

Abstract
Background. Infection with Helicobacter pylori contributes to the etiopathogenesis of various extragastrointestinal conditions, yet its etiological association with either symptomatic or asymptomatic dialysis patients remains inconclusive. Methods. Two researchers working independently conducted a literature search of the online databases PubMed, EMBase, ScienceDirect, and Cochrane Central Register of Controlled Trials to identify relevant articles to the end of 2012. Case-control and cross-sectional studies that met the inclusion criteria were included. Results. Fifteen studies involving 1237 dialysis patients and 1568 controls with normal renal function were included. Compared with normal controls, dialysis patients overall were associated with a relatively lower risk of H. pylori infection though not statistically significant. A significant inverse association was found between H. pylori prevalence and duration of treatments in those who were dialyzed >4 years (odds ratio 0.28; 95% confidence interval 0.22–0.36, P < 0.00001). No relationship between H. pylori status and duration of dialysis was observed in CRF patients. There were no significant differences in endoscopic features between patients and controls. Conclusions. Our meta-analysis found no evidence of a significant association between infection with H. pylori and dialysis overall, whereas long-term treatments of more than four years had a significant protective effect.
1. Introduction
Helicobacter pylori, an infectious organism, is present in about 50% of the global population, and the infection levels exceed 70% in some developing areas [1]. Infection with H. pylori has been implicated not only in the etiopathogenesis of gastrointestinal disease, such as gastritis, ulcerative diseases, low-grade mucosa-associated lymphoid tissue lymphoma, and gastric malignancies [2], but also in various extragastrointestinal conditions, among them chronic renal disease [3].
From 25% to 75% of chronic renal failure (CRF) patients who receive hemodialysis or continuous ambulatory peritoneal dialysis (CAPD) for long periods experience gastrointestinal troubles [4]. It has been postulated that high urea concentration makes the gastric mucosa of these patients more susceptible to colonization by H. pylori [5]. However, an etiological association between H. pylori and either symptomatic or asymptomatic dialysis patients remains inconclusive.
The prevalence of H. pylori infection in CRF patients may be as high as 64% and significantly higher in dialysis patients than in normal controls [6–9]. Others [10–12] report quite the opposite. Many factors would seem to contribute to the inhibition of H. pylori growth in the stomach of CRF patients (e.g., higher levels of proinflammatory cytokines, impaired immune system, increased pH, higher blood urea levels, and antibiotic treatment). Nevertheless, some studies [13–19] found no difference in the prevalence of H. pylori infection between patients on dialysis and healthy controls, leading to the conclusion that the level of urea is not a risk factor predisposing to H. pylori infection in this population. Because of these conflicting reports, the seriousness of H. pylori infection in dialysis patients remains unclear.
The number of dialysis patients increases by 7% annually [20], and it is therefore imperative to resolve some important issues concerning H. pylori infection in dialysis patients. The present study is a meta-analysis, designed to help clarify the prevalence of H. pylori in CRF patients as well as the relationship between dialysis duration and the prevalence of H. pylori. In addition, H. pylori status in CRF patients and the course of dialysis will be discussed.
2. Materials and Methods
2.1. Literature Sources and Searches
We systematically searched the databases MEDLINE, EMBASE, ScienceDirect, and Cochrane Central Register of Controlled Trials (CENTRAL) for relevant articles and abstracts published in English (ending 31 December 2012). Terms and keywords used to identify articles in Medical Subject Headings (MeSH) were Helicobacter pylori/H. pylori, and dialysis ((“Helicobacter pylori” OR “H. pylori”) AND “dialysis”). Two reviewers (MG and SPX) manually screened each eligible article's title, abstract, and full text to independently determine if the article met the inclusion criteria (below). Differences between the reviewers were solved by consensus.
2.2. Inclusion and Exclusion Criteria
For inclusion in the meta-analysis, case-control or cross-sectional studies had to report data on the rate of H. pylori infection in patients with and without dialysis and include a control group with normal renal function; base diagnosis of H. pylori infection on histology (e.g., Giemsa stain or Warthin-Starry method), culture, immunoglobulin G (IgG) antibody detection, rapid urease test, or urea breath test; concern human subjects only; and be published in English. Studies were excluded that were case reports, observational studies without control groups, review of the literature, or duplicated reports; if data on H. pylori infection in the dialysis group or control group was incomplete or unavailable; or if subjects had a history of drug use for antibiotics, H2 blockers, proton pump inhibitors, or bismuth within 4 weeks.
