures. In addition, an anterior approach can be used for femoral head fractures.
Hip arthroscopy is used increasingly as a less invasive surgical procedure for diagnosing and treating femoroacetabular impingement and for extracting loose bodies in hip trauma.6 It is hypothesized that hip arthroscopic surgery may become an alternative method for treating hip pain of unknown origin after hip trauma and/or neglected femoral head fractures. The use of arthroscopic techniques may also decrease morbidity compared with open excisions. We performed hip arthroscopy for neglected femoral head fractures of Pipkin type IV and report a successful outcome.
Case
A 45-year-old man was transferred to our clinic after a car accident. He sustained a posterior dislocation and acetabular posterior wall fractures of the right hip (Fig 1A). There was no associated neurologic damage to the lower extremity. The hip was promptly reduced by closed manipulation (Fig 1B). Plain radiographs confirmed the reduction of the hip as well as displaced acetabular posterior wall fractures. A computed tomography scan showed that multiple osteochondral fragments were located in the cotyloid fossa (Fig 2A). The patient underwent open reduction and internal fixation of the posterior wall of the acetabulum with a plate. Two months after the procedure, he complained of mild discomfort in the terminal cross-leg position. A follow-up computed tomography scan showed remnant osteochondral fragments that had not been completely removed (Fig 2B). A physical examination identified anterior inguinal pain and some limitation of internal rotation. We diagnosed femoroacetabular impingement due to a labral tear and loose bodies in the joint. However, in this case we could not perform magnetic resonance arthrography because of a metal artifact. We decided to remove the osteochondral fragments and to repair the torn labrum using hip arthroscopy.
Fig 1.
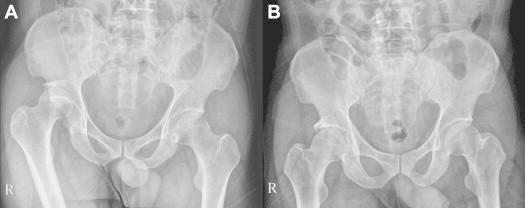
(A) The preoperative pelvis anteroposterior view shows posterior hip dislocation. (B) After reduction of the dislocated hip, the pelvis anteroposterior view shows reduction of the femoral head.
Fig 2.
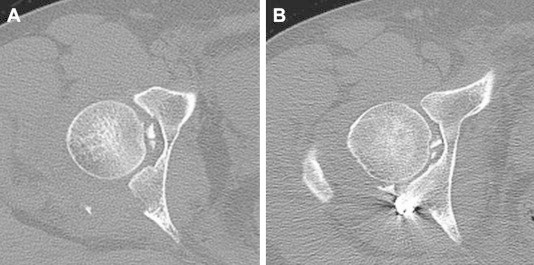
(A) The preoperative computed tomography scan shows osteochondral fragments in the joint. (B) After plate fixation to the posterior wall of the acetabulum, the computed tomography scan shows several remnants of osteochondral fragments in the joint.
Surgical Technique
The patient was treated in the supine position on a commercially available hip arthroscopy distraction unit (Smith & Nephew, Andover, MA). We used a conventional anterolateral viewing portal and an anterior working portal and examined the joint space with a 70° arthroscope. After a blood clot and the bloody joint fluid had been aspirated, we examined the joint space and found the torn labrum: an avulsion fracture torn away from the anterior wall of the acetabulum. We also found several osteochondral fragments in the cotyloid fossa. A capsulotomy was performed through the anterior to anterolateral site. The medial side of the labrum was detached and freely moved in the joint (Fig 3A). We then made an accessory midanterior portal to reattach the torn labrum. At first, a medial margin of the torn labrum was grasped with an arthroscopic grasper through the anterior portal, and the first anchor (2.3-mm Bioraptor; Smith & Nephew) was inserted through the midanterior portal. We used a loop-around technique and performed refixation of it on the detached site (Fig 3B). Then the second anchor was fixed at the mid portion of the torn labrum. Finally, we checked the stability with regard to the labrum integrity.
Fig 3.
