

Abstract
Objectives:
To determine the relations between obstructive sleep apnea (OSA) diagnosis, the likelihood of being diagnosed with a psychological condition, among obese veterans, after accounting for severity of obesity and the correlated nature of patients within facility. We hypothesized that (1) individuals with a diagnosis of OSA would be more likely to receive a diagnosis of a (a) mood disorder and (b) anxiety disorder, but not (c) substance use disorder.
Design:
Cross-sectional retrospective database review of outpatient medical records between October 2009 and September 2010, conducted across all 140 Veterans Health Administration (VHA) facilities.
Setting:
The entire VA Health Care System.
Patients or Participants:
Population-based sample of veterans with obesity (N = 2,485,658).
Main Outcome Measures:
Physician- or psychologist-determined diagnosis of psychological conditions including mood, anxiety, and substance use disorders.
Results:
Using generalized linear mixed modeling, after accounting for the correlated nature of patients within facility and the severity of obesity, individuals with a diagnosis of sleep apnea had increased odds of receiving a mood disorder diagnosis (OR = 1.85; CI = 1.71-1.72; p < 0.001), anxiety disorder diagnosis (OR = 1.82; CI = 1.77-1.84; p < 0.001), but not a diagnosis of substance use disorder.
Conclusions:
Among obese veterans within VA, OSA is associated with increased risk for having a mood and anxiety disorder, but not substance use disorder, with the strongest associations observed for posttraumatic stress disorder (PTSD) and major depressive disorder (MDD). In addition, this relation remained after accounting for severity of BMI.
Citation:
Babson KA; Del Re AC; Bonn-Miller MO; Woodward SH. The comorbidity of sleep apnea and mood, anxiety, and substance use disorders among obese military veterans within the Veterans Health Administration. J Clin Sleep Med 2013;9(12):1253-1258.
Keywords: Sleep apnea, depression, anxiety, veterans
Obstructive sleep apnea (OSA), defined as impaired patency of the upper airway during sleep, resulting in apneas (complete cessation of airflow for at least 10 seconds) and/ or hypopneas (50% reduction in airflow), is one of the most common forms of sleep disordered breathing (SDB). OSA can result in hundreds of brief arousals from sleep in a single night and affects approximately 2% of women and 4% of men nationwide,1 with higher rates documented among military veterans (6.5%).2 Indeed, OSA is one of the most common, yet underdiagnosed, causes of sleep disturbances among veterans, showing no remittance without treatment or lifestyle changes (loss of weight).3 The nearly twofold difference in prevalence of OSA among veterans, compared to community samples, is thought to be due, at least in part, to two risk factors which are common among veterans: male gender and obesity.4
In addition to direct effects (e.g., daytime fatigue, disturbed sleep, irritability, memory problems, and decreased quality of life),5,6 OSA is associated with a number of indirect physical and psychological complications. Such complications include hypertension, heart disease and heart failure, stroke, insulin resistance and impairments in neurocognitive functioning, workplace and driving accidents, and elevated psychological symptoms.7–11 While the associations between OSA and physiological conditions are well established, research is starting to expand our knowledge of the relation between OSA and psychopathology.
BRIEF SUMMARY
Current Knowledge/Study Rationale: Previous work has documented a relation between sleep apnea and psychopathology, however, limited work has examined this among veterans, a sample of individuals at elevated risk for both sleep apnea and psychopathology. The current study examines the relations between sleep apnea and the likelihood of being diagnosed with a psychological condition among veterans throughout the VA Health Care System.
Study Impact: Results indicate a strong association between mood and anxiety disorders and sleep apnea among obese veterans. This highlights the importance of conducting sleep apnea assessments among obese veterans with mood and anxiety disorders (especially MDD and PTSD), as well as conducting anxiety and mood assessments among obese veterans with sleep apnea; such information could aid in the allocation of resources in order to optimize treatments for psychopathology and sleep apnea.
OSA and Mood Disorders
To date the majority of studies investigating the association between OSA and psychopathology have focused on mood disorders, specifically major depressive disorder (MDD). While a few studies have demonstrated a lack of an association between OSA and MDD,12,13 a majority have pointed, instead, to a strong relation between OSA and MDD.14,15 For example, community-based epidemiological work has suggested that individuals with MDD are at a five-fold greater risk for having OSA than healthy controls,16 with between 44.6% and 56% of patients with OSA meeting criteria for MDD.17,18 Providing further support for the relation between OSA and MDD, intervention studies have demonstrated that treatment of OSA (via continuous positive airway pressure [CPAP] or surgery) results in improvements in depressive symptoms.19
OSA and Anxiety Disorders
Relatively less research has investigated the relation between OSA and anxiety disorders. The work that has been done in this area has demonstrated that 16.7% of military veterans with OSA also had an anxiety disorder.20 Though the comorbidity between OSA and anxiety is striking, the majority of work conducted on this association has specifically focused on the relation between OSA and posttraumatic stress disorder (PTSD), and to a lesser extent, panic disorder (PD). Indeed, 12.86% of veterans with OSA have a diagnosis of PTSD20; and OSA has been associated with nocturnal panic attacks and aggravation of panic symptoms.21,22 Intervention research further supports this association. Similar to findings with MDD, the treatment of OSA through the use of CPAP reduces symptoms of PTSD and panic.22–24 Unfortunately, over 50% of veterans with PTSD are non-adherent to CPAP, a significantly lower adherence rate than veterans without PTSD,25 suggesting that PTSD itself may interfere with successful treatment of OSA.
