

Abstract
Purpose:
To verify the association between lower urinary tract symptoms (LUTS) and erectile dysfunction (ED) and evaluate the influence of sildenafil and doxazosin either as single agents or combined on both symptoms.
Material and Methods:
A prospective randomized study including 150 patients presented with LUTS caused by BPH in association with clinically diagnosed ED, with age equal or more than 45 years from April 2010 to April 20011. They were categorized into three comparative groups each one containing 50 patients. These groups were comparable regarding pretreatment international prostate symptoms score (IPSS) and international index of erectile function (IIEF). The patients of the first group were given sildenafil 50 mg as monotherapy, those of the second group were given doxazosin 2 mg and those of the third group were given combination of both drugs for 4 months for each group. The main post-treatment parameters for assessment and comparison include assessment of patient's symptoms by repeated IPS Sand IIEF, uroflowmetry and assessment of PVR. The statistics was done by use of the Qui--square test.
Results:
Pre-treatment parameters were assessed and compared between the three groups. After 4 months of treatment, the comparative parameters were applied to all groups and the differences were measured post-treatment regarding IPSS, erectile function score, uroflowmetry, and post-void residual (PVR) urine. Sildenafil alone caused mild improvement in IPSS, more improvement in IIEF score, and little effect on flow rate and PVR urine. Doxazosin alone caused more improvement in IPSS, flow rate and PVR urine and less improvement in IIEF score. A combination of both sildenafil and doxazosin caused more improvement in all of the comparative parameters than when each drug was given alone.
Conclusions:
There is a strong relationship between LUTS and ED. Doxazosin or sidenafil as a single drug could be used in treating mild or mild to moderate symptoms but more severe symptoms may usually need a combination of both drugs.
Keywords: Doxazosin, erectile dysfunction, lower urinary tract symptoms, sildenafil
INTRODUCTION
The prevalence of lower urinary tract symptoms (LUTS) associated with benign prostatic hyperplasia (BPH) and erectile dysfunction (ED) increases with age. The prevalence of BPH is very high, 40% of men have BPH by the age of 50 and this has increased to more than 80% by the age of 80. The prevalence of ED is similarly high and increases with age, 40% of 40 year-old men experience some degree of ED, and the rate is as much as 70% in 70 year old. Not surprisingly, both BPH and ED have a significant negative impact on the quality-of-life measures for aging men.[1]
As the prevalence of both ED and LUTS increases with age, physicians could be in the position to manage these two conditions simultaneously. Moreover, medical therapies for either one of these conditions can affect the other and this should be carefully considered when making treatment decisions.
Some alpha--1-adrenergic blockers have a positive impact on erection. This is the case for alfuzosin and doxazosin which have been shown to enhance erectile function in experimental models, probably by reducing the sympathetic tone and thus relaxing corpus cavernosum smooth muscle cells.[2]
Phosphodiesterase-5 (PDE-5) inhibitors are commonly used to treat ED. There is increasing evidence that they might also have a beneficial effect on LUTS, probably through the nitric-oxide pathway. Nitric oxide is an important mediator of the relaxation of isolated bladder and urethral smooth muscle and could modulate prostatic smooth muscle tone.[3]
Considering the high incidence of both ED and BPH in aging men, the ability to treat both disorders with a single agent such as a PDE-5 inhibitor would be valuable. Sildenafil is the first oral agent to be well documented as an effective form of treatment for men experiencing ED. Since its introduction in March 1996, no other therapy for ED has achieved such prominent public recognition.[4]
In this study, our aim is to perform a prospective randomized study to verify the association between LUTS and ED and evaluate the influence of sildenafil and doxazosineither as single agents or combined on both symptoms.
MATERIALS AND METHODS
This study is a prospective randomized study including 150 patients presented with LUTS caused by BPH in association with clinically diagnosed ED from April 2010 to April 2011. Patients eligible for this study are those with age equal or more than 45 years complaining of LUTS caused by BPH (after exclusion of other causes of LUTS) for 3 months or more with international prostate symptoms score (IPSS) more than 7associated with clinically diagnosed ED for also 3 months or more with erectile function score {assessed by international index of erectile function (IIEF) questionaire} less than 25.
Exclusion criteria include those patients with previous prostatic surgery or other less invasive surgical interventions for BPH, those with active urinary tract disease that may causes LUTS as cystitis or bladder stones, those with PSA >10, and those who are not candidates for medical treatment for ED (as patients with cardiac problems which contraindicate the use of PDE-5 inhibitors, patients who need surgical interventions or patients with previous unresponsiveness to PDE-5 inhibitors).
