

Abstract
On February 21, 2013, 6 elderly people collapsed abruptly after eating bean sprout bibimbab (boiled rice mixed with bean sprouts and seasoned with soybean sauce) at a countryside restaurant in the Chungbuk Province, Korea. Minutes after eating the meal, all of the patients lapsed into a state of stupor. Respiratory arrest developed in 2 patients; and one of two patients died of cardiac arrest. The autopsy identified methomyl and methanol in the deceased patient's gastric contents and in the remaining soybeanbean sauce seasoning. Five of the 6 patients ingested one spoonful of the soybeanbean sauce seasoning and survived, while one patient who died of cardiac arrest, ingested approximately two spoons. Symptoms of toxicity presented quickly in the subjects and progressed rapidly, including chest tightness, an unusual sensation in the pit of the stomach, dizziness, ataxia, and finally, collapse. Three patients who drank ethanol with the meal experienced only mild toxic symptoms. Our analysis of the clinical observations in these cases suggests that ingestion of methomyl pesticide and the additive toxicity of methanol may have been responsible for the intoxication.
Keywords: Poisoning, Methomyl, Methanol, Mixture Toxicity
INTRODUCTION
Methomyl, methyl N-{[(methylamino)carbonyl]oxy}ethanimidothioate, is a cholinesterase inhibitor pesticide. In its pure form, it consists of colorless crystals with a slight sulfurous odor (1). Methomyl pesticide is generally produced as a liquid formulation, and it is stable in water for 30 days (1). Because of this, water and methomyl pesticide are relatively indistinguishable, which has contributed to methomyl pesticide being the subject of food-borne outbreaks (2-4). Methomyl has very high toxicity; the acute LD50 of methomyl is reportedly 30 mg/kg in rats (1). Consequently, the clinical outcome of patients with acute methomyl pesticide poisoning is generally critical. When ingested by humans, it is absorbed and metabolized rapidly, and readily excreted in the urine (1). As a cholinesterase inhibitor, the toxic symptoms of acute poisoning are similar to the cholinergic crisis that frequently results from acute organophosphate poisoning (2). While the production and marketing of methomyl pesticides have been discouraged by authorities since January 1, 2012, methomyl poisoning of humans was not uncommon in Korea.
On February 21, 2013, 6 elderly people collapsed abruptly after eating bean sprout bibimbab (boiled rice mixed with bean sprouts and seasoned with soybean sauce) in a countryside restaurant in the Chungcheongbuk-do of Korea. In this paper, we summarize the clinical features of these patients and discuss the logical validity of a diagnosis of methomyl and methanol poisoning in these cases.
MATERIALS AND METHODS
Patients
The 4 male patients in this case series (numbered cases 1-4 herein) all lived in the same neighborhood and used to share a meal together at a countryside restaurant managed by a long-term mutual friend. However, the owner of the restaurant had recently died and the owner's wife, along with a waitress, continued to operate the restaurant. All 4 male patients had been intimate with the restaurant owner (case 5) and the waitress (case 6). On the evening of the apparent poisoning, all 6 subjects of this report ate from the same dish bean sprout bibimbab for dinner. Within 3-5 min of eating the meal, all 6 subjects ran outside behaving as though they had been exposed to poisonous gas, reporting symptoms including chest tightness, an unusual sensation in the pit of the stomach, dizziness, ataxia, and a general feeling of uncomfortable heaviness of the body. Disoriented, they could not maintain a balanced posture and ultimately collapsed. All 6 patients were taken to a nearby primary care hospital within 30 min. The symptoms of toxicity appeared quickly following the meal, and progressed rapidly. After approximately 3 hr in the primary care hospital, each patient was transferred to one of 3 different general hospitals in Chung-Joo city, each of which was approximately a 1-hr drive from the scene.
Data collection
All clinical data reported herein were obtained retrospectively from hospital records. Four of the 6 patients visited our pesticide institute at the Soonchunhyang Hospital to complete the therapy; patient 4 died in hospital, and patient 5 (the restaurant owner) undertook therapy in another hospital. The initial data was obtained from the medical records of each hospital. A brief telephone interview was conducted with patient 5, the restaurant owner, 19 days after the incident. The results of the autopsy on the deceased patient (case 4) and the existence of both methomyl and methanol in the gastric contents and the remaining uneaten food were noted by the health authority of the Province. The circumstances surrounding the demise of the deceased patient (case 4) were derived from information provided by the other patients reported herein, i.e., patients 1-3, 5, and 6."