OSA and Substance Use Disorders
A relative dearth of research has investigated the relation between OSA and substance use disorders (SUDs), with generally mixed results among existing empirical investigations. Cross-sectional work has suggested a relation between OSA and SUDs, particularly alcohol use disorders.26 However, epidemiological work among military veterans has found no differences in SUD diagnosis (or alcohol use disorders, specifically) between those with and without OSA.20 While this finding may have been influenced by differential rates of diagnosis across Veterans Affairs (VA) facilities, further research is clearly needed to better understand the relation between OSA and SUDs.
Summary
Taken together, previous work has documented a relation between OSA and psychopathology,27 with the strongest associations being observed for MDD,16–18 anxiety disorders,20 and PTSD, specifically.28 To date, there has been only one study investigating the relation between OSA and psychopathology within the VA Health Care System, which is surprising given the heightened prevalence of OSA among veterans.2,22 This study was a cross-sectional retrospective review of a centralized VA database between the years 1998 and 2001. The sample included 4,060,504 military veterans with and without sleep apnea. ICD-9-CM codes were extracted to identify diagnostic status of sleep apnea and psychological conditions. Results from logistic regressions demonstrated that OSA was associated with increased risk for psychological diagnosis including MDD (21.8%), anxiety (16.7%), PTSD (11.9%), and bipolar disorder (3.3%). Two main extensions to this prior work are needed in order to inform our understanding of the relations between OSA and psychopathology among veterans. First, the study by Sharafkhaneh and colleagues20 did not account for differential diagnosis rates across VA facilities, which may explain the observed associations between OSA and psychological diagnosis. Second, relatively little work has accounted for third factors that may influence the observed associations. For example, it is possible that a common risk factor for both OSA and psychopathology may be driving these relations (e.g., severity of obesity14).
The Role of Severity of Obesity
Obesity is associated with mood, anxiety, and somatoform disorders as well as elevations in psychological distress.29–31 In addition, obesity is one of the leading risk-factors for OSA.32 The relation between obesity and OSA is thought to be due to anatomical modifications that result in either upper airway constriction or reduction in lung volume, leading to a loss of caudal traction of the upper airway and pharyngeal collapse.33 In fact, a one standard deviation increase in body mass index (BMI) has been associated with a 4-fold increase in the prevalence of OSA.34 Indeed, of those with severe obesity (BMI > 40), the prevalence of OSA ranges between 40% and 90%.35 Given these associations, there is clearly a need to account for the severity of obesity when assessing relations between OSA and psychological diagnoses.
Current Study
We sought to replicate and extend the work of Sharafkhaneh20 by examining the association between OSA and the likelihood of being diagnosed with a psychological condition. We aimed to test these associations among obese veterans across all 140 Veterans Health Administration (VHA) facilities, after accounting statistically for the potentially correlated nature of both patients and diagnostic conventions within each facility as well as severity of obesity (i.e., BMI). We examined these relations among obese veterans only, as we wanted to investigate if the pattern of these relations remained consistent with findings from Sharafkhaneh when examining a population at significant risk for both psychological conditions and OSA.32 Based on prior research,20 we hypothesized that individuals with a diagnosis of OSA would be more likely to be diagnosed with (a) mood disorders, and (b) anxiety disorders, but not (c) substance use disorders. In addition, we expected these relations would hold after accounting for severity of obesity (i.e., BMI).
METHODS
The current study is a retrospective cross-sectional database review of all outpatient medical records collected across each of the 140 VHA facilities for fiscal year (FY) 2010 (October 2009-September 2010). Study procedures were approved by the VA Palo Alto Health Care System's research office and Stanford University's Human Research Protection program.
Information Collected
Data Extraction
Data were obtained from the outpatient VHA Decision Support System (DSS) database. The DSS is a national clinical centralized relational database that includes encounter data from VHA clinical information systems. Patient information, including but not limited to, demographics, diagnoses, procedures, and services provided are updated on a daily basis. In order to construct a database appropriate for the current analyses, SAS v9.2 was used to extract demographic variables, body mass index (BMI), obesity-related physical conditions (ICD-9-CM codes), psychological diagnoses (ICD-9-CM codes), and diagnosis of sleep apnea. A unique identifier (scrambled social security number) was used to obtain complete patient records within the DSS.