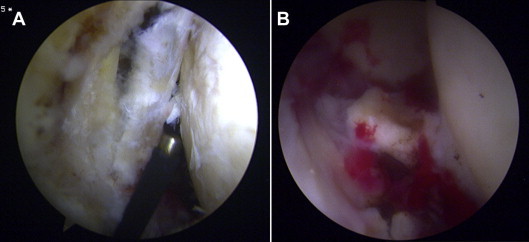
(A) The arthroscopic view shows the torn labrum and medial end detached from the anterior wall. (B) A large osteochondral fragment can be seen.
After curettage of the osteochondral fragments, a large fragment moved freely, so we continued drainage through the cannula. A large osteochondral fragment cannot be removed with an arthroscopic shaver (Fig 4), so we used a grasper (Fig 5). After completely removing the osteochondral fragments, we checked the stability of the torn labrum and fracture line again (Video 1). We then performed capsular closure along the longitudinal section of the T-shaped capsulotomy. The patient was allowed to take a non–weight-bearing walk with crutches 3 days after surgery. At last follow-up, he had excellent cosmetic results, had no pain, and had no motion limitations.
Fig 4.
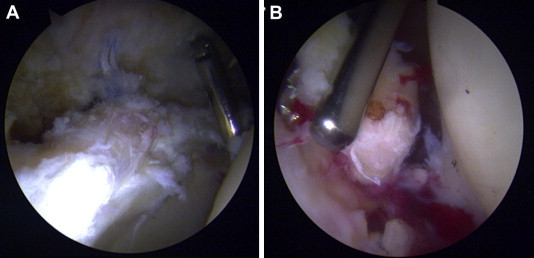
(A) Arthroscopic views show the reattached torn labrum. (B) A large osteochondral fragment cannot be removed with an arthroscopic shaver. We therefore removed it using a grasper.
Fig 5.
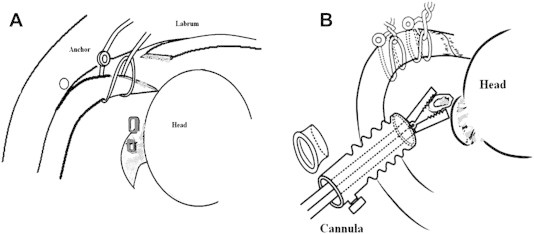
(A) Illustration of torn labrum and its reattachment using a loop-around technique. (B) Large osteochondral fragments were removed with a grasper.
Discussion
Fractures of the femoral head are relatively uncommon injuries. They make up approximately 6% to 15% of traumatic hip dislocation cases.3,7 Most often they are posterior, but there are also some anterior dislocations. This worsens the prognosis for the dislocation, with spontaneous evolution to osteoarthritis in more than 50% of cases.3 The management of femoral head fractures is controversial after a reduction of the hip dislocation. This may be achieved either surgically or nonsurgically. The size, location, and displacement of the fracture are all factors in this decision-making process. Nonsurgical treatment of femoral head fractures is acceptable when anatomic reduction is achieved and the hip joint is stable or if the fracture is inferior to the fovea and not problematic. The surgical indications include nonanatomic reduction of the femoral head articular surface, an unstable hip joint, and the presence of intra-articular incarcerated fragments that are preventing a congruent joint reduction. Controversies exist about whether fragments should be internally fixed or simply excised. Patients who have undergone surgical excision tend to have fracture patterns that are not amenable to fixation. Most surgeons agree that the factors that influence the treatment decision include fragment size, degree of comminution, and location of the fragment in relation to the weight-bearing surface of the femoral head.8 For a fracture fragment that is large enough to allow internal fixation, one should attempt to anatomically reduce and internally fixate the fragment with the goal of leaving the femoral head articular surface smooth. There are some disadvantages to open reduction because arthrotomy and redislocation can potentially further disrupt the vascular arcade because the hip's circulation is complex and disrupted by dislocation. Traditionally, the main approaches have been anterior (Smith-Petersen approach) and posterior (Kocher-Langenbeck approach). Recently, a posterior-based approach with a trochanteric flip osteotomy and surgical dislocation of the hip gained popularity among surgeons, given the wide exposure and visualization that are obtained.9 In this case the posterior wall is managed through a posterior approach and closed treatment of the femoral head fracture because concentric reduction was achieved preoperatively.