Patients of our study were categorized into three comparative groups each containing 50 patients. These groups were comparable regarding pretreatment (IPSS) and (IIEF). The patients of the first group were given sildenafil 50 mg as monotherapy, those of the second group were given doxazosin 2 mg, and those of the third group were given a combination of both drugs for 4 months for each group.
Pretreatment assessment was done for all patients, including complete medical history, assessment of the degree of both LUTS and ED using IPSS scoring system and international index for erectile function, complete physical examination including neurological assessment, laboratory investigations including CBC, random blood sugar level, lipid profile, serum creatinine, serum PSA, serum testosterone and LH and prolactin when indicated (in patients with low serum testosterone level), uroflowmetry, and PVR urine assessment.
The main post-treatment parameters for assessment and comparison include assessment of patient›s symptoms by repeated IPSSand IIEF, uroflowmetry, and assessment of PVR. The statistics was done by use of the Qui–square test.
RESULTS
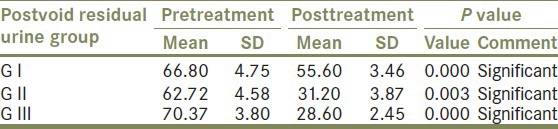
Of 272 men who were screened for eligibility, 150 subjects were randomized into three groups to receive either sildenafil 50 mg, doxazosin 2 mg, or a combination of both drugs. Pre-treatment and post-treatment parameters were assessed and compared between the three groups including mean IPSS [Table 1], mean erectile function score [Table 2], mean urine flow rate [Table 3], and mean PVR urine [Table 4].
Table 1.
IPSS score (pre and posttreatment)
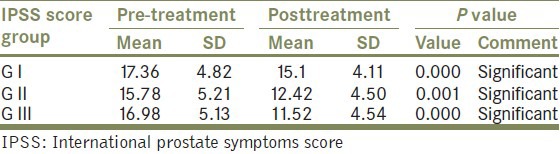
Table 2.
ED score (pre/posttreatment)
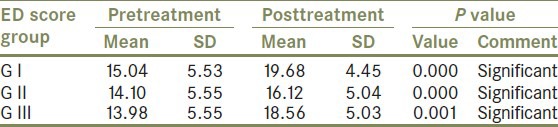
Table 3.
Urine flow rate (pre/posttreatment)
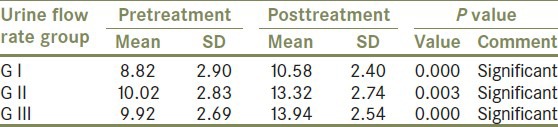
Table 4.
Post-void residual urine (pre/posttreatment)
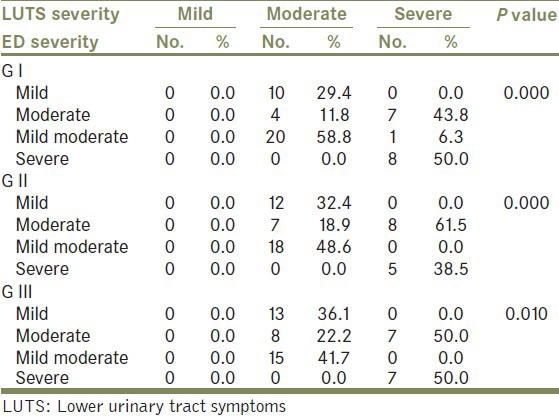
A strong relationship was detected between the severity of LUTS and the severity of ED [Table 5].
Table 5.
LUTS severity versus ED severity
There were no significant detectable side effects that mandated stoppage of treatment except for slight dizziness and blurring of vision especially in patients who took combination therapy with insignificant effect on blood pressure even in patients who took combination therapy.
DISCUSSION
There is a proven relationship between LUTS and ED through several etio-pathological mechanisms and LUTS were clearly identified as risk factors for ED; also, the severity of ED increases with increasing the severity of LUTS, this may be explained by several theories:
-
(1)
Role of alpha receptors with pelvic sympathetic overactivity: Role of alpha receptors with pelvic sympathetic ovreactivity: Heightened pelvic sympathetic tone leads to elevated local norepinephrine levels, which act on the alpha receptors in the cavernous smooth muscle to stimulate contraction.[5,6] The elevated local norepinephrine levels induce both vascular and cavernous smooth muscle contraction, producing an anti-erectogenic state. Alpha-Adrenergic receptor blockers block the effect of norepinephrine and can induce erection.[7]
-
(2)
Role of nitric oxide and bladder outlet obstruction: Experimental models were created in animals to test the effect of bladder outlet obstruction on cavernosal smooth muscle tissue. A recent study found that in rabbits with partial bladder outlet obstruction, there was impaired nitric oxide (NO)-mediated relaxation of bladder strips in vitro.[8]
-
(3)
Role of Rho-Kinase: Rho-kinase inhibits myosin light chain phosphatase and phosphorylates the myosin light chain promoting smooth muscle contraction. This pathway is responsible for the tonic contraction of cavernosal smooth muscle and the normal flaccid state of the penis. Inhibition of Rho-kinase acts synergistically with NO to promote erection and vasoconstrictors that impair erection operate through the Rho-kinase pathway. Inhibition of this pathway that is responsible for tonic contraction may promote erections.[9]
Some alpha adrenergic blockers used for treatment of LUTS caused by BPH have a positive erectogenic effect as doxazosin and alfuzosin; also, PDE-5 inhibitors have positive impact in decreasing the severity of LUTS most probably through NO pathway which mediates relaxation of bladder and prostatic smooth muscles.