2.3. Data Extraction
Two independent reviewers extracted the information from the included articles. Discrepancies in the extraction were resolved by mutual discussion. For each study, the following data were collected: author; publication year; country; study design; basic characteristics of patients including number of patients with and without dialysis and type and duration of dialysis; detection methods for H. pylori infection and endoscopic abnormalities.
2.4. Data Analysis
The software Review Manager (RevMan, version 5.1, Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2011) was used to analyze the data. We arranged eligible articles chronologically, starting with the earliest. The odds ratios (ORs) and their 95% confidence intervals (CIs) for major outcomes were estimated in a fixed model or random model for each study. Statistical heterogeneity was evaluated with the I 2 statistic, and I 2 > 50% indicated substantial heterogeneity [29], in which case the condition random effects model was used. The differences were considered statistically significant when a P value was less than 0.05.
3. Results
3.1. Basic Information and Characteristics
The literature search initially yielded 152 articles relevant to the topic (Figure 1). Eighty-eight of these were excluded for not meeting the inclusion criteria. The full texts of the remaining 64 citations were carefully reviewed. Ultimately, 49 of the 64 were excluded due to the use of certain drugs within 4 weeks or for meeting any other of the exclusion criteria. This process left 15 qualified essays (Table 1).
Figure 1.
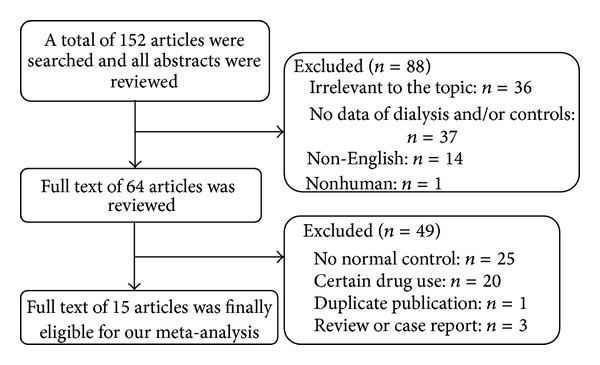
Flow chart of the eligibility selection process.
Table 1.
Basic information of eligible articles.
| Author (ref.) | Year | Country | Study design | Age, y | Test confirming infection | Duration of dialysis, m | Dialysis type, n | HP(+), n | ||
|---|---|---|---|---|---|---|---|---|---|---|
| HD | CAPD | Controls | Dialysis | |||||||
| Shousha et al. [13] | 1990 | UK | Case-control | HP(+) 54 ± 14.3 HP(−) 48 ± 14.2 |
Warthin-Starry, Giemsa | NG | NG | NG | 51/120 | 12/50 |
| Jaspersen et al. [10] | 1995 | Germany | Case-control | 58.2 ± 12.6 | Urease test, Giemsa | NG | 7/34 | 0 | 47/127 | 7/34 |
| Krawczyk et al. [14] | 1996 | Poland | Case-control | 36.8 ± 13.2 | Urease test, Giemsa | 28 ± 12.2 | 13/21 | 0 | 14/22 | 13/21 |
| Ozgür et al. [15] | 1997 | Turkey | Case-control | 37.27 ± 14.08 | Urease test | 28.87 ± 28.92 | 28/47 | 0 | 64/100 | 28/47 |