Ethics statement
The study protocol and design were approved by the institutional review board of Soonchunhyang University Cheonan Hospital (IRB approval number: 2013-65). Informed consent was not obtained due to the retrospective design of the study.
RESULTS
Six elderly people collapsed abruptly after eating bean sprout bibimbab (boiled rice mixed with bean sprouts and seasoned with soybean sauce). A primary care physician treated them for food poisoning; however, the symptoms became more serious over time; and all of the patients lapsed into a state of stupor. Respiratory arrest developed in 2 patients; and one of these patients subsequently died of cardiac arrest. The autopsy detected methomyl and methanol in that patient's gastric contents, and it was also detected in the remaining soybean sauce seasoning (patient 4). The individual cases were described as follows (Table 1).
Table 1.
Laboratory findings of the cases
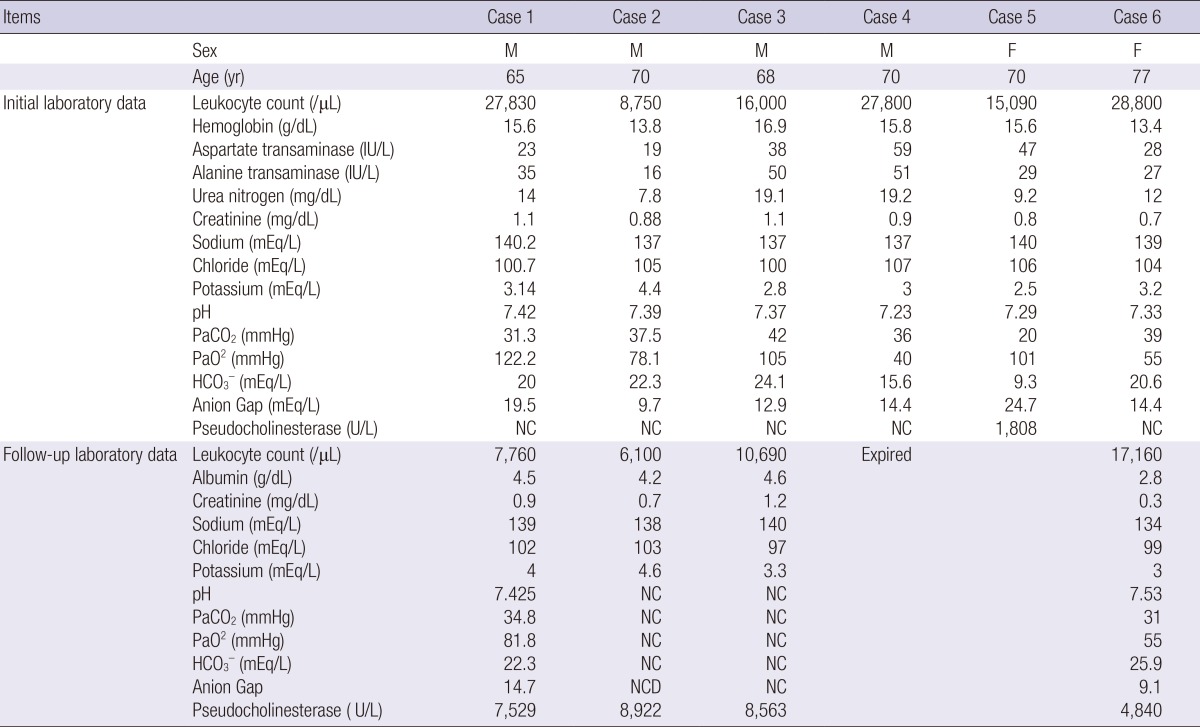
NC, not checked. Anion gap is calculated as [Na+]-{[Cl-] + [HCO3-]}. Note that the anion gap is greater than 16 mEq/L in cases 1 and 5. The initial pseudocholinesterase level was only measured in case 5 and was lower than the reference range of 3,400-14,200 U/L. The early laboratory data was obtained at the first general hospital visited. The late laboratory data was obtained between 6 and 19 days after the meal, at the Pesticide Intoxication Institute of Soonchunhyang University Hospital.
