

Abstract
Objective This case report is designed to illustrate an uncommon presentation of osteoradionecrosis (ORN) of the temporal bone and a treatment method for bloody otorrhea from a pseudoaneurysm of the internal carotid artery (ICA).
Design This is a single patient case report
Setting University of Missouri-Columbia Hospital and Clinics.
Participants The report describes a patient with a history of hypopharyngeal squamous cell carcinoma (SCCA) who was previously treated with chemoradiation therapy and salvage bilateral neck dissections and then presented in a delayed fashion with profuse, episodic bloody otorrhea. Computed tomography (CT) was consistent with ORN of the temporal bone. The patient underwent emergent cerebral angiography. A pseudoaneurysm of the cervicopetrous ICA was confirmed to be the source of the patient's bloody otorrhea. The lesion was treated by endovascular sacrifice of the ICA using the two-catheter coiling technique.
Results The patient had no neurologic sequelae or further bleeding after treatment.
Conclusions Bloody otorrhea is an uncommon presentation of ORN. Sacrifice of the internal carotid can be considered as a treatment when the source is pseudoaneurysmal.
Keywords: osteoradionecrosis, temporal bone, bloody otorrhea, endovascular coiling, radiation
Introduction
Radiation therapy is a mainstay for treatment of head and neck cancers. Radiotherapy of head and neck cancers can include the temporal bone within the field of radiation. Common radiation complications include xerostomia, eustachian tube dysfunction, chronic serous otitis media, otitis media, sinusitis, cranial nerve palsy, and osteoradionecrosis (ORN). The reported incidence of ORN after head and neck radiation is between 10 and 15%.1 ORN of the temporal bone is an uncommon finding. A rare sequelae of ORN of the temporal bone is the development of a pseudoaneurysm of the internal carotid artery (ICA). Most published case reports of postradiation pseudoaneurysms of the ICA within the temporal bone have occurred after radiation for nasopharyngeal carcinoma.2 3 4 5 Patients with a pseudoaneurysm of the petrous ICA may present with symptoms that include hearing loss, tinnitus, and life-threatening hemorrhage.6
Coiling, stenting, and carotid sacrifice have been described as independent and complementary therapies to treat pseudoaneurysms in this area.7 8 9 10 11 12 Stent coiling is also an option outlined in the literature.10 13 Stenting has the drawback of requiring prolonged antiplatelet therapy. Carotid sacrifice has moved from open procedures for ligation to endovascular techniques for occlusion. One such technique is the deployment of coils into the carotid artery.9 14 Forming a coil mass large enough to seat firmly in the desired segment of the carotid artery can be technically challenging. The two-catheter technique has been described in the literature and is one method to overcome such a problem.15 16 17
Case Report
History and Examination
A 63-year-old man with a history of T2N2cM0 squamous cell carcinoma (SCCA) of the right pyriform sinus was treated with chemotherapy, radiation, and subsequent salvage bilateral neck dissections. At his original surgery, the patient was found to have positive level 2 nodes. The patient subsequently underwent radiation treatment. The technique used was parallel opposed right/left lateral 6 MV X-rays to a dose of 60 Gy. Review of the original plan demonstrated that the upper region of the field did, in fact, include the skull base. He was considered cured of his hypopharyngeal SCCA 8 years later when he presented with several weeks of intermittent right-sided bloody otorrhea.
On evaluation in clinic, the patient gave a 2-year history of right otitis externa. He reported that minor bleeding had evolved into intermittent, unpredictable, and forceful expulsion of bright red blood from his right ear over the last several weeks. This phenomenon was witnessed in clinic when the patient was placed in the supine position. Microscopy revealed extensive bony erosion of the anterior portion of the external auditory canal (EAC) with exposure of the temporomandibular joint. The floor of the EAC was partially eroded with areas of spiculated bone. The erosion extended toward the petrous apex with a small area of exposed and palpable ICA covered with clot and granulation tissue. The tympanic membrane was thickened with obscured landmarks. A biopsy from the floor of the EAC was taken to rule out malignancy. Pathologic examination revealed acute inflammation with intraosseous bacterial invasion of the temporal bone consistent with ORN. Computed tomography (CT) of the head and temporal bones also demonstrated findings consistent with ORN and was concerning for an abnormality of the right cervicopetrous ICA (Fig. 1). Positron emission tomography scan was also performed and did not demonstrate evidence of recurrent or metastatic head and neck cancer.