| Gür et al. [21] | 1999 | Turkey | Case-control | HP(+) 35.1 ± 4.2 HP(−) 32.5 ± 5.3 |
Urease test, histology | HP(+) 21.2 ± 16.4 HP(−) 21.8 ± 11.4 |
25/45 | 0 | 24/44 | 25/45 |
| Araki et al. [4] | 1999 | Japan | Case-control | 57.4 ± 12.8 | Histology, culture | 91.2 ± 62.4 | NG/54 | NG/9 | 42/64 | 29/63 |
| Yildiz et al. [22] | 1999 | Turkey | Cross-sectional | 36.6 ± 15.2 | ELISA (IgG) | 32.5 ± 27.7 | NG | NG | 39/55 | 31/47 |
| Tamura et al. [23] | 1999 | Japan | Case-control | 52.2 ± 1.8 | Urease test, histology, and culture | 29.3 ± 5.4 | 20/41 | 5/8 | 26/48 | 25/49 |
| Blusiewicz et al. [24] | 2005 | Poland | Case-control | 50.8 ± 2.9 | Urease test, histology | NG | 19/30 | 0 | 22/31 | 19/30 |
| Khedmat et al. [6] | 2007 | Iran | Case-control | 47.9 ± 3.5 | Urease test | 46.9 ± 10.7 | 46/73 | 0 | 106/305 | 46/73 |
| Khazaei et al. [25] | 2008 | Iran | Case-control | 14.7 ± 3.4 | Urease test, histology | HP(+) 22.5 ± 18.5 HP(−) 26.9 ± 32.5 |
16/24 | 0 | 5/25 | 16/24 |
| Gioè et al. [26] | 2008 | Italy | Case-control | NG | RUT, Giemsa | NG | 75/142 | 0 | 59/132 | 75/142 |
| Asl and Nasri [27] | 2009 | Iran | Cross-sectional | 56 ± 14 | Giemsa | ≥6 | 28/40 | 0 | 23/40 | 28/40 |
| Sugimoto et al. [11] | 2009 | Japan | Case-control | 58.8 ± 0.4 | ELISA (IgG) | 100.8 ± 3.6 | NG | NG | 314/400 | 262/539 |
| Chang et al. [28] | 2010 | Korea | Case-control | 62 ± 9.8 | RUT, histology | HP(+) 56.8 ± 26.9 HP(−) 66.4 ± 26.1 |
12/33 | 0 | 36/55 | 12/33 |
Ref.: reference; HD: hemodialysis; CAPD: continuous ambulatory peritoneal dialysis; NG: not given; RUT: rapid urease test.
3.2. Overall Analysis
These 15 articles comprised 1237 dialysis patients and 1568 controls with normal renal function. Since I 2 was greater than 50%, a random model was applied. Pooled data showed that there was no difference in H. pylori prevalence between the dialysis (hemodialysis and CAPD) patients and normal controls (OR = 0.86, 95% CI: 0.52–1.42, P = 0.55; Figure 2(a)). A subanalysis showed no difference in H. pylori infection between patients receiving hemodialysis and the control group (OR = 1.11, 95% CI: 0.69–1.81, P = 0.66; Figure 2(b)). A funnel plot indicated that there was no publication bias (Figure 3).
Figure 2.
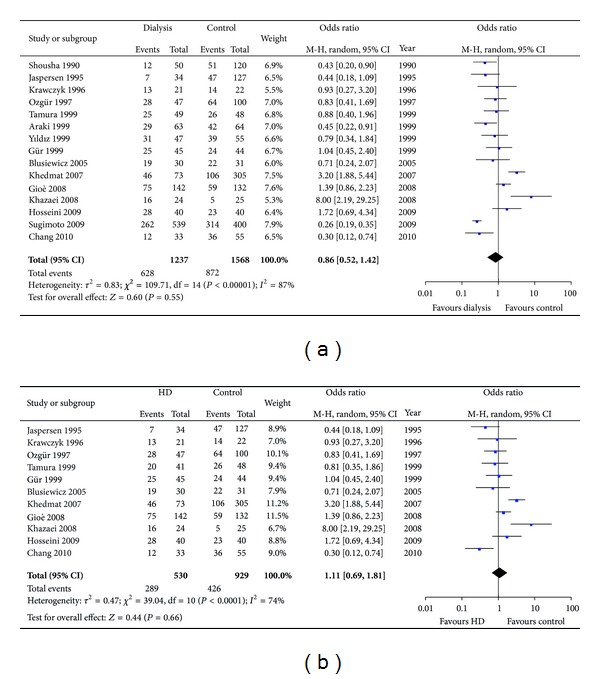
(a) Prevalence of H. pylori in dialysis patients and controls with normal renal function. (b) The prevalence of H. pylori in hemodialysis patients and controls with normal renal function.
Figure 3.
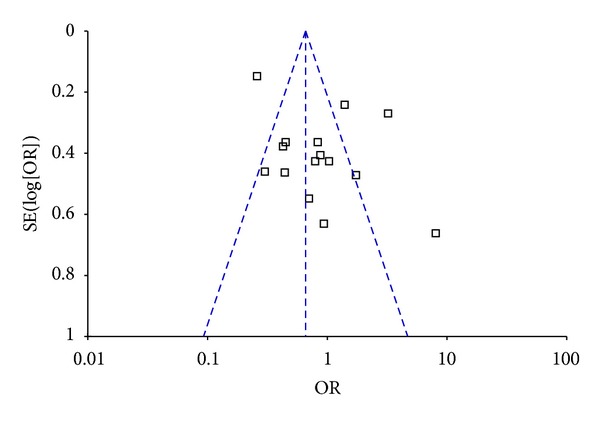
Funnel plot for 15 studies.