Patient 1 was a 65-yr-old man weighing 70 kg. He had been healthy without specific difficulties in performing activities of daily living, despite a medical history of a cerebral hemorrhage in 2009. On the evening of the reported event, he suddenly felt dizzy after eating the meal, left the restaurant, and collapsed. He attempted to call for emergency assistance with his cell phone, but was unable to do so due to the sudden onset of visual and sensorimotor dysfunction. He exhibited diarrhea, nausea, vomiting, and incoherence. Despite hospitalization, he did not exhibit coherence until the following morning. He was treated conservatively for food poisoning until the authorities announced that the autopsy results from case 4 had suggested methomyl poisoning. He was discharged from the hospital on day 6 after the symptoms of toxicity had apparently subsided. However, symptoms of headache, nausea, and weakness persisted. Eight days after the incident, he visited our pesticide intoxication institute. His blood pressure (BP) was 140/80 mmHg, pulse rate was 90/min, and body temperature (BT) was 37℃. He was alert, and no pathological neurologic reflex was observed.
Patient 2 was a 70-yr-old man weighing 65 kg. After the meal, he immediately developed abdominal discomfort and generalized muscle aches. He experienced a rapid onset of dizziness and a feeling of oncoming diarrhea. He did not become disoriented, but lost his sense of balance. He tried to call for emergency assistance, but could not because he was unable to read the text on his cell phone. The appetizer that he had consumed prior to the meal contained approximately 120 mL of 20% ethanol, and patients 3 and 5 also consumed the same appetizer. His toxic symptoms were much less severe than those of the other patients. He was treated in the hospital for food poisoning and discharged on the 3rd hospitalization day. He visited our pesticide intoxication institute 19 days after the incident for a follow-up examination. On arrival, he exhibited a clear mental status, BP of 120/70 mmHg, pulse rate of 77/min, BT of 36℃, stable vital signs, and no pathological neurologic reflex.
Patient 3 was a 68-yr-old man weighing 76 kg. Immediately after the meal, he experienced dizziness and vertigo. During the meal, he had consumed an appetizer containing approximately 100 mL of 20% ethanol, as had patients 2 and 5. He lost his balance and fell to the ground, but did not lose consciousness. He was treated for food poisoning in the hospital for 3 days, and did not exhibit loss of consciousness throughout his stay in hospital. On 8 days after the incident, he visited our pesticide intoxication institute for a follow-up examination. BP was 150/90 mmHg, pulse rate was 70/min, and BT was 36.5℃. No pathological neurologic reflex was observed.
Patient 4 was a 67-yr-old man of average size who was previously of good health, as assessed by his friends. The survivors all remembered that while they had added approximately 1 spoonful of soybean sauce seasoning to the meal, he had added approximately twice that amount. After the meal, he experienced vomiting and diarrhea and became unconscious. After endotracheal intubation at the primary care clinic, he was transferred to a general hospital in a comatose state. In the emergency room, his BP was 180/120 mmHg, pulse rate was 120/min, and BT was 37℃. Respiration was shallow and slow, with a rate of 7/min. Mechanical ventilation was initiated. The results of a portable emergency chest radiograph were compatible with acute respiratory distress syndrome. He exhibited pin-point pupils and increased bronchial secretions. On day 3, he died of cardiac arrest.
Patient 5 was owner of the restaurant, and was a 70-yr-old average-sized woman. She drank approximately 120 mL of 20% ethanol as an appetizer with patients 2 and 3. Immediately after the meal, she experienced dizziness and vertigo, and was transferred to hospital. High anion gap metabolic acidosis detected in the emergency room led the duty doctor to suspect methanol intoxication. Serum methanol level was 12.0 mg/L approximately 5 hr after the meal, as measured by gas chromatography-mass spectrometry at the emergency department. Several hours after arrival, hypotension (80/56 mmHg) and T inversion on precordial ECG lead were observed. Echocardiogram showed akinesia of the left ventricle and the left ventricle ejection fraction was less than 30%. After conservative treatment, the patient recovered quickly. On the 5th hospital day, her pseudocholinesterase level was 5,800 U/L (reference range of 3,400-14,200 U/L). After conservative treatment for 6 days, she was discharged without sequelae. A brief telephone interview was conducted with her after her discharge on 19 days after the meal. She was in shock about the incident, but no major problems were apparent with regard to her physical condition.