A recent review of the orthopaedic literature documents the use of arthroscopic hip surgery in trauma including removal of post-traumatic osteochondral loose bodies and interposed tissues. Lansford and Munns10 reported hip arthroscopic excisions of small fragments in a Pipkin type I fracture. Recently, Matsuda11 reported internal fixation of a suprafoveal fracture using hip arthroscopy (1 case), which had a good outcome.
In our case, pain and a limited range of motion were noted for full flexion and external rotation (as in femoroacetabular impingement). However, we could not obtain magnetic resonance imaging for our patient because of the presence of the metal artifact. We believe that hip arthroscopy is a useful method for diagnosing and treating labral damage and osteochondral fractures after hip trauma. Although hip arthroscopy is technically more demanding, it is less invasive and can be performed as an outpatient procedure. There are many advantages to using hip arthroscopy for hip trauma.12 It avoids operative hip dislocation and allows for early rehabilitation and outstanding cosmetic results (Table 1). However, there are concerns in relation to fluid extravasation creating compartment syndrome–type complications in the acute setting.13,14 There are no large series and there is little experience with respect to applying this technique to torn labral repair and removing osteochondral fragments. We believe that hip arthroscopy will become an indispensable procedure in cases in which magnetic resonance arthrography cannot be used because of the presence of metal artifacts, especially if there is pain of unknown origin after a hip trauma.
Table 1.
Critical Concepts in Hip Arthroscopy for Femoral Head Fracture and Hip Trauma
| Indications |
| Pain of unknown origin with or without loose bodies after hip trauma |
| Contraindications |
| Unstable hip joint caused by surrounding soft-tissue injuries |
| Pitfalls |
| Hip trauma |
| Clinical experience with femoroacetabular impingement surgery is needed. |
| Surgical techniques for a torn labrum are not like those for flap tears of the labrum, because on 1 side there is a tear and it is freely moving in the joint. An additional third portal should be made on the midanterior side; this can be used in the capsular repair procedure also. Through the anterior portal, the surgeon should grasp the medial border of the torn labrum. The reattachment procedure should be performed through the midanterior portal. |
| Capsulotomy |
| To examine the inner joint space, a T-shaped capsulotomy is preferred. Although capsulotomy is typically made along the midneck region, we prefer going through the midanterior portal. This allows for better visualization of the head-neck area and all around the labrum. |
| Torn labrum |
| Torn labrum should be reattached to its original site with a suture anchor. |
| Loose bodies or osteochondral fragments |
| Loose bodies or osteochondral fragments are usually impacted in the cotyloid fossa, but some are also impacted on the articular surface. These fragments are not easily removed with a hip arthroscopic shaver alone; sometimes they need curettage. Some larger fragments cannot be removed by a grasper, but it is much better to remove fragments by a grasper or shaver. |
| Advantages |
| Excellent cosmetic results are obtained. |
| Early ambulation and rehabilitation are permitted. |
| Disadvantages |
| Surgical skill in hip arthroscopic surgery is required. |
| The procedure is recommended for skillful hip arthroscopists only. An inexperienced hip arthroscopist may damage the chondral part by, for example, scuffing. |
| Sometimes surgeons should be willing to open the hip joint if hip arthroscopy does not allow proper examination of the hip joint. |
| Tip and pearls |
| The surgeon should start with hip traction and always use a cannula for labral reattachment and removal of osteochondral fragments. |
| Labral side: torn labrum (same as an avulsion fracture) |
| Reattach the flap-like tear (as in femoroacetabular impingement). |
| If 1 side is detached, the tear side should be grasped or fixed to the margin and reattached by a loop-around technique made at the midanterior portal. |
| We think that using a mattress stitch may do more damage to the torn labrum. |
| Osteochondral fragments |
| Fragments located in the joint should be curetted first; a shaver alone is not enough. |
| The surgeon should use a grasper for large fragments and remove them through a cannula. (If one is using a gasper, the cannula's rubber side or silicone valve should be opened first.) |
| Take-home messages |
| To diagnose pain of unknown origin or limited range of motion after hip trauma is difficult with magnetic resonance imaging because of metal artifact. |
| Hip arthroscopy now presents useful alternative methods for diagnosis and treatment in the trauma setting. |
| Hip arthroscopic management should be performed only after one has significant experience with femoroacetabular impingement. |
Footnotes
The authors report that they have no conflicts of interest in the authorship and publication of this article.
