

Abstract
Aim
Dental caries is a major public health problem worldwide, with very significant deleterious consequences for many people. The available data are alarming in Canada and the province of Quebec. The water fluoridation program has been shown to be the most effective means of preventing caries and reducing oral health inequalities. This article analyzes the cost-effectiveness of Quebec’s water fluoridation program to provide decision-makers with economic information for assessing its usefulness.
Methods
An approach adapted from economic evaluation was used to: (1) build a logic model for Quebec’s water fluoridation program; (2) determine its implementation cost; and (3) analyze its cost-effectiveness. Documentary analysis was used to build the logic model. Program cost was calculated using data from 13 municipalities that adopted fluoridation between 2002 and 2010 and two that received only infrastructure grants. Other sources were used to collect demographic data and calculate costs for caries treatment including costs associated with travel and lost productivity.
Results
The analyses showed the water fluoridation program was cost-effective even with a conservatively estimated 1 % reduction in dental caries. The benefit-cost ratio indicated that, at an expected average effectiveness of 30 % caries reduction, one dollar invested in the program saved $71.05–$82.83 per Quebec’s inhabitant in dental costs (in 2010) or more than $560 million for the State and taxpayers.
Conclusion
The results showed that the drinking-water fluoridation program produced substantial savings. Public health decision-makers could develop economic arguments to support wide deployment of this population-based intervention whose efficacy and safety have been demonstrated and acknowledged.
Keywords: Water fluoridation, Dental caries, Logic model, Costs, Benefits, Cost-effectiveness
Background and problem
Dental caries is a disease that leads to demineralization and decay of the hard tissues of the tooth through the action of bacterial acids (Levy et al. 2007). In addition to causing suffering, it imposes an economic burden on both individuals and public health services. The population of Quebec, a Canadian province, is particularly affected; children between the ages of 5 and 8 years have up to 40 % more caries than do children in Ontario or the United States, and more than one-third do not meet the dental standards set by the World Health Organization (WHO) in 1979 (MSSS 2006). Quebec children’s poorer dental health is partly due to the fact that the province’s drinking water is much less fluoridated, with only 2.7 % of the population having access to voluntarily fluoridated water in 2010 (as opposed to 7 % in 2006 and 12 % in 1993); that percentage is 70 % in Ontario and 75 % in the United States (INSPQ 2011). This situation is difficult to explain, given that the costs of installing equipment and of the supplies used in fluoridation are fully subsidized by Quebec’s Ministry of Health and Social Services (MSSS).
Water fluoridation consists of adjusting the quantity of fluoride ions already present in drinking water by adding concentrated fluoride. Many studies and systematic literature reviews have demonstrated the beneficial effects of water fluoridation (American Dental Association 2005; Centre for Reviews and Disseminations 2000; McDonagh et al. 2000; MMWR 2001; Ahokas et al. 1999; Truman et al. 2002). A fluoride concentration in water of between 0.7 and 1.5 mg/L protects against dental caries while at the same time minimizing the risk of dental fluorosis (mild whitish spots that generally diminish over time) that can be caused by excessive fluoride (INSPQ 2011; Levy et al. 2007).
At the individual level, by reducing the prevalence of caries, fluoridation helps to improve chewing, enhance overall appearance, reduce tooth loss and use of dental prostheses, and improve health and quality of life, among other things (INSPQ 2011). Studies have also shown that water fluoridation significantly reduces repeat treatments each year over the course of a lifetime among persons already treated for caries. A reduction of 15 to 35 % in root caries has been observed among adults and the elderly living in communities where water is fluoridated (American Dental Association 2005; Centre for Reviews and Disseminations 2000; Griffin et al. 2007; MMWR 2001). In addition, comparisons of communities with and without water fluoridation have shown the former to have lower caries prevalence, ranging from 18 to 40 % for primary and permanent teeth in the general population (MMWR 2001). This reduction in prevalence is quite variable among children 5–12 years old, ranging from 5 to 60 % depending on the sociodemographic and socioeconomic characteristics of the population, with an average of 14.3 % (McDonagh et al. 2000; Ahokas et al. 1999).
In addition to its effects on individuals’ dental health, the fluoridation of drinking water helps reduce social inequalities related to oral health (Levy et al. 2007). The benefits of fluoridation are very significant for people living in disadvantaged environments (Jones et al. 1997; Kumar et al. 1998; McLaren and Emery 2012; Provart and Carmichael 1995; Slade et al. 1996). In effect, since it is tap water that is fluoridated, this intervention reaches the entire population, including the poor, for whom other prevention measures are often not accessible (Akehurst and Sanderson 1994; Levy et al. 2007).
Several opponents of water fluoridation fear it could have harmful effects on the environment, wildlife, and vegetation, and also that it could raise blood levels of lead in children, as well as create other health problems such as bone cancer, etc. However, these fears are not confirmed by current scientific knowledge (Macek et al. 2006; Schock et al. 2006; Osterman 1990; Pollick 2004; Reeves 1986; Tacoma-Pierce County Health Department 2002; Wallis et al. 1996). Thus, fluoridation of drinking water has been shown to be an effective and safe solution not only for improving dental health, but also for reducing oral health inequalities, as recommended by WHO and the Centers for Disease Control (Centre for Reviews and Disseminations 2000).
In this context, the MSSS’s Public Health Directorate has been seeking to develop a solid argument incorporating economic information that could promote fluoridation to decision-makers, especially in the various Quebec municipalities targeted for the water fluoridation program. Demonstrating the cost-effectiveness of fluoridation would provide this solid argument to facilitate and encourage this intervention’s implementation province-wide.
The objective of this study was to analyze the economic value and cost-effectiveness of the fluoridation of drinking water in Quebec. We present here the methodology used and the results obtained; we also discuss the significance and the limitations of the results, as well as possible implications of this research for public health policies in Quebec. This article will be of interest to public health decision-makers, as well as to the community of researchers working in dental health, public health, and economic evaluation.