In this meta-analysis, various methods were adopted to confirm H. pylori infection as stated previously. As we all know, IgG antibody detection cannot judge present infection of H. pylori, since serum antibodies specific to H. pylori would still remain for several months after successful eradication, nevertheless; serology is the only test which is not affected by local changes in the stomach that could lead to a low bacterial load and to false negative results of the other tests and it is the third method commonly used as a noninvasive method to diagnose H. pylori infection [30]. In order to exclude the probability that different methods for H. pylori detection would lead to different outcomes, we chose to exclude 2 articles [11, 22] which only utilized IgG to detect H. pylori infection. However, subsequent analysis again found no differences between the two groups (Figure 4). Still, we wanted to detect if other detection methods like rapid urease test (RUT) would influence the overall analysis, while more than one kind of detection method was involved in the other studies included in our meta-analysis. The data of other detection methods cannot be analyzed separately.
Figure 4.
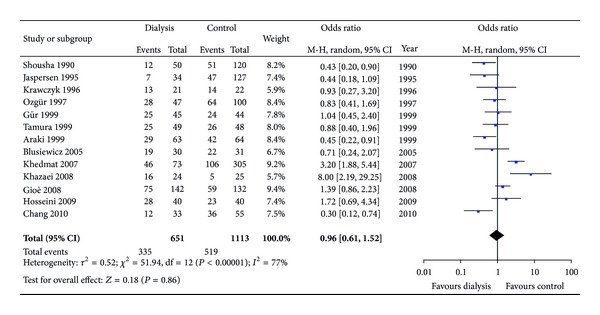
Various methods for detecting H. pylori infection (excluding IgG titer).
3.3. Effect of Dialysis Duration on H. pylori Prevalence
Some studies have indicated that the rate of H. pylori infection decreases over a prolonged course of hemodialysis. Hence we performed a subgroup meta-analysis of H. pylori infection and the duration of dialysis (Figures 5(a) and 5(b)). Those who underwent dialysis longer than four years [4, 11, 28] indeed showed a significantly lower rate of H. pylori infection (P < 0.00001) than those with normal renal function, while it is another story when it comes to those who endured dialysis duration shorter than four years [6, 14, 15, 21–23, 25] (P = 0.27) with no difference in H. pylori infection rate between two groups.
Figure 5.
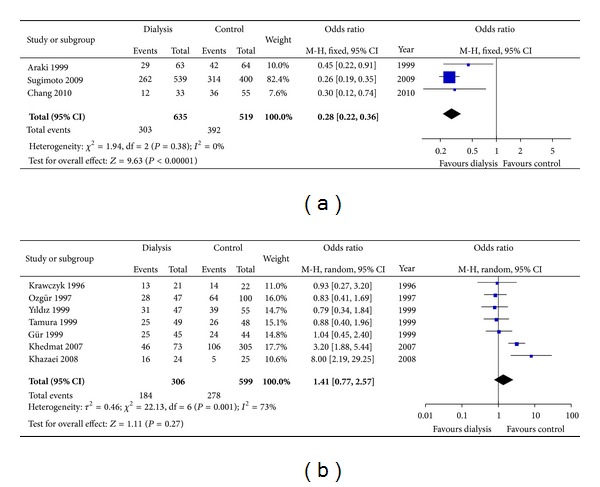
(a) Effect of dialysis duration (>4 years) on H. pylori prevalence. (b) Effect of dialysis duration (≤4 years) on H. pylori prevalence.
3.4. Effect of H. pylori Status on Duration of Dialysis
A few previous studies have shown that H. pylori positive patients required a significantly shorter course of dialysis than uninfected patients [22, 31]. Among the included studies, five studies [4, 15, 21, 22, 25, 28] evaluated the relationship between H. pylori status and duration of dialysis. However, no statistical significance was observed between H. pylori negative and H. pylori positive patients. The weighted mean difference between these studies was 4.56 (95% CI: −1.55–10.67, P = 0.14) (Figure 6).
Figure 6.
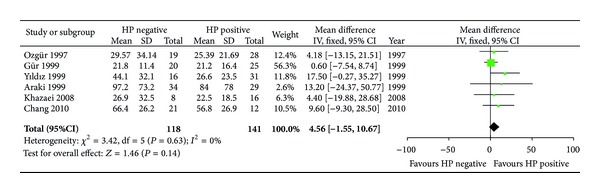
Association between H. pylori status and duration of dialysis in CRF patients.