In the first group of our patients, we tried to show the effect of sildenafil as a single drug on both symptoms after 4 months follow up [Tables 1 and 2]. This coincides with a study done by Ying et al., in which 32 patients with ED and BPH were offered oral sildenafil and reviewed before and 6 months after the administration of sildenafil by the (IIEF) and the (IPSS) questionnaires. After 6 months, IIEF-5 scores were increased by 42.36% and IPSS scores declined by 20.14%, with statistical significance (P < 0.01).[10]
In this study, the mean pre-treatment flow rate was 9.82 ml/sraised to 10.58 ml/s after 4 months of treatment (P = 0.000). CemGüler et al. reported that the Qmax. Of 38 patients with obstructive LUTS were evaluated before and after treatment with sildenafil 50 mg for 3 months The mean Qmax was 11.4 and 12.3 ml/s before and after sildenafil, respectively (P < 0.0001).[11] This relaxant effect of sildenafil on the prostatic smooth muscles may also explain its positive effect on PVR urine. In our study, the mean pre-treatment PVR urine was 65.8 ml and it decreased to 59.6 ml after 4 months of treatment (P = 0.000 0.).
From these results we noticed that sildenafil alone caused mild improvement in IPSS, more improvement in IIEF score and little effect on flow rate and PVR urine.
In the second group of our patients, we tried to show the effect of doxazosin as a single drug on both symptoms after 4 months follow up [Tables 1 and 2]. This coincides with a study done by Demir et al.[12] In this study 53 patients with LUTS (IPSS score >7) whose maximum flow rate (Qmax) was <15 ml/s were enrolled in the study. Patients received doxazosin 2 mg once daily for 6 weeks. Subjective efficacy was assessed by IPSS for LUTS and efficacy was assessed by (IIEF) for erectile functions at baseline and sixth week. The objective efficacy was assessed by (Qmax). At the endpoint, doxazosin significantly improved the mean total IPSS score (4.7) (P = 0.001), and mean Qmax (+3.2 ml/s) (P = 0.002) over baseline. The mean improvement of IIEF scores after the treatment period was (+2.3) (P = 0.0002).
The mean pretreatment flow rate was 10.02 ml/s raised to 12.32 ml/s after 4 months of treatment (P = 0.000). This also coincide with the previous study done by Demir et al.[12] This means that doxazosin is better in improving urine flow rate than sildenafil.
The mean pre-treatment PVR urine was 66.7 ml and decreased to 41.2 ml after 4 months of treatment (P = 0.0001) which is better than the first group. This means that doxazosin has better effect in reducing PVR than sildenafil.
From these results, we noticed that doxazosin alone caused more improvement in IPSS, flow rate, and PVR urine and lesser improvement in IIEF score.
In the third group of our patients, we tried to show the effect of combination therapy by both doxazosin and sildenafil on both symptoms after 4 months follow up [Tables 1-4]. This correlates with a pilot study done by Steven A. Kaplan[2] to assess the efficacy and safety of the alpha-1-blocker doxazosin 2 mg once daily (OD), the PDE-5 inhibitor sildenafil 50 mg OD, and the combination of both on UTS suggestive of. Men aged 50–76 years with previously untreated LUTS and ED were randomized to receive doxazosin (n = 20), sildenafil (n = 21), or the combination of both (n = 21) for 12 weeks. Changes from baseline in international prostate symptom score (IPSS), maximum urinary flow rate (Qmax), (PVR urine volume, and erectile function domain of the international index of erectile function (IIEF) were assessed at week 12. He showed that improvement of IPSS was significant with the 3 months treatments but greatest with the combination (24.1%) compared with doxazosin (15.6%) and sildenafil (16.9%) alone (P < 0.03). PVR, and Qmax were significantly improved with doxazosin only and the combination. Improvement in IIEF was slight with doxazosin (16.7%), marked with sildenafil (49.7%), and greatest with the combination (58.6%).