Methodology
Given that traditional economic evaluation and cost–benefit analysis methods are not well suited to public health interventions, whose effects are spread out over time (Goldsmith et al. 2004), we used an economic evaluation approach that has been adapted and specially conceived for these types of interventions. This innovative approach combines validated methods borrowed from both program evaluation and cost–benefit economic evaluations. It consists of four steps: (1) building a logic model of the intervention; (2) estimating the intervention’s implementation cost; (3) attributing a financial value to the benefits; and (4) evaluating cost-effectiveness in terms of a benefit-cost ratio.
Building a logic model of the water fluoridation program
In the field of program evaluation, building a logic model should be the first step in the evaluative process (Brousselle and Champagne 2011; Funnell and Rogers 2011; Rossi et al. 2004; Weiss 1998). The logic model is a schematic representation of the intervention’s resources, activities, and effects.
Documentary analysis of the scientific literatures (Akehurst and Sanderson 1994; Bertrand et al. 2011; Griffin et al. 2007; Jones et al. 1997; Kumar et al. 1998; McDonagh et al. 2000; Osterman 1990; Pollick 2004; Provart and Carmichael 1995; Quiñonez et al. 2005; Sköld et al. 2008; Slade et al. 1996; Truman et al. 2002; Wallis et al. 1996) and grey literatures (American Dental Association 2005; Brodeur et al. 1998; Brodeur et al. 1999; Brodeur et al. 2001; Centre for Reviews and Disseminations 2000; INSPQ 2011; Levy et al. 2007; Schock et al. 2006; MMWR Fluoride Recommendations Work Group 2001; Ahokas et al. 1999; Reeves 1986; Tacoma-Pierce County Health Department 2002) was used to develop the first version of the logic model. This model was then submitted to three experts in water fluoridation in Quebec for validation. Based on their feedback a new logic model was built, which was subsequently validated by the same experts.
Calculating the cost of the intervention
Data sources
Before presenting in detail the methods used to estimate the costs related to the water fluoridation program, we should point out that most of the data used for this calculation came from the 13 Quebec municipalities that voluntarily fluoridated their water between 2002 and 2010 as well as from two other municipalities that had only received infrastructure subsidies for fluoridation. These data came from MSSS databases. Only 2.7 % of Quebec’s population had access to voluntarily fluoridated water in 2010. Table 1 presents the municipalities that implemented water fluoridation and were subsidized by the MSSS, the years of fluoridation and the years when infrastructure subsidies were received. The demographic data for the population of Quebec as a whole and broken down geographically for each municipality studied were collected from a database at the Institut de la statistique du Québec (ISQ 2011).
Table 1.
Municipalities with water fluoridation programs that were subsidized, with years of fluoridation and of infrastructure subsidies
| Municipalities | Years of fluoridation | Years of infrastructure subsidies |
|---|---|---|
| Bécancour | 2002–2010 | c |
| Côte-de-Beaupréa | b | 2008 |
| Châteauguay | 2002–2010 | 2005 and 2008 |
| Dorval | 2002; 2008–2010 | 2007 |
| Fermont | 2003–2010 | c |
| La Prairie | 2002–2010 | c |
| Lavala | b | 1995 and 1999 |
| Montmagny | 2002–2010 | c |
| Pointe-Claire | 2002–2010 | 2007 |
| Québec | 2002–2007 | c |
| Richmond | 2009–2010 | 2006 |
| Saint-Georges | 2010 | 2009 |
| Saint-Romuald | 2003–2010 | c |
| Trois-Rivières | 2002–2008 | 2010 |
| Verchères | 2005–2010 | 2005 |
aReceived only infrastructure subsidy for fluoridation
bNo fluoridation, Source: MSSS
cNo equipment subsidy
Estimation methods
The cost of the water fluoridation program in Quebec was estimated using the typology developed by the Institut National d’excellence en santé et services sociaux (INESSS) [National institute for health and social services excellence]. This cost was broken down into investment costs, fixed recurrent costs, and variable recurrent costs.
Investment costs
The investment costs are the amounts of the subsidies allocated to nine municipalities for water fluoridation activities (Table 1). Based on MSSS recommendations, we considered that all the infrastructures would be depreciated degressively over 20 years from the date the subsidy was received. The investment costs were assessed in 2010 dollars, adjusted based on: (1) the annual rate of growth in the consumer price index (inflation rate); (2) the discount rate; and (3) the rate of inflation for dental products. Rather than calculate a summary discount rate incorporating all the above rates, which could potentially have introduced biases, we opted instead to estimate the investment costs by varying the discount rate using 3, 5, and 8 %. The 3 and 5 % rates are the discount rates suggested by the federal government of Canada, while 6 and 8 % rates are mentioned by the provincial government of Quebec (Montmarquette and Scott 2007); given the minimal difference between the 6 and 5 % rates, we opted to use the latter. Thus, for each municipality, we calculated the amount of the annual subsidies after degressive depreciation over 20 years. The amount obtained was then adjusted to 2010 dollars for each of the rates retained for this study, i.e., 3, 5 and 8 %.
Finally, we estimated the average cost per inhabitant by municipality (average weighted by the average size of the population of each municipality from 2002 to 2010) and for all of Quebec (average population of Quebec from 2002 to 2010).
Recurrent fixed costs
Recurrent fixed costs are the amounts paid in salaries and fixed contractual costs for the use of the INSPQ public health laboratory for water fluoridation activities. Based on MSSS sources, the following costs were considered:
The salary of a technician in each of the 13 municipalities with fluoridation, at $35/h, 1 h/day, 365 days/year in 2010.
The salary of a full-time MSSS consulting dentist, at $79.10/h, 35 h/week for 44 weeks in 2010.
The salary of a half-time INSPQ consulting dentist, at $79.10/h, 17.5 h/week for 44 weeks in 2010.
The salary of one consulting dentist serving 18 administrative regions of Quebec, at $79.10/h, for one 7-h day per month, 12 times per year, in 2010.
The costs for use of the public health laboratory (INSPQ) under a 2-year contract (2009–2010). These include the costs of monitoring (1) overall system performance, (2) fluoride levels in the networks, and (3) the source of the fluoride ions, as well as general costs and information system costs.
In the first case, the average costs per inhabitant were calculated based on the size of each municipality. In the four other cases, the average costs per inhabitant were calculated by dividing the total annual costs by the total population of Quebec in 2010.