3.5. Endoscopic Findings
We compared the endoscopic findings between the dialysis and control groups, mainly concerning gastritis and ulcerative diseases. Ten studies [4, 6, 10, 11, 13, 15, 21, 24, 26, 28] provided detailed endoscopic information regarding, for example, gastritis, ulcerative diseases, and intestinal metaplasia. The incidence of gastritis and ulcerative diseases in dialysis patients and normal controls was 66.2% versus 56.2% (P = 0.99) and 13.7% versus 24.9% (P = 0.08), respectively. There are no significant differences in endoscopic abnormities between the dialysis patients and the controls with normal renal function (Figures 7(a) and 7(b)).
Figure 7.
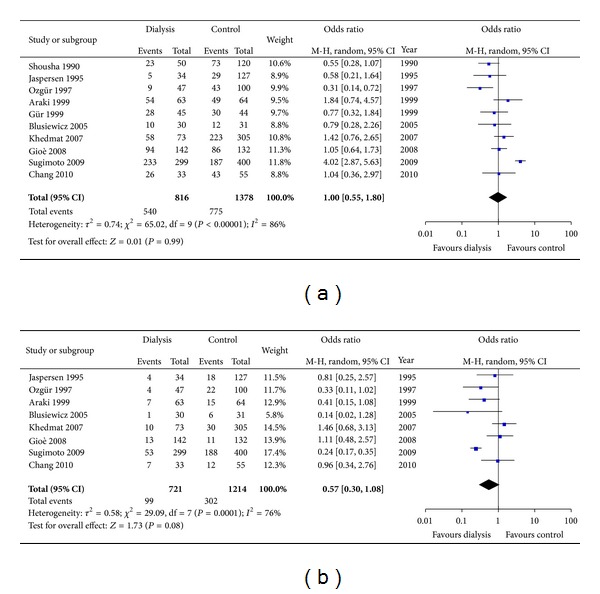
(a) Incidence of gastritis between CRF patients on dialysis and normal controls. (b) Incidence of ulcer diseases between CRF patients on dialysis and normal controls.
4. Discussion
Recently, more and more evidence has shown that H. pylori is related to extragastrointestinal diseases such as iron deficiency anemia, idiopathic thrombocytopenic purpura [32], and diabetes mellitus [33]. Moreover, patients with CRF usually suffer from systemic or local chronic circulatory failure (or both) [34], hypergastrinemia [21], high ammonia levels [35], and enhanced inflammation that facilitates H. pylori infection. In the present study, we performed a meta-analysis and found that CRF patients on dialysis treatment had an overall H. pylori infection rate of ~50.8%, which was relatively but not significantly lower than the 55.6% in controls (P = 0.55).
Upon investigating the association between H. pylori infection and the different types of dialysis, we found that H. pylori infection was not statistically associated with hemodialysis specifically. However, the H. pylori infection rate in the hemodialysis group (54.5%) was slightly higher than that of the control (45.9%), which contrasts with the results of the overall analysis. Due to lack of data, we were not able to analyze the difference in H. pylori prevalence between CRF patients undergoing CAPD and those receiving hemodialysis. Thus, our results from these studies revealed that the prevalence of H. pylori infection is similar between CRF patients who were receiving dialysis and the control group with normal renal function (P > 0.05).
From the results of the present study, it appears that CRF treatment with dialysis does not change the probability of H. pylori infection. Although one researcher went against current thought and concluded that the level of urea is not a risk factor in H. pylori colonization [28], neither theory has proved definitive and more research is required to clarify the issue. Among the included studies in our meta-analysis, some researchers [4, 11, 13, 28] found that the prevalence of H. pylori in CRF patients undergoing dialysis was significantly lower than in non-CRF controls with or without gastrointestinal symptoms. The truth is that many CRF patients who receive dialysis inevitably have access to antibiotics, proton pump inhibitors, or H2 receptor antagonists which then influence the H. pylori infection rate to some extent [13, 36]. Moreover, gastric atrophy progresses along with decreased secretion of acid [37] as well as higher levels of proinflammatory cytokines [38] in CRF patients, making H. pylori difficult to survive. Apart from these, the prevalence of H. pylori varies widely across different demographic and geographic areas due to economic situations, sanitary conditions, cultural habits, and more.