Selection of Participants
Within the DSS we sought to identify veterans at-risk for sleep apnea as a function of obesity. From the 5,576,858 total VHA outpatients seen in FY2010 across the 140 facilities, 64% (N = 3,574,765) had at least one record entry of height and weight available to calculate BMI. Previous research using this database has indicated that 90% of within-person repeated measures demonstrated < 1-inch differences in height and < 2% had different values for weight.36 Based on this work, we included individuals with ≥ 1 measurement for height and weight in order to optimize our potential sample size. In the case of multiple values per patient, the largest biologically plausible (i.e., height < 84 inches and weight < 700 pounds), value was used to calculate BMI. The largest weight value was chosen because those fluctuating throughout the year in meeting obesity criteria were considered higher risk than those not meeting criteria at any point during the year. Patients were retained in the final sample (n = 2,485,658) if they had a (a) BMI ≥ 30, or (b) 25 ≤ BMI < 30 and at least one obesity associated comorbidity (e.g., diabetes, hypertension, hyperlipidemia, heart disease, congestive heart failure, cholelithiasis, osteo-arthritis, low back pain, gastroesophageal reflux disease, and obstructive sleep apnea).
Measures
Outcome Variables
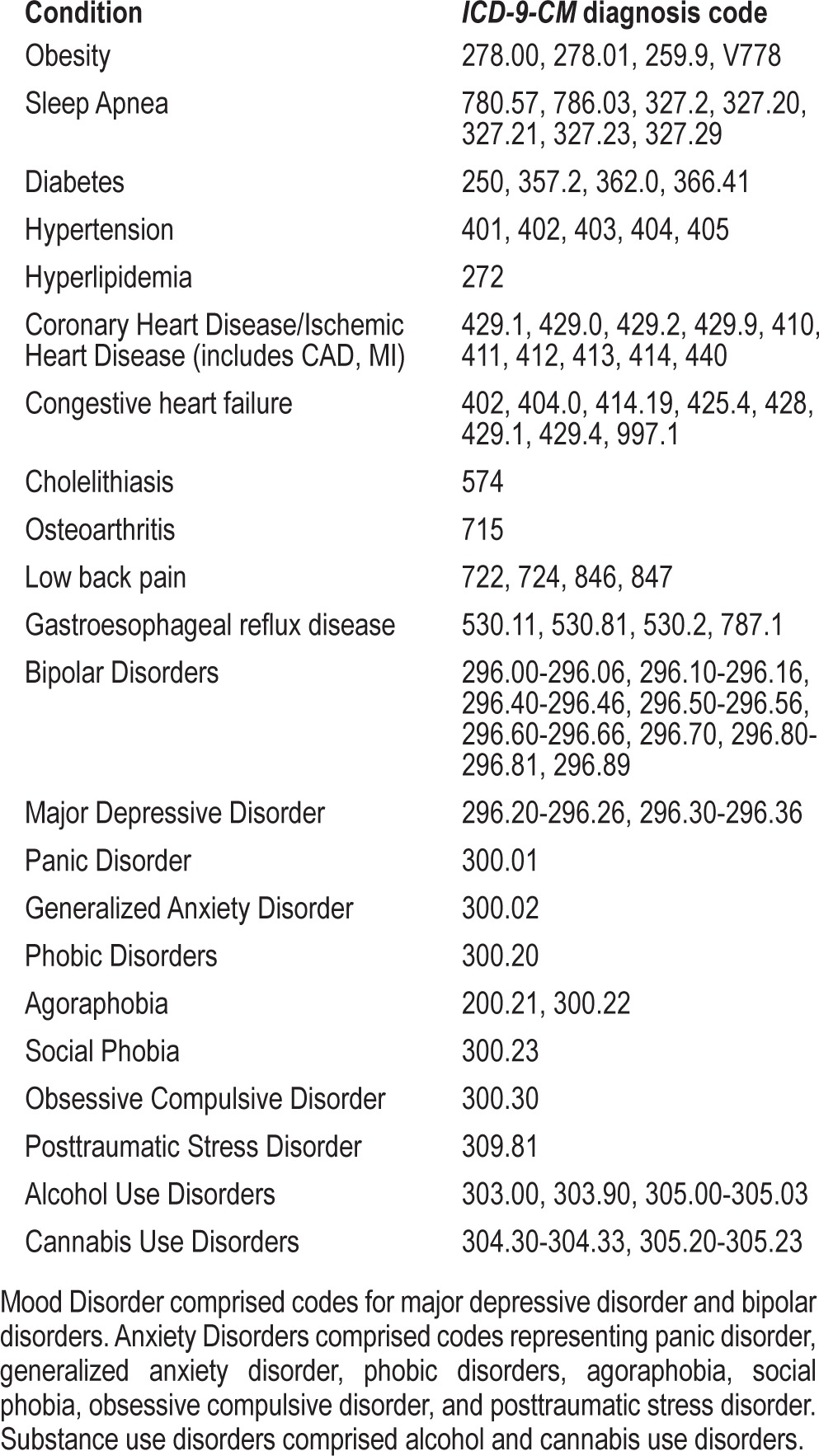
The primary outcomes of this study included psychological diagnostic status. All diagnoses were made by outpatient health care providers and are based on diagnostic criteria consistent with ICD-9-CM diagnoses. Previous work has vetted the accuracy of diagnoses within VA administrative databases.37 First, we investigated psychological diagnostic status across broad classifications including (a) mood disorders, (b) anxiety disorders, and (c) substance use disorders (SUDs; see Table 1 for corresponding ICD-9-CM codes). Second, in the event of a clinically significant finding within a classification, subsidiary analyses were then conducted for each specific disorder (e.g., PTSD, MDD, alcohol use disorder; see Table 1 for corresponding ICD-9-CM codes) comprising that classification. All outcomes were binary (0 = absence of diagnosis, 1 = presence of diagnosis).