Fig. 1.
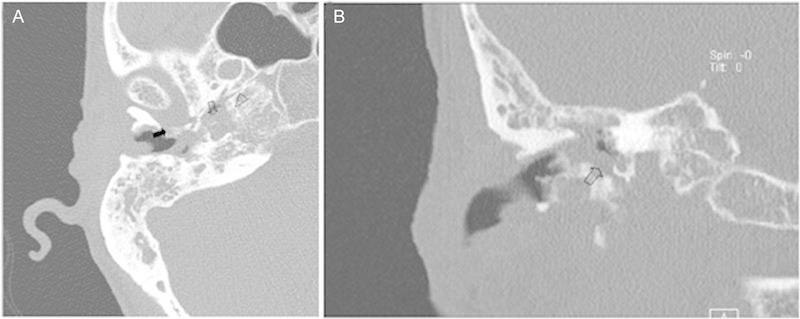
Computed tomography (CT) of the temporal bone showing bony erosion consistent with osteoradionecrosis (ORN) and concerning for a vascular abnormality of the petrous internal carotid artery (ICA). (A) Axial: Solid arrow: eroded posterior wall of temporomandibular joint (TMJ). Clear arrow: pseudoaneurysm. Clear arrowhead: eroded carotid canal. (B) Coronal: Clear arrow: pseudoaneurysm.
The patient was immediately admitted to the hospital and his hemoglobin was 6.4 g/dL. He subsequently underwent diagnostic cerebral angiography that identified a pseudoaneurysm of the right cervicopetrous ICA without active extravasation (Fig. 2A). Given the history of intermittent hemorrhage and the patient's low hemoglobin, he was taken for emergent endovascular treatment.
Fig. 2.
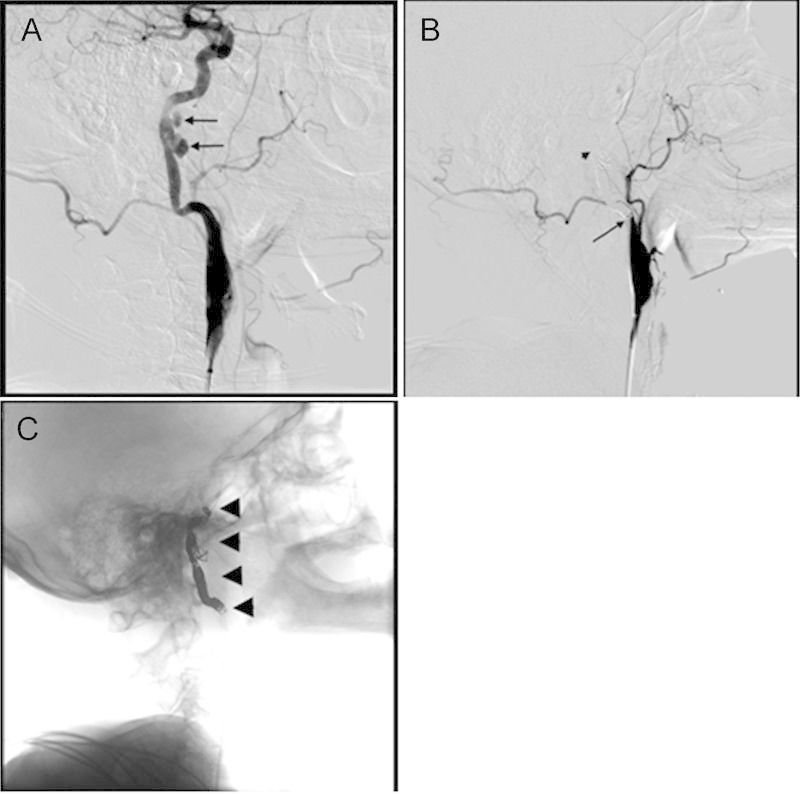
Angiography. (A) Pretreatment image shows a multilobulated pseudoaneurysm (arrows) of the cervicopetrous internal carotid artery (ICA). (B) Posttreatment image showing no filling of the pseudoaneurysm. Long arrow located at the proximal ICA. Short arrow demonstrates the occluded pseudoaneurysm. (C) Posttreatment image showing coil placement (arrowheads) from the petrous ICA to the proximal ICA.