Our subgroup analysis revealed that the prevalence of H. pylori of those patients who were on dialysis for longer than 4 years was significantly lower than of individuals with normal renal function, while the duration of dialysis between H. pylori negative and H. pylori positive patients did not differ from each other. It is in accordance with other studies. Sugimoto et al. [11] showed that the prevalence of H. pylori infection decreased in the first 4 years of dialysis and plateaued after 5 years of treatment and it was not affected by basement diseases. He and his colleagues concluded that more than one-third of patients who had received approximately four years of dialysis treatments had been naturally cured of H. pylori infections. Nakajima et al. [31] also reported that the prevalence of H. pylori decreased along with extended hemodialysis duration of two years and more. They declared that the reduction of H. pylori prevalence in long-term dialysis patients was due to reduction of gastric acid secretion related to chronic gastritis or frequent antibiotic consumption. Nevertheless there are actually conflicts about the relationship between H. pylori status and duration of dialysis. Several studies argued that duration of dialysis was inversely related to H. pylori colonization in dialysis patients [39–41], and some found an opposite result [42]. Yet, the underlying mechanism is still obscure. More investigations are warranted to be conducted to elucidate these findings in the future.
Endoscopic abnormities such as erosive gastritis, duodenitis, and peptic ulcers are often found in CRF and dialysis patients. In some studies, peptic ulcers and gastroduodenal mucosa lesions were associated with H. pylori infection [43–47]. Khedmat et al. [6] showed that there was no significant difference in the rate of nonerosive gastritis, duodenitis, and gastric ulcer diseases between hemodialysis patients and those with normal renal function. These findings are in accordance with the results of our present meta-analysis, which indicated no statistical differences between dialysis patients and normal controls (P > 0.05) concerning endoscopic gastritis and ulcerative diseases. Thus it seems that dialysis itself is not a risk factor for the occurrence of gastritis or ulcers, although it is still necessary to perform endoscopy in dialysis patients with gastrointestinal symptoms. However, the above results rarely came from children's studies. Whether to recommend upper gastrointestinal examination based on symptoms requires more consideration in pediatric dialysis patients.
Although in the present meta-analysis we found no significant difference in H. pylori prevalence between dialysis patients and control subjects, according to some studies [21, 48, 49] successful eradication of H. pylori would lead to a significant decrease in dyspeptic symptoms, improvement in upper endoscopic results, and reduction in serum gastrin concentrations among hemodialysis patients. In such patients, due to impaired renal function and decline in the rate of excretion of drugs, the ideal treatment regimen should emphasize high efficacy and few adverse effects. Seyyedmajidi et al. conducted a randomized controlled trial comparing sequential therapy and standard triple therapy for H. pylori eradication in uraemic and nonuraemic patients. The eradication rates did not differ with both sequential and standard therapeutic regimens in the patients and normal controls. They preferred the standard triple therapy due to its lower side effects and complexity [50]. Chang et al. [28] found that a 7-day triple therapy with a low-dose OAC (omeprazole, amoxicillin, and clarithromycin) regimen was effective and safe for eradication of H. pylori infection in hemodialysis patients, with the consideration that amoxicillin and clarithromycin are primarily eliminated via the renal route. Further studies investigating the effect of eradication of H. pylori on symptom relief of dialysis patients are necessary.
When weighing the findings of the present meta-analysis, it is imperative to note that these studies were all case-control or cross-sectional studies, each performed at a single center with a cohort, and the sociodemographic characteristics of the populations were unclear. Although we adjusted for potential confounders, heterogeneity still existed among the study designs; confounding is an intrinsic limitation of these observational studies, so we precluded any assessment of causality in reported associations. Also, variables such as age and gender may be important considerations in the analysis of risk factors, but here we were unable to adjust for them, mainly due to incomplete data.
5. Conclusion
In the present meta-analysis there was no evidence of a significant association between infection with H. pylori and dialysis treatments for CRF patients. With heterogeneity limiting certainty of this association, there is a need for well-conducted randomized controlled trials to further verify these findings. According to subgroup analysis dialysis treatments for more than 4 year appears to have a protective effect against H. pylori infection; mechanistic studies of this negative association are needed to be further identified. It is indeterminable whether H. pylori status would affect duration of dialysis in CRF patients or whether endoscopic abnormalities of dialysis patients are related to H. pylori infection; further clinical studies investigating the effect of H. pylori infection on endoscopic findings of dialysis patients are necessary.