Table 1.
ICD-9-CM Diagnostic Codes
Explanatory Variables
To determine patient characteristics associated with psychological diagnostic status, data on patient variables were obtained including: (a) BMI (defined as [703 × weight in pounds]/height in inches squared), (b) obesity-related comorbidities (diabetes: ICD-9-CM 250, 357.2, 362.0, 366.41; hypertension (401-405); 8 additional obesity-related comorbidities summarized in Table 1), and (c) sleep apnea (see Table 1 for details). All variables, with the exception of BMI, were binary (0 = absence, 1 = presence).
Data Analytic Plan
To describe and explore variability in facility-level rates of psychological diagnoses and sleep apnea diagnosis, we calculated the rate of each respective diagnosis (number of patients with the diagnosis divided by the total number of patients in the facility) in each of the 140 VHA facilities. Next, in order to evaluate the relation between sleep apnea, obesity, and psychological diagnoses (anxiety disorder, mood disorder, substance abuse disorder) we conducted three primary analyses using generalized linear mixed effects models. Independent models were generated for each binary dependent variable (i.e., anxiety disorder, mood disorder, substance use disorder). In the event of a clinically significant finding, subsidiary analyses were conducted for each specific disorder comprising the significant category of psychopathology. Within all models, a random effect for facility was included to account for grouping of patients within VHA facilities. PROC GLIMMIX procedures available within SAS V 9.2 were used to perform estimation and statistical inference for generalized linear mixed effects models.
RESULTS
Rates of Diagnosis
In FY2010, PTSD (12.30%) was the most common psychological diagnosis among obese veterans, followed by: MDD (6.40%), SUD (4.19%), bipolar disorder (I and II; 2.63%), generalized anxiety disorder (1.75%), panic disorder (.91%), agoraphobia (.35%), and social anxiety disorder (0.11%). Additionally, 6.68% of obese veterans received a diagnosis of sleep apnea.
Facility-Level Correlates of Psychological Disorder Diagnosis
In relation to facility-level correlates of psychological diagnosis, the intraclass correlation (ICC) of the intercept-only model indicated that 9.4% of the total variance in mood disorder diagnosis was between facilities rather than explainable by patient factors. Similarly, 10.3% of the total variance in anxiety disorder diagnosis and 20.3% of variance in SUD diagnosis were attributable to differences between facilities.
Final Model
Results from the final multi-predictor analyses are provided below. Results are discussed in relation to each diagnostic classification (i.e., mood disorders, anxiety disorders, SUDs). Next, in the case of a clinically significant finding, results are presented for each specific disorder comprising the respective classification of psychopathology.
Mood Disorders
After accounting for the correlated nature of patients within facility, individuals with a diagnosis of sleep apnea were at increased odds of receiving a mood disorder diagnosis (OR = 1.85; CI = 1.80-1.88; p < 0.001). Results remained after accounting for BMI, such that after holding BMI constant, a diagnosis of sleep apnea was associated with increased odds of a mood disorder diagnosis (OR = 1.75; CI = 1.62-1.89; p < 0.001). In comparison, when holding sleep apnea diagnosis constant, BMI was not associated with the odds of having a mood disorder diagnosis (OR = 1.04; CI = 1.03-1.04). Subsidiary analyses indicated that individuals with a sleep apnea diagnosis had a 1.4 times (p < 0.001) greater likelihood of having a diagnosis of MDD, and a 1.01 times (p < 0.001) greater likelihood in having a bipolar disorder diagnosis. Results remained after accounting for BMI such that when holding BMI constant, individuals with sleep apnea had greater odds of having a diagnosis of MDD (OR = 0.59; CI = 0.58-0.60; p < 0.001) and to a lesser extent, bipolar disorder (OR = 0.48; CI = 0.46-0.49; p < 0.001). Consistent with the primary analysis, results were nonsignificant when holding sleep apnea constant.