Patient 6 was waitress of the restaurant, a 77-yr-old woman weighing 48 kg. She experienced dizziness within 5 min of the meal and vomited. She ran outside, collapsed on the ground, and lost consciousness. Immediately after arrival at hospital, she developed respiratory arrest and underwent emergency tracheal intubation followed by mechanical ventilation. The following day, the physician noted increased bronchial secretions with wheezing sounds upon lung examination. Unconvinced of a diagnosis of cholinesterase inhibitor toxicity, the physician injected atropine (unfortunately, they did not measure her cholinesterase level). Six days later, the patient was transferred to our pesticide intoxication institute with tracheal intubation. Her symptoms of toxicity subsided rapidly. Two days later, the tracheal tube was removed. She was discharged on the 10th hospitalization day without specific complaints.
DISCUSSION
The clinical characteristics observed in this case are very similar to those of a previous report (2). It is hard to understand why and how the toxic symptoms developed qucikely, 3-5 min after ingestion of the meals. In the current outbreak, the following points suggested that additive and/or synergistic toxicity of methomyl and methanol was responsible for the symptoms: Toxic symptoms developed early, within 5 min after the meals. This suggested that the poison was absorbed in the stomach. Methanol is rapidly and completely absorbed after oral ingestion, reaching a peak serum methanol concentration within 1-2 hr. The initial symptoms of methanol intoxication included central nervous system depression, headache, dizziness, nausea, lack of coordination, confusion, and with sufficiently large doses, unconsciousness, and death. Methanol is highly toxic to humans. If ingested, as little as 10 mL of pure methanol can cause permanent blindness through destruction of the optic nerve. Approximately 30 mL is potentially fatal, although the median lethal dose is typically 100 mL (1-2 mL/kg of pure methanol) (6). Four of the patients (cases numbered 1, 2, 3, and 6) stated that they experienced visual impairment during the first a few days after the incident. However, ocular examinations conducted on days 7 or 8 showed no specific abnormalities in visual acuity, visual field, or anterior segment and fundus in any of the patients.
Acute methanol poisoning is often accompanied by metabolic acidosis with an elevated anion gap (7). In the cases reported herein, the method used for the measurement of the anion gap consisted of colorimetry for HCO3- and Cl- as well as flame photometry for Na+ and K+. Anion gap was high in case 1 (19.5 mEq/L) and case 5 (24.7 mEq/L). There are 2 types of methomyl pesticide products in Korea: water-dispersible powder and a liquid formulation. In liquid formulations, methanol is usually the solvent used, and the solvent comprises approximately 75% of the volume of methomyl pesticide products. Therefore, when humans ingest methomyl pesticide in liquid formulation, they ingest a volume of methanol 3 times greater than the amount of methomyl ingested. In general, the effects of ingesting a combination of 2 toxic chemicals are either additive, synergistic, or inhibitory (8, 9). Further research is required to determine whether the toxicity of methomyl and methanol is synergistic.
Recently, we reported a separate case of a 49-yr-old man with acute methanol intoxication that occurred after ingestion of a methomyl pesticide (10). He was brought to the emergency department in an unconscious state after ingestion of 20 mL of a methomyl pesticide. Upon arrival, he was semi-comatose and did not breathe spontaneously. However, his cholinesterase level was normal level and cholinergic symptoms were not observed. His urine methanol level was 55.60 mg/dL, and he was treated with hemodialysis. Subsequently, his metabolic acidosis resolved and his mental status returned to normal.
The symptoms of toxicity were comparatively mild in the 3 cases in which an ethanol drink was consumed during the meal. It is well-known that the same alcohol dehydrogenase enzyme competitively breaks down both ethanol and methanol. Therefore, the administration of ethanol during methanol intoxication reduces the rate of formic acid production. A concentration of 1 g/L of ethanol is known to be sufficient to fully block the degradation of methanol. Investigation of this incident is currently being conducted by the relevant authorities, to determine whether it was an accident or whether criminality may have been involved. Bearing in mind that the boiling point of methanol is 67.4℃ (11), we believe that the methomyl pesticide was added after the boiling of both the rice and the vegetables, either intentionally or accidently.
The clinical observations reported herein have some limitations. A police investigation into this incident is currently underway. All of the information pertaining to the investigation, including the autopsy findings, were provided by the Korean National Forensic Service. We were not permitted to make inquiries about details of the progress of the investigation.