Operation
Given the requirement for emergent management, an endovascular intervention was performed without anesthesia or sedation so that the patient's neurological status could be monitored. A baseline neurologic exam was performed and found to be without deficits prior to the procedure. A 35-minute balloon test occlusion was performed using a 4 mm × 10 mm Hyperform balloon (ev3 Endovascular, Plymouth, Minnesota, USA) advanced over a microwire into the cervical ICA. The patient received a 5,000-unit bolus of heparin prior to balloon inflation. During this time period, the patient's neurologic status was evaluated every 5 minutes and remained deficit-free. A hypotensive challenge was performed and was also tolerated without neurologic deficits. With the balloon inflated, diagnostic angiographic runs performed in the contralateral ICA and vertebral arteries revealed adequate collateral flow. The patient was thus deemed a candidate for right ICA occlusion using detachable coils.
The balloon was deflated and withdrawn. A microcatheter was advanced into the petrous ICA. An attempt was made to deploy a single coil, but it tended to migrate intracranially. Therefore, a second microcatheter was advanced and two coils were deployed simultaneously. This produced enough radial force to seat the coils firmly in the petrous ICA. Additional coils were subsequently deployed from the cavernous ICA to the midcervical ICA, including the deployment of coils within the pseudoaneurysm sac. Throughout the procedure, the patient's neurologic status was monitored and remained stable. Once the occlusion was adequate, a final angiographic run was performed and showed adequate occlusion of the ICA without filling of the pseudoaneurysm (Fig. 2B, Fig. 2C).
Postoperative Course
The patient was observed in the intensive care unit overnight. He received a transfusion of two units of packed red blood cells, which elevated his hemoglobin to 8.7 g/dL. He was progressively mobilized starting 12 hours postembolization and developed no neurologic deficits. He was transferred to the floor on postprocedure day 1 and discharged to home on postprocedure day 2.
Discussion
This case illustrates a potential solution to this unusual presentation of a postradiation pseudoaneurysm of the cervicopetrous ICA. Pseudoaneurysms are described in the literature, but there are many treatment options available. Although stent-assisted treatment may have been an option, this would have required intraprocedural and postprocedural antiplatelet therapy to prevent acute, in-stent thrombosis. Given the patient's active hemorrhage, a therapy requiring antiplatelet medications is not an ideal treatment option. Use of the two-catheter technique does have drawbacks—mainly, increasing the number of catheters in the vessel, which increases both the complexity of the case and the risk related to thrombus formation on not one but two catheters. Overall, however, the two-catheter technique was useful for this case because it eliminated the need for stenting and provided a more controlled deployment of coils within a specific area in the carotid artery that was not possible with a single catheter. The successful use of this technique allowed us to shield the patient from the risks of acute hemorrhage and in-stent thrombosis as well as the long-term risk of in-stent stenosis/thrombosis. Overall, the authors feel that the acute risk of intraprocedural thrombus with a two-catheter treatment is significantly less than the cumulative risk that the patient would have been subjected to in regards to acute hemorrhage and/or in-stent thrombosis/stenosis if he were to have received a stent-assisted treatment.