Variable recurrent costs
Variable recurrent costs were measured based on the amounts expended to purchase supplies used to fluoridate water in each of the 13 municipalities that participated in the program for at least 1 year between 2002 and 2010. First, all the amounts were converted to 2010 dollars for each of the rates of 3, 5 and 8 %. Then, the average costs per inhabitant for each municipality were calculated as a weighted average of the annual supply costs in relation to the annual size of the municipalities’ populations from 2002 to 2010. Finally, the total average cost for all of Quebec in 2010 dollars was calculated by adding together all the costs for each municipality.
Estimate of the benefits associated with the water fluoridation program
Estimation methods
The estimated benefits were in fact the savings resulting from the reduction in the number of dental services related to caries, including travel costs and productivity. Dental services included all costs related to the treatments and repeat treatments expected to be required because of caries over the course of a lifetime.
Data sources
The data compiled to estimate the benefits of the Quebec’s water fluoridation program were drawn mainly from the reports of three studies carried out in Quebec by Brodeur and colleagues on the oral health of children 5–8 years old, of children 11–14 years old, and of adults 35–44 years old (Brodeur et al. 2001, 1999, 1998). These are the most recent studies done in Quebec in terms of oral health epidemiology. The prevalence data on caries were taken from the dmft and DMFT indices in those reports and compiled by age; dmft and DMFT indices express the number of primary or permanent teeth decayed (d or D), missing (m or M) or filled (f or F) in children and adults, respectively. The data on percentage of dental services utilization within the past year by age (percentage of the population having consulted) were also extracted from these reports. The demographic data for population estimates by age in Quebec were compiled from a Statistics Canada database (Statistics Canada 2011). Table 2 summarizes, by age groups, the data collected to estimate the benefits associated with water fluoridation in Quebec.
Table 2.
Prevalence of caries, percentage of dental services utilization, and demographic data collected by age
| Age (years) | Study years | Types of teeth | Population with at least one cavity (%) | Index of the average number of decayed, missing or filled teeth (dmft or DMFT) (A) | Percentage of dental services utilization within the past year (B) | Total population in Quebec in 2010 (C) | Estimated population consulting for a cavity during the past year D = (B x C) | Number of teeth restored E = (A x D) |
|---|---|---|---|---|---|---|---|---|
| 5 | 1998 | Primary | 38.9 | 1.77 | 85.6 | 77,644 | 66,463.30 | 117,640.04 |
| 6 | 1998 | Primary | 46.4 | 2.24 | 85.3 | 77,540 | 66,141.60 | 148,157.18 |
| 7 | 1998 | Primary | 52.8 | 2.42 | 90.7 | 76,493 | 69,379.20 | 167,897.66 |
| 8 | 1998 | Primary | 58.2 | 2.83 | 90.8 | 77,436 | 70,311.90 | 198,982.68 |
| Total 5–8 years | 309,113 | 272,295.90 | 632,677.57 | |||||
| 11 | 1996 | Permanent | 53.6 | 1.55 | 86.3 | 79,373 | 68,498.90 | 106,173.30 |
| 12 | 1996 | Permanent | 63.8 | 2.15 | 81.9 | 82,127 | 67,262.00 | 144,613.30 |
| 13 | 1996 | Permanent | 71.8 | 2.59 | 81.8 | 87,047 | 71,204.40 | 184,419.40 |
| 14 | 1996 | Permanent | 74.6 | 3.21 | 78.4 | 91,134 | 71,449.10 | 229,351.61 |
| Total 11–14 years | 339,681 | 278,414.40 | 664,557.60 | |||||
| Total 35–44 years | 1994 | Permanent | 96 | 20 | 69 | 1,049,556 | 724,193.60 | 14,483,872.00 |
| Total Quebec | 7,905,679 |
Costs of treatment for dental caries
Treatment of a tooth that is decayed, missing or filled due to dental caries requires a complete examination, the filling of a dental surface with an amalgam or composite material, and at least one round trip to the treatment centre (hospital or dental clinic). The costs associated with treatment were calculated taking into account all expenses related to each of these items by age group and accordance to the fees then in effect as set by the Régie d’Assurance Maladie du Québec (RAMQ) [Quebec Health Insurance Board] and the Association des chirurgiens-dentistes du Québec (ACDQ) [Quebec Association of Dental Surgeons]. Table 3 summarizes all the activities, their volumes, and the unit costs used to calculate expenses in each of the options for treatment of caries, by type of tooth and age group.
Table 3.
Fees for treatment of one cavity by type of tooth and age group
| Option | Description | Quantification | Assigned value | Source |
|---|---|---|---|---|
| Primary teeth (children 8 years of age and under) | Complete examination | 1 | $41.25 | RAMQ (2006) |
| Filling on 2 surfaces, amalgam, primary tooth | 1 | $70.25 | RAMQ (2006 | |
| Loss of productivity | 85.3 min | $9.65/h | Commission des normes du travail (2011) | |
| Transportation | 32.16 km | $1.059/L | Régie de l’énergie du Québec (2010) | |
| 9.04 L/100 km | ||||
| Permanent teeth (children 14 years of age and under) | Complete examination | 1 | $54.63 | ACDQ (2011) |
| RAMQ (2006) | ||||
| ACDQ (2011) | ||||
| Filling on 2 surfaces, amalgam/composite, permanent tooth | 0.963 | $107.25 | RAMQ (2006) | |
| Loss of productivity | 85.3 min | $9.65/h | Commission des normes du travail (2011) | |
| Transportation | 32.16 km | $1.059/L | Régie de l’énergie du Québec (2010) | |
| 9.04 L/100 km | ||||
| Permanent teeth (adults over the age of 14 years) | Complete examination | 1 | $90 | ACDQ (2011) |
| Filling on 2 surfaces, amalgam/composite, permanent tooth | 6 | $132.50 | ACDQ (2011) | |
| Loss of productivity | 170.6 min | $9.65/h | Commission des normes du travail (2011) | |
| Transportation | 64.32 km | $1.059/L | Régie de l’énergie du Québec (2010) | |
| 9.04 L/100 km |
Cost associated with a complete examination
The cost of a complete examination varies according to the type of tooth (primary or permanent) and the patient’s age. For patients aged 9 years and under, a complete examination for a primary tooth was $41.25 in 2006 according to the RAMQ schedule (RAMQ 2006). This rate is still in effect today. For permanent teeth in children aged 14 years and under, the cost was estimated at $54.63 in 2011 by the ACDQ (ACDQ 2011). Finally, for children aged 15 years and older, as well as for adults, this cost was $90 in 2011, again according to the ACDQ.