Anxiety Disorders
After accounting for the correlated nature of patients within facility, individuals with a diagnosis of sleep apnea were at greater odds of receiving an anxiety disorder diagnosis (OR = 1.82; CI = 1.77-1.84; p < 0.001). Results remained after accounting for BMI, such that after holding BMI constant, a diagnosis of sleep apnea was associated with increased odds of an anxiety disorder diagnosis (OR = 1.71; CI = 1.61-1.82). In comparison, when holding sleep apnea diagnosis constant, BMI was not clinically significantly associated with the odds of having an anxiety disorder diagnosis (OR = 1.02; CI = 1.02-1.02). Subsidiary analyses indicated that individuals with a sleep apnea diagnosis had 1.5-fold greater odds of having a PTSD diagnosis, a 1.3-fold increase in odds of a panic disorder diagnosis, and a 1.2-fold increase in having a diagnosis of both generalized anxiety disorder and agoraphobia (all p's < 0.001). Results remained after accounting for BMI. Here, when holding BMI constant, individuals with sleep apnea had the greatest odds of having a diagnosis of PTSD (OR = 0.58; CI = 0.58-0.59; p < 0.001), followed by panic disorder (OR = 0.55; CI = 0.53-0.56; p < 0.001), generalized anxiety disorder (OR = 0.54; CI = 0.53-0.56; p < 0.001), and agoraphobia (OR = 0.54; CI = 0.51-0.57; p < 0.001). Again, consistent with the primary analysis, results were nonsignificant when holding sleep apnea constant.
Substance Use Disorders
After accounting for the correlated nature of patients within facility, individuals with a diagnosis of sleep apnea were not at clinically greater odds of receiving a substance use disorder diagnosis (OR = 0.94; CI = 0.92-0.97). Due to the nonsignificant findings, further analyses were not conducted.
DISCUSSION
Results from this study demonstrate that, among obese veterans in the VA Health Care System, a diagnosis of sleep apnea is associated with increased risk for having a mood or anxiety disorder, but not a substance use disorder. The strongest associations were observed for MDD and PTSD. In addition, results remained after accounting for BMI, such that when holding BMI constant, individuals with sleep apnea had increased odds of both mood and anxiety disorders, specifically MDD, bipolar disorder, PTSD, panic disorder, generalized anxiety disorder, and agoraphobia.
Obese veterans with sleep apnea had clinically significant greater odds of having a mood disorder. This finding is consistent with previous research.20 In addition, when holding BMI constant, a significant relation emerged for mood disorders. This indicates that the association between sleep apnea and mood disorders is attributable, at least in part, to factors other than BMI. While mixed results exist for the relation between sleep apnea and MDD, results from specificity analyses supported previous research,20 indicating an association between sleep apnea and MDD (and to a lesser extent bipolar disorders) as the strongest association within the mood disorders. As results demonstrated that the association was above and beyond BMI, it is unlikely that among this sample BMI was affecting the nature of the relation between sleep apnea and MDD. Two primary theoretical models have been posited to explain this relation. First, some have suggested that the relation between sleep apnea and MDD is explained by depression secondary to a general medication condition.38 Additional work has suggested that hypoxemia, fragmented sleep, and the daytime consequences of poor sleep (fatigue, excessive daytime sleepiness) have been shown to increase depressed mood.39 Unfortunately, the cross-sectional nature of the present investigation does not allow for an understanding of the temporal relations of the observed associations.
Obese veterans with sleep apnea also had clinically significant greater odds of having an anxiety disorder. This finding adds to the literature base supporting an association between sleep apnea and anxiety.20 Further, results remained after accounting for BMI, such that when holding BMI constant, sleep apnea was still associated with anxiety disorders. Consistent with the findings regarding mood disorders, this suggests that the relation between sleep apnea and anxiety is above and beyond the impact of BMI. In terms of specific anxiety disorders, results indicated that sleep apnea had the strongest association with PTSD (followed by panic disorder and generalized anxiety disorder), a consistent finding in the recent literature.20
As expected, we did not observe an association between sleep apnea and substance use disorders. This is consistent with previous research conducted among veterans,20 however, is in contrast to a host of additional work suggesting an association between substance use disorders and sleep apnea.40,41 This finding may be influenced by data collection methods. This is to say, all data were collected from outpatient VA records. It is possible that individuals with severe substance abuse disorders (a) do not seek treatment within the VA, or (b) are more likely to use inpatient and residential services, which were not included here.