Conflict of Interests
The authors declare no conflict of interests.
Authors' Contribution
Min Gu and Shuping Xiao contributed equally to the work.
Acknowledgment
This work was supported by Grants from the National Natural Science Foundation of China (nos. 81072032 and 81270476).
References
- 1.Rocha GA, Queiroz DM, Mendes EN, et al. Indirect immunofluorescence determination of the frequency of anti-H. pylori antibodies in Brazilian blood donors. Brazilian Journal of Medical and Biological Research. 1992;25(7):683–689. [PubMed] [Google Scholar]
- 2.Huang JJ, Huang CJ, Ruaan MK, Chen KW, Yen TS, Sheu BS. Diagnostic efficacy of 13C-urea breath test for Helicobacter pylori infection in hemodialysis patients. The American Journal of Kidney Diseases. 2000;36(1):124–129. doi: 10.1053/ajkd.2000.8284. [DOI] [PubMed] [Google Scholar]
- 3.van Vlem B, Schoonjans R, Vanholder R, et al. Delayed gastric emptying in dyspeptic chronic hemodialysis patients. The American Journal of Kidney Diseases. 2000;36(5):962–968. doi: 10.1053/ajkd.2000.19094. [DOI] [PubMed] [Google Scholar]
- 4.Araki H, Miyazaki R, Matsuda T, Gejyo F, Koni I. Significance of serum pepsinogens and their relationship to Helicobacter pylori infection and histological gastritis in dialysis patients. Nephrology Dialysis Transplantation. 1999;14(11):2669–2675. doi: 10.1093/ndt/14.11.2669. [DOI] [PubMed] [Google Scholar]
- 5.Hazell SL, Lee A. Campylobacter pyloridis, urease, hydrogen ion back diffusion, and gastric ulcers. The Lancet. 1986;2(8497):15–17. doi: 10.1016/s0140-6736(86)92561-4. [DOI] [PubMed] [Google Scholar]
- 6.Khedmat H, Ahmadzad-Asl M, Amini M, et al. Gastro-duodenal lesions and Helicobacter pylori infection in uremic patients and renal transplant recipients. Transplantation Proceedings. 2007;39(4):1003–1007. doi: 10.1016/j.transproceed.2007.03.034. [DOI] [PubMed] [Google Scholar]
- 7.Schoonjans R, Van VB, Vandamme W, et al. Dyspepsia and gastroparesis in chronic renal failure: the role of Helicobacter pylori . Clinical Nephrology. 2002;57(3):201–207. doi: 10.5414/cnp57201. [DOI] [PubMed] [Google Scholar]
- 8.Aydemir S, Boyacioglu S, Gur G, et al. Helicobacter pylori infection in hemodialysis patients: susceptibility to amoxicillin and clarithromycin. World Journal of Gastroenterology. 2005;11(6):842–845. doi: 10.3748/wjg.v11.i6.842. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gladziwa U, Haase G, Handt S, et al. Prevalence of Helicobacter pylori in patients with chronic renal failure. Nephrology Dialysis Transplantation. 1993;8(4):301–306. [PubMed] [Google Scholar]
- 10.Jaspersen D, Fassbinder W, Heinkele P, et al. Significantly lower prevalence of Helicobacter pylori in uremic patients than in patients with normal renal function. Journal of Gastroenterology. 1995;30(5):585–588. doi: 10.1007/BF02367783. [DOI] [PubMed] [Google Scholar]
- 11.Sugimoto M, Sakai K, Kita M, Imanishi J, Yamaoka Y. Prevalence of Helicobacter pylori infection in long-term hemodialysis patients. Kidney International. 2009;75(1):96–103. doi: 10.1038/ki.2008.508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Korzonek M, Szymaniak L, Giedrys-Kalemba S, Ciechanowski K. Is it necessary to treat Helicobacter pylori infection in patients with end-stage renal failure and renal transplant recipients? Polskie Archiwum Medycyny Wewnetrznej. 2004;111(3):297–304. [PubMed] [Google Scholar]
- 13.Shousha S, Arnaout AH, Abbas SH, Parkins RA. Antral Helicobacter pylori in patients with chronic renal failure. Journal of Clinical Pathology. 1990;43(5):397–399. doi: 10.1136/jcp.43.5.397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Krawczyk W, Górna E, Suwala J, et al. Frequency of Helicobacter pylori infection in uremic hemodialyzed patients with antral gastritis. Nephron. 1996;74(3):621–622. doi: 10.1159/000189465. [DOI] [PubMed] [Google Scholar]