Cost related to filling a molar with an amalgam or composite material
For temporary teeth in children aged 9 years and under, the cost of an amalgam filling on two surfaces for a primary molar was $70.25 according to the RAMQ schedule, including the cost of asepsis ($5.50). For permanent teeth in children aged 14 years and under, the cost of an amalgam or composite filling of two surfaces for a permanent molar was $107.25. This cost was obtained by averaging the ACDQ (2011) costs of restoring two surfaces in amalgam ($113) or composite ($152) and the RAMQ (2006) cost of restoring two surfaces in amalgam ($82, including asepsis), giving a total of $107.25, since some of the fillings were done in children below the age of 10 years and others in children age 10 years and over. For children over 14 years old, the price of a filling on two surfaces for a molar (averaging amalgam and composite) was $132.50 (ACDQ 2011).
Cost of travel for a filling
In travel costs, we included both the costs of transportation to the dental services centre and the costs related to loss of productivity due to caries. Loss of productivity: In Quebec, a filling is associated with a single complete examination. The estimated number of minutes for the examination and a return visit to fill a molar, including the wait times in the office for these two visits, was based on the results of a study conducted among Quebec dentists (Bertrand et al. 2011), which obtained an average of 85.3 min for an examination and filling. This time was doubled for patients over the age of 14 years, given that two visits are required. For a conservative estimate, we used the minimum wage rate of $9.65/h to assess costs related to time spent in dental visits for examinations and restorations, both for adult patients and parents of children (Commission des normes du travail 2011). Costs of transportation: The same survey was used to determine the distance travelled by patients to get to a dental clinic. That survey calculated an average one-way distance of 8.04 km, which we multiplied by two for patients under 14 years of age, and by four for patients 14 years and older, given that the examination and filling required two round trips for that age group. Otherwise, average fuel consumption for vehicles in Quebec in 2007 was 9.04 L per 100 km (DesRosiers Automotive Consultants 2008), and the average price of a litre of regular gasoline in Quebec in 2010 was $1.059 (Régie de l’énergie du Québec 2010). Finally, multiplying the average price of fuel by the number of kilometres travelled and the average fuel consumption of vehicles in Quebec, we obtained an average cost of transportation of $2.90 for patients under 14 years of age and $5.80 for patients 14 years and older. These costs were similar to the average public transportation fare in Quebec ($2.75 per ride) in 2010 (Government of Québec 2010). Hence, given the minimal difference in the one-way cost of transportation whether patients used a car or not, we assumed all patients travelled by car.
Average cost of treatment per inhabitant for a decayed, missing or filled tooth, by age
Finally, the average cost of treatment per inhabitant for decayed, missing or filled teeth in Quebec was estimated as follows. First, the total number of teeth restorations was estimated by multiplying the dmft or DMFT index value by the population examined who had used dental services in 2010, in each age group. Then, the total estimated cost for the treatment of decayed, missing or filled teeth was obtained by multiplying the total number of these teeth by the average cost per visit for treatment of a tooth, expressed in 2010 dollars. None of the fees were discounted because they had remained unchanged since that time. Finally, the average cost of treatment per inhabitant in Quebec in 2010 was calculated by dividing the total estimated cost by the total population in 2010.
Costs of repeat treatment of dental caries
The costs of repeat treatment by age group and for all of Quebec were estimated based on the assumption that every year 6.87 % of patients treated for dental caries undergo repeat treatment, up to the age of 81 years (Bertrand et al. 2011; Quiñonez et al. 2005; Sköld et al. 2008). Repeat treatments for primary teeth were considered to occur up to the age of 12 years. All costs were discounted using rates of 3, 5, and 8 %/year.
Benefits of the water fluoridation program due to reduction in dental caries prevalence
Financial benefits and losses were estimated by calculating the difference in dental care costs with and without the intervention. When this difference is positive, we refer to the result as a benefit. In other words, if the water fluoridation program leads to a reduction in dental caries, and thereby to a lowering of costs for dental care related to treatments and repeat treatments for dental caries, then economic benefits will be observed. Given a reduction of X% of prevalence in caries due to a water fluoridation program, the benefit is calculated as follows: Benefit = (1–X %) × total cost of dental care for treatment and repeat treatment. Since the results in the literature have been divergent, with demonstrated effectiveness of the water fluoridation program ranging from 1 to 50 % when comparing fluoridated and non-fluoridated regions, we carried out a sensitivity analysis to estimate the benefits by varying X % between 1 and 50 %.
Cost-effectiveness evaluation
The cost-effectiveness of the water fluoridation program was evaluated by comparing the benefits of the intervention to its costs. We included all the costs of the intervention; for the benefits, we retained only those indirect effects for which monetary values had already been set in the healthcare market. Indeed, it is not always necessary for the economic value of all effects to be calculated in order to reach a cost-effectiveness threshold.
The benefit-cost (B/C) ratio was calculated by age group and for all of Quebec. The B/C ratio provides information on the savings achieved for each dollar invested in the program in Quebec in 2010. The program is considered to be cost-effective if the B/C ratio is above 1. This ratio was calculated by varying the percentage X of reduction in caries attributable to water fluoridation between 1 and 50 %. These percentages represent the levels of effectiveness reported in the literature when comparing reductions in dental caries between regions with and without fluoridation. Univariate and bivariate sensitivity analyses were also carried out, simultaneously varying the discount rate (3, 5, and 8 %) and the percentage of reduction in dental caries (X %). This produced a cost-effectiveness threshold.
Results
Result 1
Logic model for the intervention – water fluoridation program
Figure 1 presents the logic model for Quebec’s water fluoridation program. This model clearly describes the intervention by presenting all of its resources, activities, and effects. In the grey boxes are the items that were included in calculating the intervention’s cost-effectiveness.
Fig. 1.