While this study has a number of strengths, including the use of a large sample across the VA health care system, and accounting for differential rates of diagnosis across facilities, there are some limitations which should be considered when interpreting these results. First, the data presented here are cross-sectional in nature and therefore causal or temporal conclusions cannot be made, nor can we identify mechanisms that may be involved in the observed associations. However, as findings have replicated those of Sharafkhaneh and colleagues,20 future research would now benefit from determining mechanisms that may further explain the differential relations between sleep apnea and mood/anxiety versus substance use disorders. Second, a number of individuals were excluded due to missing height and/or weight assessments. Future research would benefit from more consistent inclusion of these assessments. Third, all data were obtained from a retrospective database review of ICD-9-CM diagnostic codes. While the reliance on ICD-9-CM diagnostic codes within DSS data introduces the potential for miscoding or misclassification, ICD-9-CM codes have generally been found to be a valid proxy for estimating disorder42 and have been consistently used within VA research.20,43 Future research would benefit from the inclusion of longitudinal work using standardized assessments. For example, inclusion of multi-modal assessment would strengthen confidence in diagnoses, especially in relation to sleep apnea. Here, inclusion of a sleep laboratory assessment to confirm sleep apnea status would be beneficial. This form of assessment would also allow for the determination of history and type of sleep apnea, as well as the patients' involvement in treatment for sleep apnea, which our current data cannot provide. Fourth, as our sample was comprised entirely of obese veterans, we may have a restricted range of BMI, which may have affected the observed findings. Finally, the use of an entirely veteran sample may limit the generalizability of the findings. While our prevalence rates of PTSD are consistent with past VA research20 and VA diagnostic trends,44 observed rates of MDD were significantly lower than among other VA samples.20 These findings should be replicated among other VA, as well as non-veteran and female samples.
Despite these limitations, results provide preliminary clinical implications. Namely, findings indicate a strong association between mood and anxiety disorders and sleep apnea among obese veterans. This highlights the importance of conducting sleep apnea assessments among obese veterans with mood and anxiety disorders (especially MDD and PTSD), as well as conducting anxiety and mood assessments among obese veterans with sleep apnea. Such information could aid in the allocation of resources in order to optimize treatments for psychopathology and sleep apnea.
DISCLOSURE STATEMENT
This was not an industry supported study. This work was supported, in part, by Health Services Research and Development Service funds provided to Drs. Babson and Del Re. The expressed views do not necessarily represent those of the Department of Veterans Affairs. The authors have indicated no financial conflicts of interest.
REFERENCES
- 1.Vgontzas A, Kales A. Sleep and its disorders. Annu Rev Med. 1999;50:387–400. doi: 10.1146/annurev.med.50.1.387. [DOI] [PubMed] [Google Scholar]
- 2.Engdahl B, Eberly R, Hurwitz T, Mahowald M, Blake J. Sleep in a community sample of elderly war veterans with and without posttraumatic stress disorder. Biol Psychiatry. 2000;47:520–5. doi: 10.1016/s0006-3223(99)00201-2. [DOI] [PubMed] [Google Scholar]
- 3.Ballester E, Badia J, Hernandez L, et al. Evidence of the effectiveness of continuous positive airway pressure in the treatment of sleep apnea/hypopnea syndrome. Am J Respir Crit Care Med. 1999;159:495–501. doi: 10.1164/ajrccm.159.2.9804061. [DOI] [PubMed] [Google Scholar]
- 4.Ocasio-Tascon M, Alicea-Colon E, Torres-Palacios A, Rodriguez-Cintron W. The veteran population: one at high risk for sleep-disordered breathing. Sleep Breath. 2006;10:70–5. doi: 10.1007/s11325-005-0043-9. [DOI] [PubMed] [Google Scholar]
- 5.Flemons W, Tsai W. Quality of life consequences of sleep disordered breathing. J Allergy Clin Immunol. 1997;99:S750–60. doi: 10.1016/s0091-6749(97)70123-4. [DOI] [PubMed] [Google Scholar]