From these results we noticed that acombination of both sildenafil and doxazosin caused more improvement in all of the comparative parameters than when each drug was given alone.
Correlation between LUTS and ED: From our results we found a strong relationship between the severity of LUTS and the severity of ED, and LUTS are well--documented risk factors for ED.
CONCLUSION
From the previously reviewed data we have reached to two important conclusions: First, there is a strong relationship between LUTS and ED; second, doxazosin or sidenafil as a single drug could be used in treating mild or mild to moderate symptoms but more severe symptoms may usually need a combination of both drugs in order to achieve patient satisfaction.
Footnotes
Source of Support: Nil
Conflict of Interest: None.
REFERENCES
- 1.Garraway WM, Kirby RS. Benign prostatic hyperplasia: Effects on quality of life and impact on treatment decisions. Urology. 2001;44:629–36. doi: 10.1016/s0090-4295(94)80194-0. [DOI] [PubMed] [Google Scholar]
- 2.Kaplan SA, Gonzalez RR, Alexis E. Combination of alfuzosin and sildenafil is superior to monotherapy in treating lower urinary tract symptoms and erectile dysfunction. Eur Urol. 2007;51:1717–23. doi: 10.1016/j.eururo.2007.01.033. [DOI] [PubMed] [Google Scholar]
- 3.Fink HA, MacDonald R, Rutks IR, Nelson DB, Wilt TJ. Sildenafil for male erectile dysfunction. A systematic review and meta-analysis. Arch Intern Med. 2002;162:1349–60. doi: 10.1001/archinte.162.12.1349. [DOI] [PubMed] [Google Scholar]
- 4.Boolell M, Allen MJ, Ballard SA, Gepi-Attee S, Muirhead GJ, Naylor AM, et al. Sildenafil: An orally active type 5 cyclic GMP-specific phosphodiesterase inhibitor for the treatment of penile erectile dysfunction. Int J Impot Res. 1996;8:47–52. [PubMed] [Google Scholar]
- 5.Levin RM, Wein AJ. Adrenergic alpha receptors outnumber beta receptors in human penile corpus cavernosum. Invest Urol. 1980;18:225–6. [PubMed] [Google Scholar]
- 6.Traish A, Kim NN, Huang YH, Goldstein II, Moreland RB. Cyclic AMP regulates mRNA expression of alpha-1d and alpha-2a adrenergic receptors in cultured human corpus cavernosum smooth muscle cells. Int J Impotence Res. 2000;12(suppl 1):41–7. [PubMed] [Google Scholar]
- 7.Brindley GS. Cavernosal alpha-blockade: A new technique for investigating and treating erectile impotence. Br J Psychiatry. 1983;143:332–7. doi: 10.1192/bjp.143.4.332. [DOI] [PubMed] [Google Scholar]
- 8.Calvert RC, Khan MA, Thompson CS, Dashwood MR, Mikhailidis DP, Morgan RJ. Anaheim, Calif: Paper presented at: American Urological Association Annual Meeting; 2001. Jun, Alterations in nitric oxide signaling provides insight into the pathophysiology of erectile dysfunction associated with benign prostatic hyperplasia. [Google Scholar]
- 9.Wingard CJ, Husain S, Williams J, James S. RhoA-Rho kinase mediates synergistic ET-1 and phenylephrine contraction of the rat corpus cavernosum. Am J Physiol Regul Integr Comp Physiol. 2003;285:1145–52. doi: 10.1152/ajpregu.00329.2003. [DOI] [PubMed] [Google Scholar]
- 10.Ying J, Yao D, Jiang Y, Ren X, Xu M. The positive effect of sildenafil on LUTS from BPH while treating ED. Zhonghua Nan Ke Xue. 2004;10:681–3. [PubMed] [Google Scholar]
- 11.Güler C, Roehrborn CG, Kaminetsky JC, Auerbach SM, Wachs B, Young JM. Sildenafil relieves lower urinary tract symptoms secondary to benign prostatic hyperplasia. J Urol. 2007;177:1401–7. doi: 10.1016/j.juro.2006.11.037. [DOI] [PubMed] [Google Scholar]
- 12.Demir O, Murat N, Aslan G, Gidener S, Esen AA. Effect of doxazosin with and without rho-kinase inhibitor on human corpus cavernosum smooth muscle in the presence of bladder outlet obstruction. J Urol. 2006;175:2345–9. doi: 10.1016/S0022-5347(06)00281-3. [DOI] [PubMed] [Google Scholar]