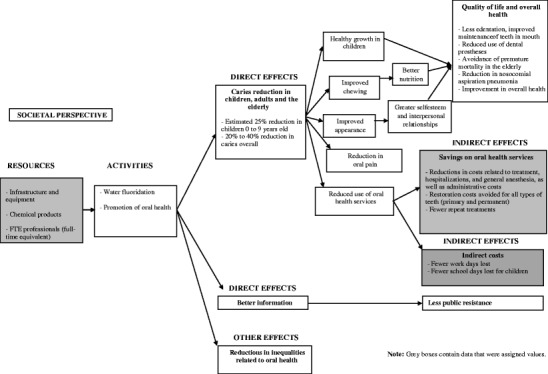
Logic model of Quebec’s water fluoridation program
Result 2
Cost of the water fluoridation program
The analyses showed the total average cost per inhabitant (total population of 7,907,375 in 2010) of the water fluoridation program in Quebec to be $1.93, $2.05, and $2.25 (in 2010 dollars), based on discount rates of 3, 5, and 8 %, respectively.
Result 3
Benefits of the water fluoridation program
Before explaining the benefits of the water fluoridation program, it is important to mention the amount spent on dental care (treatments and repeat treatments) in the absence of any water fluoridation program. The analyses showed these expenses to be either $532.08, $532.87, or $534.05 per inhabitant per year (2010), based on variations in inflation and discount rates of 3, 5, and 8 %, respectively.
Assuming the water fluoridation program reduces the prevalence of caries by X percent, ranging from 1 to 50 %, the benefits achieved for all of Quebec are presented in Table 4, based on discount rates of 3, 5, and 8 %. As an example, if the water fluoridation program reduces dental caries by 30 % on average, as estimated by the MSSS, this would represent savings of more than $159 per inhabitant in 2010 in Quebec.
Table 4.
Savings per inhabitant (2010) by percentage of caries reduction due to the water fluoridation program and by discount rate
| Discount rates | ||||
|---|---|---|---|---|
| 3 % | 5 % | 8 % | ||
| Percentage of caries reduction due to the water fluoridation program | 1 % | $5.32 | $5.33 | $5.34 |
| 15 % | $79.81 | $79.93 | $80.11 | |
| 20 % | $106.42 | $106.57 | $106.81 | |
| 25 % | $133.02 | $133.22 | $133.51 | |
| 30 % | $159.62 | $159.86 | $160.22 | |
| 35 % | $186.23 | $186.50 | $186.92 | |
| 40 % | $212.83 | $213.15 | $213.62 | |
| 50 % | $266.04 | $266.43 | $267.03 | |
Result 4
Cost-effectiveness of the water fluoridation program
Table 5 and Fig. 2 present the detailed results, based on the discount rates applied (3, 5, and 8 %) and reductions in dental caries attributed to the water fluoridation program ranging from 1 to 50 %. Sensitivity analyses showed that, if the water fluoridation program reduced dental caries by 1 %, one dollar invested in the fluoridation program would save $7.32 to $8.53 in dental care costs per inhabitant in 2010 (savings in costs for treatment and repeat treatments). Assuming the MSSS forecasts, which anticipate a 30 % reduction in dental caries due to water fluoridation, are achieved, each dollar invested in fluoridation would avoid a minimum of $71 to $83 (2010) per inhabitant, for total savings of more than $560 million for the State and the population.
Table 5.
Benefit-cost ratios by percentage of caries reduction and discount rate
| Discount rates | ||||
|---|---|---|---|---|
| 3 % | 5 % | 8 % | ||
| Percentage of caries reduction due to the water fluoridation program | 1 % | 8.53 | 8.03 | 7.32 |
| 15 % | 44.4 | 41.8 | 38.08 | |
| 20 % | 57.21 | 53.86 | 49.07 | |
| 25 % | 70.02 | 65.92 | 60.06 | |
| 30 % | 82.83 | 77.98 | 71.05 | |
| 35 % | 95.64 | 90.04 | 82.04 | |
| 40 % | 108.45 | 102.1 | 93.03 | |
| 50 % | 134.07 | 126.22 | 115.00 | |
Fig. 2.
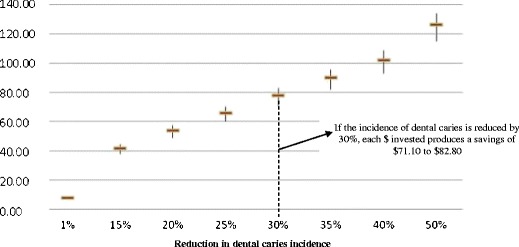
Benefit-cost ratio (B/C)
Our study showed that the water fluoridation program is cost-effective, and that this would be true even for a very conservative estimate of only a 1 % reduction in dental caries. These results were confirmed regardless of the inflation rates and discount rates used. Our results showed that this program would produce substantial savings if implemented in different municipalities across the province. This study, with its economic data, adds to the already well-documented conclusions on the effectiveness of the intervention both at the individual level, in reducing dental caries, and at the societal level, in reducing health-related social inequalities.
Discussion
Even though our methodological approach is quite different from those used in studies on this subject reported in the literature since the 1960s in contexts other than those of Canada and Quebec (Birch 1990; Davies 1973, 1974; Dowell 1976; Griffin et al. 2001; Hardwick 1965; Jackson 1987; Sanderson 1998; Sanderson and Wilson 1994; MMRW Fluoride Recommendations Work Group 2001), our results go in the same direction.
The cost of Quebec’s water fluoridation program ranges from $1.93 to $2.25 (in 2010) per person (total population of almost 8 million). This cost appears high in comparison with that obtained by Ringelberg and colleagues (1992) in their study of 44 communities in Florida, in the US. However, the cost of water fluoridation there varied with community size. The average cost of fluoridation was $2.12 per person in communities with 10,000 inhabitants, whereas in communities of between 10,000 and 50,000 it was only $0.68, and in communities of more than 50,000 inhabitants it was even lower, at $0.31. There are three possible key explanations for the higher costs in Quebec. The first is that all the municipalities with water fluoridation in 2010 had fewer than 50,000 inhabitants. The more populous municipalities, Quebec City and Trois-Rivières, stopped their programs in 2007 and 2008, respectively. The second possible explanation is that the salaries of municipal employees involved in sanitation activities may have been overstated, since water fluoridation activities are blended into their overall daily tasks. It was therefore difficult to isolate the actual time spent by these employees on the fluoridation of drinking water in their municipalities. The third possible explanation relates to the time devoted by the half-time INSPQ consulting dentist to water fluoridation activities in Quebec, which may be overstated. Even though the protocols call for an INSPQ consulting dentist to be involved in these activities, we were informed by various experts that this dentist devotes less time than envisioned to the drinking water fluoridation program.