- 6.Guilleminault C, Partinen M, Querasalva M, Hayes B, Dement W, Ninomurcia G. Determinants of daytime sleepiness in obstructive sleep apnea. Chest. 1988;94:32–7. doi: 10.1378/chest.94.1.32. [DOI] [PubMed] [Google Scholar]
- 7.Redline S, Strohl K. Recognition and consensus of obstructive sleep apnea hypopnea syndrome. Otolaryngol Clin North Am. 1999;132:303. doi: 10.1016/s0030-6665(05)70132-8. [DOI] [PubMed] [Google Scholar]
- 8.Malone S, Liu P, Holloway R, Rutherford R, Xie A, Bradley T. Obstructive sleep apnoea in patients with dilated cadiomyopathy: effects of continuous positive airway pressure. Lancet. 1991;338:1480–4. doi: 10.1016/0140-6736(91)92299-h. [DOI] [PubMed] [Google Scholar]
- 9.Partinen M, Guilleminault C. Daytime sleepiness and vascular morbidity at seven-year follow-up in obstructive sleep apnea patients. Chest. 1988;94:9–24. doi: 10.1378/chest.97.1.27. [DOI] [PubMed] [Google Scholar]
- 10.Quan S, Howard B, Iber C, et al. The Sleep Heart Health Study: design, rationale, and methods. Sleep. 1997;20:1077–85. [PubMed] [Google Scholar]
- 11.Stepnowsky C, Palau J, Zamora T, Ancoli-Israel S, Loredo J. Fatigue in sleep apnea: The role of depressive symptoms and self-reported sleep quality. Sleep Med. 2011;12:832–7. doi: 10.1016/j.sleep.2011.07.004. [DOI] [PubMed] [Google Scholar]
- 12.Pillar G, Lavie P. Psychiatric symptoms in sleep apnea syndrome: effects of gender and respiratory disturbance index. Chest. 1998;114:697–703. doi: 10.1378/chest.114.3.697. [DOI] [PubMed] [Google Scholar]
- 13.Sforza E, de Sant Hilaire Z, Pelissolo, et al. Personality, anxiety and mood traits in patient with sleep-related breathing disorders: effect of reduced daytime alertness. Sleep Med. 2002;3:139–45. doi: 10.1016/s1389-9457(01)00128-9. [DOI] [PubMed] [Google Scholar]
- 14.Aloia M, Arnedt J, Smith L, et al. Examining the construct of depression in obstructive sleep apnea syndrome. Sleep Med. 2005;6:115–21. doi: 10.1016/j.sleep.2004.09.003. [DOI] [PubMed] [Google Scholar]
- 15.Peppard P, Szklo-Coxe M, Hla K, et al. Longitudinal association of sleep related breathing disorder and depression. Arch Intern Med. 2006;166:1709–15. doi: 10.1001/archinte.166.16.1709. [DOI] [PubMed] [Google Scholar]
- 16.Ohayon M. The effects of breathing-related sleep disorders on mood disturbances in the general population. J Clin Psychiatry. 2003;64:1195–200. doi: 10.4088/jcp.v64n1009. [DOI] [PubMed] [Google Scholar]
- 17.Kales A, Caldwell A, Cadieux R, Vela-Bueno A, Ruch L, Mayes S. Severe obstructive sleep apnea-II: Associated psychopathology and psychosocial consequences. J Chron Dis. 1985;38:427–34. doi: 10.1016/0021-9681(85)90138-9. [DOI] [PubMed] [Google Scholar]
- 18.McCall W, Harding D, O'Donovan C. Correlates of depressive symptoms in patients with obstructive sleep apnea. J Clin Sleep Med. 2006;2:424–6. [PubMed] [Google Scholar]
- 19.Kawahara S, Akashiba T, Akahoshi T, Takasji H. Nasal CPAP improves the quality of life and lessens the depressive symptoms in patients with obstructive sleep apnea syndrome. Intern Med. 2005;44:422–7. doi: 10.2169/internalmedicine.44.422. [DOI] [PubMed] [Google Scholar]
- 20.Sharafkhaneh A, Giray N, Richardson P, Young T, Hirshkowitz M. Association of psychiatric disorders and sleep apnea in a large cohort. Sleep. 2005;23:1405–11. doi: 10.1093/sleep/28.11.1405. [DOI] [PubMed] [Google Scholar]
- 21.Edlund M, McNamara E, Millman R. Sleep apnea and panic attacks. Comp Psychiatry. 32:130–2. doi: 10.1016/0010-440x(91)90004-v. [DOI] [PubMed] [Google Scholar]
- 22.Takaesu Y, Inoue Y, Komadad Y, Kagimura T, Iimori M. Effects of nasal continuous positive airway pressure on panic disorder comorbid with obstructive sleep apnea syndrome. Sleep Med. 2012;13:156–60. doi: 10.1016/j.sleep.2011.10.016. [DOI] [PubMed] [Google Scholar]
- 23.Krakow B, Lowry C, Germain A, et al. A retrospective study on improvements in nightmares and post-traumatic stress disorder following treatment for co-morbid sleep-disordered breathing. J Psychosom Res. 2000;49:291–8. doi: 10.1016/s0022-3999(00)00147-1. [DOI] [PubMed] [Google Scholar]
- 24.Youakim J, Doghramji K, Schutte S. Posttraumatic stress disorder and obstructive sleep apnea syndrome. Psychosomatics. 1998;39:168–71. doi: 10.1016/S0033-3182(98)71365-9. [DOI] [PubMed] [Google Scholar]