References
- 1.Hao S P Chen H C Wei F C Chen C Y Yeh A R Su J L Systematic management of osteoradionecrosis in the head and neck Laryngoscope 199910981324–1327., discussion 1327–1328 [DOI] [PubMed] [Google Scholar]
- 2.Auyeung K M, Lui W M, Chow L C, Chan F L. Massive epistaxis related to petrous carotid artery pseudoaneurysm after radiation therapy: emergency treatment with covered stent in two cases. AJNR Am J Neuroradiol. 2003;24(7):1449–1452. [PMC free article] [PubMed] [Google Scholar]
- 3.Lam H C, Abdullah V J, Wormald P J, Van Hasselt C A. Internal carotid artery hemorrhage after irradiation and osteoradionecrosis of the skull base. Otolaryngol Head Neck Surg. 2001;125(5):522–527. doi: 10.1067/mhn.2001.118248. [DOI] [PubMed] [Google Scholar]
- 4.Lau W Y, Chow C K. Radiation-induced petrous internal carotid artery aneurysm. Ann Otol Rhinol Laryngol. 2005;114(12):939–940. doi: 10.1177/000348940511401208. [DOI] [PubMed] [Google Scholar]
- 5.Mak W K, Chow T L, Kwok S P. Radionecrosis of internal carotid artery in nasopharyngeal carcinoma presenting as epistaxis. Aust N Z J Surg. 2000;70(3):237–238. doi: 10.1046/j.1440-1622.2000.01795.x. [DOI] [PubMed] [Google Scholar]
- 6.Luo C B, Teng M M, Chang F C, Chang C Y, Guo W Y. Radiation carotid blowout syndrome in nasopharyngeal carcinoma: angiographic features and endovascular management. Otolaryngol Head Neck Surg. 2008;138(1):86–91. doi: 10.1016/j.otohns.2007.10.013. [DOI] [PubMed] [Google Scholar]
- 7.Alexander M J, Smith T P, Tucci D L. Treatment of an iatrogenic petrous carotid artery pseudoaneurysm with a Symbiot covered stent: technical case report. Neurosurgery. 2002;50(3):658–662. doi: 10.1097/00006123-200203000-00047. [DOI] [PubMed] [Google Scholar]
- 8.Banna M, TerBrugge K, Lasjaunias P, Fournier D. Embolization of dissecting aneurysms of the petrocavernous segment of the carotid artery. Can Assoc Radiol J. 1991;42(4):265–269. [PubMed] [Google Scholar]
- 9.Barr J D, Lemley T J. Endovascular arterial occlusion accomplished using microcoils deployed with and without proximal flow arrest: results in 19 patients. AJNR Am J Neuroradiol. 1999;20(8):1452–1456. [PMC free article] [PubMed] [Google Scholar]
- 10.Bush R L, Lin P H, Dodson T F, Dion J E, Lumsden A B. Endoluminal stent placement and coil embolization for the management of carotid artery pseudoaneurysms. J Endovasc Ther. 2001;8(1):53–61. doi: 10.1177/152660280100800109. [DOI] [PubMed] [Google Scholar]
- 11.Pride G L Jr, Replogle R E, Rappard G, Graybeal C L, White J, Purdy P. Stent-coil treatment of a distal internal carotid artery dissecting pseudoaneurysm on a redundant loop by use of a flexible, dedicated nitinol intracranial stent. AJNR Am J Neuroradiol. 2004;25(2):333–337. [PMC free article] [PubMed] [Google Scholar]
- 12.Saatci I, Cekirge H S, Ozturk M H. et al. Treatment of internal carotid artery aneurysms with a covered stent: experience in 24 patients with mid-term follow-up results. AJNR Am J Neuroradiol. 2004;25(10):1742–1749. [PMC free article] [PubMed] [Google Scholar]
- 13.Mericle R A, Lanzino G, Wakhloo A K, Guterman L R, Hopkins L N. Stenting and secondary coiling of intracranial internal carotid artery aneurysm: technical case report. Neurosurgery. 1998;43(5):1229–1234. doi: 10.1097/00006123-199811000-00130. [DOI] [PubMed] [Google Scholar]
- 14.Braun I F, Hoffman J C Jr, Casarella W J, Davis P C. Use of coils for transcatheter carotid occlusion. AJNR Am J Neuroradiol. 1985;6(6):953–956. [PMC free article] [PubMed] [Google Scholar]
- 15.Horowitz M, Gupta R, Jovin T. The dual catheter technique for coiling of wide-necked cerebral aneurysms. An under-reported method. Interv Neuroradiol. 2005;11(2):155–160. doi: 10.1177/159101990501100206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kwon S C, Shin Y S, Kim H S, Kim S Y. A double catheter technique for elongated middle cerebral artery bifurcation aneurysm. A case report. Interv Neuroradiol. 2006;12(1):41–44. doi: 10.1177/159101990601200108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Shin Y S, Kim D I, Lee S I, Chung J I, Yoon P H, Lee K C. The usefulness of the new “double-catheter technique” in the treatment of parent artery incorporated wide-necked aneurysm with guglielmi detachable coils. Technical notes. Interv Neuroradiol. 2000;6(1):61–64. doi: 10.1177/159101990000600107. [DOI] [PMC free article] [PubMed] [Google Scholar]