Supplementary data
This video shows our hip arthroscopic technique for pain of unknown origin and limited range of motion after acetabular fracture (Pipkin type IV). The arthroscopic view shows the torn labrum (like an avulsion rim fracture) and remnant loose bodies. These lesions were successfully treated with hip arthroscopy.
References
- 1.Matsuda D.K. A rare fracture, an even rarer trauma: The arthroscopic reduction and internal fixation of an isolated femoral head fracture. Arthroscopy. 2009;25:408–412. doi: 10.1016/j.arthro.2009.01.011. [DOI] [PubMed] [Google Scholar]
- 2.Ledere S., Tauber M., Karpik S., Bogner R., Auffarh A., Resch H. Fractures of the femoral head. A multicenter study. Unfallchirurg. 2007;110:513–520. doi: 10.1007/s00113-007-1246-2. (in German) [DOI] [PubMed] [Google Scholar]
- 3.Epstein H.C., Wiss D.A., Cozen L. Posterior fracture dislocation of the hip with fractures of the femoral head. Clin Orthop Relat Res. 1985:9–17. [PubMed] [Google Scholar]
- 4.Pipkin G. Treatment of grade IV fracture dislocation of the hip. J Bone Joint Surg Am. 1957;39:1027–1042. [PubMed] [Google Scholar]
- 5.Sahin V., Karakas E.S., Aksu S. Traumatic dislocation and fracture-dislocation of the hip. A long-term follow-up study. J Trauma. 2003;54:520–529. doi: 10.1097/01.TA.0000020394.32496.52. [DOI] [PubMed] [Google Scholar]
- 6.Haupt U., Volkle D., Waldherr C., Beck M. Intra- and retroperitoneal irrigation liquid after arthroscopy of the hip joint. Arthroscopy. 2008;24:966–968. doi: 10.1016/j.arthro.2007.02.019. [DOI] [PubMed] [Google Scholar]
- 7.Thompson V.P., Epstein H.C. Traumatic dislocation of the hip: A survey of two hundred and four cases covering a period of twenty-one years. J Bone Joint Surg Am. 1951;33:746–778. [PubMed] [Google Scholar]
- 8.Ross J.R., Gardner M.J. Femoral head fractures. Curr Rev Musculoskeletal Med. 2012;5:199–205. doi: 10.1007/s12178-012-9129-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ganz R., Gill T.J., Gautier E., Krugel N., Berlemann U. Surgical dislocation of adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br. 2001;83:1119–1124. doi: 10.1302/0301-620x.83b8.11964. [DOI] [PubMed] [Google Scholar]
- 10.Lansford T., Munns S.W. Arthroscopic treatment of Pipkin type I femoral head fractures: A report of 2 cases. J Orthop Trauma. 2012;26:e94–e96. doi: 10.1097/BOT.0b013e3182323f4f. [DOI] [PubMed] [Google Scholar]
- 11.Matsuda D.K. A rare fracture, an even rarer treatment: The arthroscopic reduction and internal fixation of and isolated femoral head fracture. Arthroscopy. 2009;25:408–412. doi: 10.1016/j.arthro.2009.01.011. [DOI] [PubMed] [Google Scholar]
- 12.Yamamoto Y., Ide T. Usefulness of arthroscopic surgery in hip trauma cases. Arthroscopy. 2003;19:269–273. doi: 10.1053/jars.2003.50033. [DOI] [PubMed] [Google Scholar]
- 13.Bartlett C.S., DiFelice G.S., Buly R.L., Quinn T.J., Green D.S., Helfet D.L. Cardiac arrest as a result of intraabdominal extravasation of fluid during arthroscopic removal of a loose body from hip joint of a patient with an acetabular fracture. J Orthop Trauma. 1998;12:294–299. doi: 10.1097/00005131-199805000-00014. [DOI] [PubMed] [Google Scholar]
- 14.Sampson T.G. Arthroscopic treatment of femoroacetabular impingement. Tech Orthop. 2005;20:56–62. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
This video shows our hip arthroscopic technique for pain of unknown origin and limited range of motion after acetabular fracture (Pipkin type IV). The arthroscopic view shows the torn labrum (like an avulsion rim fracture) and remnant loose bodies. These lesions were successfully treated with hip arthroscopy.