Finally, we deliberately decided to overestimate program costs whenever there was uncertainty, since our approach was aimed at testing the cost-effectiveness of the water fluoridation program and not at calculating all of its benefits. Only the economic benefits related to savings in treatments and repeat treatments were taken into account. The total savings would have been much greater if our calculations had included the costs of anaesthesia and hospitalizations associated with the treatment of dental caries complications, potential savings related to improved quality of life and overall health, and economic benefits due to reduced oral health inequalities, among others.
However, one limitation should be noted. This study used dental caries prevalence data that were more than a decade old (Brodeur et al. 2001; Brodeur et al. 1999; Brodeur et al. 1998). However, no population-based epidemiological study on dental caries has been carried out since then in Quebec. From the data in the Canadian Health Measures Survey (CHMS) done by Health Canada in 2010, the percentage of the Canadian population with at least one dental cavity has remained stable at 96 % for more than 20 years. We can reasonably assume that the prevalence of caries, in terms of the number of primary or permanent decayed, missing or filled (dmft or DMFT) teeth has remained stable or even increased. Even if the number of dmft or DMFT had decreased over time, the sensitivity analyses (Fig. 2) cover a broad spectrum of potential variation in dental caries in Quebec, thereby strengthening the robustness of the results.
Conclusion
We live in a society where, increasingly, economic data are used to justify the implementation of new interventions or to confirm their validity. This is the case, for instance, for the global health technology assessment movement. While not subject to the same evaluation processes as new drugs and technologies, public health is also under pressure to defend the economic value of its interventions. Therefore, demonstrating the cost-effectiveness of public health interventions would constitute a solid argument for greater investment in this sector.
Public health interventions are not generally good candidates for traditional economic evaluation methods because of the nature of their effects, which are often spread out over the long term and have indistinct boundaries, since they involve many different sectors of activity (education, health, employment, etc.). The approach used here was designed to describe accurately the spectrum of impacts of public health interventions while at the same time offering relevant information for decision-making on resource allocation in the health-care system. The nature of the information provided by this type of analysis is different from what would be offered by traditional analyses: cost-effectiveness analysis would have compared different interventions aimed at improving dental health (e.g. milk fluoridation vs. water fluoridation); traditional cost–benefit analysis would have converted into monetary the direct health effects (e.g. attempting to assign a value to a healthy tooth). We worked with indirect effects related to treatment costs avoided rather than with direct effects related to tooth health, as the former already had an established monetary value in the healthcare market. In this way, we were able to circumvent the ethical and methodological pitfalls of traditional cost–benefit analyses.
The results delivered here on the cost-effectiveness of the drinking water fluoridation program provide directly relevant information to promote an intervention whose efficacy and safety have already been scientifically demonstrated, but which has not been implemented on a large scale in Quebec. This information constitutes a new argument that can be brought into the political arena of budget allocations. One question to which our analysis does not respond, however, is that of ‘who pays and who receives’. In our analysis, we adopted a societal perspective that allowed us to track all the costs and effects of the intervention. However, if the government should decide to proceed, it would probably need to undertake new negotiations among (1) the economic beneficiaries of the intervention, that is, those who would pay less for dental treatment (individuals paying directly, private insurers, the RAMQ), (2) those receiving less as a result of the intervention (dentists and dental health professionals), and (3) those who would fund the intervention (Ministry of Health, municipalities, and taxpayers). It is well known that one person’s income is another person’s expense, and as such, introducing this intervention, even if it is cost-effective, will have redistributive effects. This will likely be the next challenge facing proponents of this program. However, it might also be the redistributive effect of this relatively coercive public health measure that would trigger the decision to proceed with its large-scale deployment: water fluoridation, in contributing to everyone’s oral health, has a major impact on reducing the social inequalities of health, an objective much sought-after but often difficult to achieve through public health policies.
Acknowledgements
We would like to thank the Ministry of Health and Social Services (MSSS) of Quebec, which funded this project, as well as the Canadian Institutes of Health Research (CIHR) and the Fonds de recherche du Québec – Santé (FRQS) which fund the Canada Research Chair in Evaluation and Health System Improvement held by Astrid Brousselle and also funded the postdoctoral fellowships of Éric Tchouaket (4P Training Program: Prevention, Promotion and Public Policy, and PHIRNET: Population Health Intervention Research Network) and Alvine Fansi.
We also extend our thanks to the following experts for their counsel and generous collaboration and contributions: Ginette Lafontaine, Public Health Directorate for the Montérégie Region; Annie-Claude Voisine, MSSS; Caroline De Pokomandy-Morin, MSSS; Bernard Laporte, MSSS; and Lucie Desgagné, MSSS.
Conflict of interest
The authors declare that they have no conflict of interest.