- 25.El-Solh A, Ayyar L, Akinnusi M, Sachin R, Akinnusi O. Positive airway pressure adherence in veterans with posttraumatic stress disorder. Sleep. 2010;33:1495–500. doi: 10.1093/sleep/33.11.1495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Cui R, Tanigawa T, Sakurai S, et al. Associations between alcohol consumption and sleep-disordered breathing among Japanese women. Respir Med. 2011;105:796–800. doi: 10.1016/j.rmed.2011.01.003. [DOI] [PubMed] [Google Scholar]
- 27.Sateia M. Update on sleep and psychiatric disorders. Chest. 2009;135:1370–9. doi: 10.1378/chest.08-1834. [DOI] [PubMed] [Google Scholar]
- 28.Maher M, Rego S, Asnis G. Sleep disturbances in patients with posttraumatic stress disorder: Epidemiology, impact and approaches to management. CNS Drugs. 2006;20:567–90. doi: 10.2165/00023210-200620070-00003. [DOI] [PubMed] [Google Scholar]
- 29.Baumeister H, Harter M. Mental disorders in patients with obesity in comparison with healthy probands. Int J Obes. 2007;31:1155–65. doi: 10.1038/sj.ijo.0803556. [DOI] [PubMed] [Google Scholar]
- 30.Onyike C, Crum R, Lee H, Lyketsos C, Eaton W. Is obesity associated with major depression? Results from the third National Health and Nutrition Examination Survey. Am J Epidemiology. 2003;158:1139–47. doi: 10.1093/aje/kwg275. [DOI] [PubMed] [Google Scholar]
- 31.Simon G, Von Korff M, Saunders K, Miglioretti D, et al. Association between obesity and psychiatric disorders in the US adult population. Arch Gen Psychiatry. 2006;63:824–30. doi: 10.1001/archpsyc.63.7.824. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Young T, Skatrud J, Peppard P. Risk factors for obstructive sleep apnea in adults. JAMA. 2004;291:2013–6. doi: 10.1001/jama.291.16.2013. [DOI] [PubMed] [Google Scholar]
- 33.Schwartz A, Patil S, Laffan A, Polotsky V, Schneider H, Smith P. Obesity and obstructive sleep apnea. Pathogenic mechanisms and therapeutic approaches. Proc Am Thorac Soc. 2008;5:185–92. doi: 10.1513/pats.200708-137MG. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Young T, Palta M, Dempsey J, et al. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328:1230–5. doi: 10.1056/NEJM199304293281704. [DOI] [PubMed] [Google Scholar]
- 35.Frey W, Pilcher J. Obstructive sleep-related breathing disorders in patients evaluated for bariatric surgery. Obes Surg. 2003;13:676–83. doi: 10.1381/096089203322509228. [DOI] [PubMed] [Google Scholar]
- 36.Noel P, Copeland L, Perrin R, et al. VHA corporate data warehouse height and weight data: Opportunities and challenges for health services research. J Rehab Res Dev. 2010;47:739–50. doi: 10.1682/jrrd.2009.08.0110. [DOI] [PubMed] [Google Scholar]
- 37.Szeto H, Coleman R, Gholami P, Hoffman B, Goldstein M. Accuracy of computerized outpatient diagnoses in a veterans affairs general medicine clinic. Am J Manag Care. 2002;8:37–43. [PubMed] [Google Scholar]
- 38.American Psychiatric Association. Diagnostic and statistical manual of mental disorders. Washington DC: American Psychiatric Association; 2000. (4th ed, text revision) [Google Scholar]
- 39.Pochat M, Ferber C, Lemoine P. Depressive symptomatology and sleep apnea syndrome. Encephale. 1993;19:601–7. [PubMed] [Google Scholar]
- 40.Aldrich M, Brower K, Hall J. Sleep-disordered breathing in alcoholics. Alcohol Clin Exp Res. 1999;23:134–40. [PubMed] [Google Scholar]
- 41.Brower K. Alcohol's effects on sleep in alcoholics. Alcohol Res Health. 2001;25:110–125. [PMC free article] [PubMed] [Google Scholar]
- 42.Borzecki A, Wong A, Hickey E, Ash A, Berlowitz D. Identifying hypertension-related comorbidities from administrative data: what's the optimal approach? Am J Med Qual. 2004;19:201–6. doi: 10.1177/106286060401900504. [DOI] [PubMed] [Google Scholar]
- 43.Seal K, Bertenthal D, Miner C, Sen S, Marmer C. Bringing the war back home: Mental health disorders among 103,788 US veterans returning from Iraq and Afghanistan seen at Department Of Veterans Affairs facilities. Arch Intern Med. 2007;167:476–82. doi: 10.1001/archinte.167.5.476. [DOI] [PubMed] [Google Scholar]
- 44.Veterans Health Administration Office of Public Health and Environment Hazards. Analysis of VA health care utilization among U.S. Department of Veterans Affairs. 2009.