The patients were treated at 3 different hospitals and the initial laboratory tests and the treatment modalities differed from hospital to hospital. Given this, summarizing common laboratory findings was problematic. Blood methanol level was only measured in 1 patient (case 5). Fortunately, in the emergency room of one of the hospitals, methanol measurement was a routine laboratory test for patients who showed high anionic gap acidosis.
In conclusion, we have reported an outbreak of methomyl pesticide intoxication that was mistaken for bacterial food poisoning. Toxic symptoms appeared within a few minutes after the meals and progressed rapidly. One patient who ingested a larger amount of the soybeanbean sauce seasoning than the others died. Three patients who drank ethanol during the meals experienced less severe symptoms of toxicity. Our analysis of clinical observations suggests that when a patient presents with the abrupt onset of unconsciousness after a meal, associated with high anion gap metabolic acidosis, methomyl pesticide intoxication is one of the conditions that the doctor should consider with regard to differential diagnosis.
Footnotes
This work was carried out with the support of "Cooperative Research Program for Agriculture Science & Technology Development (Project No. PJ008246)" Rural Development Administration, Republic of Korea.
The authors have no conflicts of interest to disclose.
References
- 1.Krieger R. Handbook of pesticide toxicology: vol. 2. classes of pesticides. New York: Academic Press; 2001. pp. 1087–1106. [Google Scholar]
- 2.Tsai MJ, Wu SN, Cheng HA, Wang SH, Chiang HT. An outbreak of food-borne illness due to methomyl contamination. J Toxicol Clin Toxicol. 2003;41:969–973. doi: 10.1081/clt-120026519. [DOI] [PubMed] [Google Scholar]
- 3.Buchholz U, Mermin J, Rios R, Casagrande TL, Galey F, Lee M, Quattrone A, Farrar J, Nagelkerke N, Werner SB. An outbreak of food-borne illness associated with methomyl-contaminated salt. JAMA. 2002;288:604–610. doi: 10.1001/jama.288.5.604. [DOI] [PubMed] [Google Scholar]
- 4.Shelton AM, Sances FV, Hawley J, Tang JD, Boune M, Jungers D, Collins HL, Farias J. Assessment of insecticide resistance after the outbreak of diamondback moth (Lepidoptera: Plutellidae) in California in 1997. J Econ Entomol. 2000;93:931–936. doi: 10.1603/0022-0493-93.3.931. [DOI] [PubMed] [Google Scholar]
- 5.Lee BK, Jeung KW, Lee HY, Jung YH. Mortality rate and pattern following carbamate methomyl poisoning. Comparison with organophosphate poisoning of comparable toxicity. Clin Toxicol (Phila) 2011;49:828–833. doi: 10.3109/15563650.2011.617309. [DOI] [PubMed] [Google Scholar]
- 6.Coulter CV, Farquhar SE, McSherry CM, Isbister GK, Duffull SB. Methanol and ethylene glycol acute poisonings - predictors of mortality. Clin Toxicol (Phila) 2011;49:900–906. doi: 10.3109/15563650.2011.630320. [DOI] [PubMed] [Google Scholar]
- 7.Kraut JA, Kurtz I. Toxic alcohol ingestions: clinical features, diagnosis, and management. Clin J Am Soc Nephrol. 2008;3:208–225. doi: 10.2215/CJN.03220807. [DOI] [PubMed] [Google Scholar]
- 8.Reffstrup TK, Larsen JC, Meyer O. Risk assessment of mixtures of pesticides: current approaches and future strategies. Regul Toxicol Pharmacol. 2010;56:174–192. doi: 10.1016/j.yrtph.2009.09.013. [DOI] [PubMed] [Google Scholar]
- 9.Junghans M, Backhaus T, Faust M, Scholze M, Grimme LH. Application and validation of approaches for the predictive hazard assessment of realistic pesticide mixtures. Aquat Toxicol. 2006;76:93–110. doi: 10.1016/j.aquatox.2005.10.001. [DOI] [PubMed] [Google Scholar]
- 10.Gil HW, Hong JR, Song HY, Hong SY. A case of methanol intoxication caused by methomyl pesticide ingestion. Hum Exp Toxicol. 2012;31:1299–1302. doi: 10.1177/0960327112459532. [DOI] [PubMed] [Google Scholar]
- 11.Sigma-Aldrich. Methanol. [accessed on 8 October 2013]. Available at http://www.sigmaaldrich.com/chemistry/solvents/methanol-center.html.