References
- ACDQ . Guide des tarifs et nomenclature des actes buccodentaires au premier janvier 2011. Montreal: Association des Chirurgiens Dentistes du Québec; 2011. [Google Scholar]
- Ahokas J, Demos L, Donohue DC, Killalea S, McNeil J, Rix CJ (1999) Review of water fluoridation and fluoride intake from discretionary fluoride supplements: Review for NHMRC. Royal Melbourne Institute of Technology, Department of Applied Chemistry, Key Centre for Applied Nutritional Toxicology, Monash University, Department of Epidemiology and Preventive Medicine, Melbourne, Australia. Available at: http://www.ada.org.au/app_cmslib/media/lib/0703/m50958_v1_nhmrc%20fluoride.pdf. Accessed 14 May 2012
- Akehurst RL, Sanderson DJ. Cost-effectiveness in dental health: a review of strategies available for preventing caries. J Med Econ. 1994;7:43–54. [Google Scholar]
- American Dental Association (2005) Fluoridation facts. American Dental Association, Chicago. Available at http://www.ada.org/sections/professionalResources/pdfs/fluoridation_facts.pdf. Accessed 14 May 2012
- Bertrand E, Mallis M, Bui NM, Reinharz D. Cost-effectiveness simulation of a universal publicly funded sealants application program. J Public Health Dent. 2011;71(1):38–45. doi: 10.1111/j.1752-7325.2010.00200.x. [DOI] [PubMed] [Google Scholar]
- Birch S. The relative cost effectiveness of water fluoridation across communities: analysis of variations according to underlying caries levels. Community Dent Health. 1990;7:3–10. [PubMed] [Google Scholar]
- Brodeur JM, Payette M, Olivier M, Chabot D, Benigeri M, Williamson S (1998) Étude 1994–1995 sur la santé buccodentaire des adultes québécois de 35 à 44 ans. Government of Québec, Ministry of Health and Social Services, Québec. Available at http://publications.msss.gouv.qc.ca/acrobat/f/documentation/1998/98-268.pdf. Accessed 14 May 2012
- Brodeur JM, Olivier M, Payette M, Benigeri M, Williamson S, Bedos C (1999) Étude 1996–1997 sur la santé buccodentaire des élèves québécois de 11–12 ans et de 13–14 ans. Government of Québec, Ministry of Health and Social Services, Québec. Available at http://publications.msss.gouv.qc.ca/acrobat/f/documentation/1999/99-235.pdf. Accessed 14 May 2012
- Brodeur JM, Olivier M, Benigeri M, Bedos C, Williamson S (2001) Étude 1998–1999 sur la santé buccodentaire des élèves québécois de 5–6 ans et de 7–8 ans. Government of Québec, Ministry of Health and Social Services, Québec. Available at http://publications.msss.gouv.qc.ca/acrobat/f/documentation/2001/01-222-01.pdf. Accessed 14 May 2012
- Brousselle A, Champagne F. Program theory evaluation: logic analysis. Eval Program Plan. 2011;34:69–78. doi: 10.1016/j.evalprogplan.2010.04.001. [DOI] [PubMed] [Google Scholar]
- Centre for Reviews and Disseminations (2000) Fluoridation of drinking water: a systematic review of its efficacy and safety. University of York, UK. Available at: http://www.york.ac.uk/inst/crd/fluores.htm. Accessed 14 May 2012
- Commission des normes du travail (2011) Salaire, paie et travail : taux du salaire minimum. Government of Québec, Québec. Available at http://www.cnt.gouv.qc.ca/salaire-paie-et-travail/salaire/. Accessed 14 August 2012
- Davies GN. Fluoride in the prevention of dental caries: a tentative cost-benefit analysis. Br Dent J. 1973;135:131–134. doi: 10.1038/sj.bdj.4803053. [DOI] [PubMed] [Google Scholar]
- Davies GN. Cost and benefit of fluoride in the prevention of dental caries. Brisbane, Australia: Queensland University; 1974. [Google Scholar]
- DesRosiers Automotive Consultants . 2008 Canadian used vehicle report. Richmond Hill, ON: DesRosiers Automotive Consultants; 2008. [Google Scholar]
- Dowell TB. The economics of fluoridation. Br Dent J. 1976;140:103–106. doi: 10.1038/sj.bdj.4803707. [DOI] [PubMed] [Google Scholar]
- Funnell SC, Rogers PJ. Purposeful program theory: effective use of theories of change and logic models. Indianapolis, IN: Jossey Bass; 2011. [Google Scholar]
- Goldsmith LJ, Hutchison B, Hurley J. Economic evaluation across the four faces of prevention: a Canadian perspective. Hamilton, ON: McMaster University, Centre for Health Economics and Policy Analysis; 2004. [Google Scholar]
- Government of Québec (2010) http://www.gouv.qc.ca/portail/quebec/international/general/quebec/informations/transports/commun/. Accessed 18 September 2012
- Griffin SO, Jones K, Tomar SL. An economic evaluation of community water fluoridation. J Public Health Dent. 2001;61(2):78–86. doi: 10.1111/j.1752-7325.2001.tb03370.x. [DOI] [PubMed] [Google Scholar]
- Griffin SO, Regnier E, Griffin PM, Huntley V. Effectiveness of fluoride in preventing caries in adults. J Dent Res. 2007;86(5):410–415. doi: 10.1177/154405910708600504. [DOI] [PubMed] [Google Scholar]
- Hardwick JL. The value of fluoridation of water supplies. Br Dent J. 1965;119:529–534. [PubMed] [Google Scholar]
- INSPQ . Avis sur un projet de fluoration de l’eau. Québec: Government of Québec, Institut National de Santé Publique du Québec, Comité d’éthique de Santé Publique; 2011. [Google Scholar]
- ISQ (2011) Données démographiques régionales. Government of Québec, Institut de la Statistique, Québec. Available at http://www.stat.gouv.qc.ca/donstat/societe/demographie/dons_regnl/regional/index.htm. Accessed 14 May 2012
- Jackson D. Has the decline of dental caries in English children made water fluoridation both unnecessary and uneconomic? Br Dent J. 1987;162:170–173. doi: 10.1038/sj.bdj.4806063. [DOI] [PubMed] [Google Scholar]
- Jones CM, Taylor GO, Whittle JG, Evans D, Trottier DP. Water fluoridation, tooth decay in 5 year olds, and social deprivation measured by the Jarman score: analysis of data from British dental surveys. BMJ. 1997;315:514–517. doi: 10.1136/bmj.315.7107.514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kumar JV, Swango PA, Lininger LL, Leske GS, Green EL, Haley VB. Changes in dental fluorosis and dental caries in Newburgh and Kingston, New York. Am J Public Health. 1998;88:1866–1870. doi: 10.2105/AJPH.88.12.1866. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Levy M, Corbeil F, Fortin C, Lamarre JR, Lavallière A, Schwartz S, et al. Fluoration de l’eau : analyse des bénéfices et des risques pour la santé: avis scientifique. Développement des individus et des communautés. Québec: Government of Québec, Institut National de la Santé Publique du Québec; 2007. [Google Scholar]
- Macek MD, Matte TD, Sinks T, Malvitz DM. Blood lead concentrations in children and method of water fluoridation in the United States, 1988–1994. Environ Heal Perspect. 2006;114(1):130–134. doi: 10.1289/ehp.8319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McDonagh MS, Whiting PF, Wilson PM, Sutton AJ, Chestnutt I, Cooper J, et al. Systematic review of water fluoridation. BMJ. 2000;321(7265):855–859. doi: 10.1136/bmj.321.7265.855. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLaren L, Emery JCH (2012). Drinking water fluoridation and oral health inequalities in Canadian children. Canadian J Public Health 103(Suppl 1):S49–S56. Available at http://www.ucalgary.ca/phirc/pdf/CJPH%202012%20McLaren%20&%20Emery.pdf. Accessed 12 November 2012 [DOI] [PMC free article] [PubMed]
- MMWR Fluoride Recommendations Work Group (2001) Recommendations for using fluoride to prevent and control dental caries in the United States. MMWR Recommendations and Reports, vol 50. Centres for Disease Control and Prevention, Morbidity and Mortality Weekly Report, Atlanta, GA. Available at http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5014a1.htm. Accessed 14 May 2012 [PubMed]
- Montmarquette C, Scott I. Taux d’actualisation pour l’évaluation des investissements publics au Québec. Research report. Montreal: Centre for Interuniversity Research and Analysis on Organizations (CIRANO); 2007. [Google Scholar]
- MSSS (2006) Plan d’action de santé dentaire publique 2005–2012. Government of Québec, Ministry of Health and Social Services, Public Health Directorate, Québec. Available at: http://publications.msss.gouv.qc.ca/acrobat/f/documentation/2006/06-231-01.pdf. Accessed 14 May 2012
- Osterman JW. Evaluating the impact of municipal water fluoridation on the aquatic environment. Am J Public Health. 1990;80(10):1230–1235. doi: 10.2105/AJPH.80.10.1230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pollick HF. Water fluoridation and the environment: a current perspective in the United States. Int J Occup Environ Heal. 2004;10:343–350. doi: 10.1179/oeh.2004.10.3.343. [DOI] [PubMed] [Google Scholar]
- Provart SJ, Carmichael CL. The relationship between caries, fluoridation and material deprivation in five-year-old children in County Durham. Community Dent Health. 1995;12:200–203. [PubMed] [Google Scholar]
- Quiñonez RB, Downs SM, Shugars D, Christensen J, Vann WF., Jr Assessing cost-effectiveness of sealant placement in children. J Public Health Dent. 2005;65(2):82–89. doi: 10.1111/j.1752-7325.2005.tb02791.x. [DOI] [PubMed] [Google Scholar]
- RAMQ (2006) Manuel des dentistes (no. 200). Régie de l’assurance-maladie du Québec, mise à jour 43. http://www.ramq.gouv.qc.ca/fr/professionnels/manuels/200/000_complet_dentiste.pdf. Accessed 14 May 2012
- Reeves TG. Water fluoridation: a manual for engineers and technicians. Atlanta, GA: US Department of Health and Human Services, Public Health Service, Centres for Disease Control and Prevention; 1986. [Google Scholar]
- Régie de l’énergie du Québec (2010) Bulletin d’information sur les prix des produits pétroliers au Québec. Essence ordinaire – revue annuelle 2010 – ensemble du Québec. Government of Québec, Régie de l’énergie, Québec. Available at: http://www.regie-energie.qc.ca/energie/prodpetro/Essence_EnsQc_2010.pdf. Accessed 14 August 2012
- Ringelberg ML, Allen SJ, Brown LJ. Cost of fluoridation: 44 Florida communities. J Public Health Dent. 1992;52:75–80. doi: 10.1111/j.1752-7325.1992.tb02247.x. [DOI] [PubMed] [Google Scholar]
- Rossi PH, Lipsey MW, Freeman HE. Evaluation: a systematic approach. Thousand Oaks, CA: Sage; 2004. [Google Scholar]
- Sanderson D. Water fluoridation: an economics perspective. York, UK: York Health Economics Consortium, University of York; 1998. [Google Scholar]
- Sanderson D, Wilson A. The cost-effectiveness of fluoridation. Report for Yorkshire Health and Trent Health. York, UK: University of York; 1994. [Google Scholar]
- Schock MR, Metz DH, Dionysious D (2006) Predicting lead dissolution in drinking water distribution systems: the effect of fluoride additives on lead solubility and corrosion. Presentation at the AWWA Conference, Cleveland, OH
- Sköld UM, Petersson LG, Birkhed D, Norlund A. Cost-analysis of school-based fluoride varnish and fluoride rinsing programs. Acta odontologica Scandinavica. 2008;66:286–292. doi: 10.1080/00016350802293978. [DOI] [PubMed] [Google Scholar]
- Slade GD, Spencer AJ, Davies MJ, Stewart JF. Influence of exposure to fluoridated water on socioeconomic inequalities in children’s caries experience. Community Dent Oral Epidemiol. 1996;24:89–100. doi: 10.1111/j.1600-0528.1996.tb00822.x. [DOI] [PubMed] [Google Scholar]
- Statistics Canada (2011) Canada’s population estimates. Government of Canada, Statistics Canada, Ottawa. Available at http://www.statcan.gc.ca/daily-quotidien/120321/dq120321e-eng.htm. Accessed 14 May 2012
- Tacoma-Pierce County Health Department (2002) Tacoma-Pierce County Health Department fluoridation resolution. WAC 197-11-960. Environmental checklist Tacoma-Pierce County Health Department, Tacoma, WA
- Truman BI, Gooch BF, Sulemana I, Gift HC, Horowitz AM, Evans CA, et al. Reviews of evidence on interventions to prevent dental caries, oral and pharyngeal cancers, and sports-related craniofacial injuries. Am J Prev Med. 2002;23(Suppl 1):21–54. doi: 10.1016/S0749-3797(02)00449-X. [DOI] [PubMed] [Google Scholar]
- Wallis P, Gehr R, Anderson P. Fluorides in wastewater discharges: toxic challenges to the St. Lawrence River Biological Community. Water Qual Res J Canada. 1996;31(4):809–838. [Google Scholar]
- Weiss C (1998) Evaluation: methods for studying programs and policies, 2nd edn. Prentice Hall, Upper Saddle River, NJ