- 15.Ozgür O, Boyacioğlu S, Ozdoğan M, Gür G, Telatar H, Haberal M. Helicobacter pylori infection in haemodialysis patients and renal transplant recipients. Nephrology Dialysis Transplantation. 1997;12:289–291. doi: 10.1093/ndt/12.2.289. [DOI] [PubMed] [Google Scholar]
- 16.Loffeld RJLF, Peltenburg HG, Oever HVD, Stobberingh E. Prevalence of Helicobacter pylori antibodies in patients on chronic intermittent haemodialysis. Nephron. 1991;59(2):250–253. doi: 10.1159/000186560. [DOI] [PubMed] [Google Scholar]
- 17.Luzza F, Imeneo M, Maletta M, et al. Helicobacter pylori-specific IgG in chronic haemodialysis patients: relationship of hypergastrinaemia to positive serology. Nephrology Dialysis Transplantation. 1996;11(1):120–124. [PubMed] [Google Scholar]
- 18.Fabrizi F, Martin P. Helicobacter pylori infection in patients with end-stage renal disease. International Journal of Artificial Organs. 2000;23(3):157–164. [PubMed] [Google Scholar]
- 19.Asl MKH, Nasri H. Prevalence of Helicobacter pylori infection in maintenance hemodialysis patients with non-ulcer dyspepsia. Saudi Journal of Kidney Diseases and Transplantation. 2009;20(2):223–226. [PubMed] [Google Scholar]
- 20.Lysaght MJ. Maintenance dialysis population dynamics: current trends and long-term implications. Journal of the American Society of Nephrology. 2001;13(supplement 1):S37–S40. [PubMed] [Google Scholar]
- 21.Gür G, Boyacioglu S, Gül C, et al. Impact of Helicobacter pylori infection on serum gastrin in haemodialysis patients. Nephrology Dialysis Transplantation. 1999;14(11):2688–2691. doi: 10.1093/ndt/14.11.2688. [DOI] [PubMed] [Google Scholar]
- 22.Yildiz A, Beşişik F, Akkaya V, et al. Helicobacter pylori antibodies in hemodialysis patients and renal transplant recipients. Clinical Transplantation. 1999;13(1, part 1):13–16. doi: 10.1034/j.1399-0012.1999.t01-1-130102.x. [DOI] [PubMed] [Google Scholar]
- 23.Tamura H, Tokushima H, Murakawa M, et al. Influences of Helicobacter pylori on serum pepsinogen concentrations in dialysis patients. Nephrology Dialysis Transplantation. 1999;14(1):113–117. doi: 10.1093/ndt/14.1.113. [DOI] [PubMed] [Google Scholar]
- 24.Blusiewicz K, Rydzewska G, Rydzewski A. Gastric juice ammonia and urea concentrations and their relation to gastric mucosa injury in patients maintained on chronic hemodialysis. Roczniki Akademii Medycznej w Białymstoku. 2005;50:188–192. [PubMed] [Google Scholar]
- 25.Khazaei MR, Imanieh MH, Al-Hashemi GH. Gastrointestinal evaluation in pediatric kidney transplantation candidates. Iranian Journal of Kidney Diseases. 2008;2(1):40–45. [PubMed] [Google Scholar]
- 26.Gioè FP, Cudia B, Romano G, et al. Role and clinical importance of Helicobacter pylori infection in hemodialysis patients. Il Giornale di Chirurgia. 2008;29(3):81–84. [PubMed] [Google Scholar]
- 27.Asl MKH, Nasri H. Prevalence of Helicobacter pylori infection in maintenance hemodialysis patients with non-ulcer dyspepsia. Saudi Journal of Kidney Diseases and Transplantation. 2009;20(2):223–226. [PubMed] [Google Scholar]
- 28.Chang WC, Jo YI, Park HS, et al. Helicobacter pylori eradication with a 7-day low-dose triple therapy in hemodialysis patients. Clinical and Experimental Nephrology. 2010;14(5):469–473. doi: 10.1007/s10157-010-0319-7. [DOI] [PubMed] [Google Scholar]
- 29.Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. British Medical Journal. 2003;327(7414):557–560. doi: 10.1136/bmj.327.7414.557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Malfertheiner P, Jo YI, Megraud F, O’Morain CA, et al. Management of Helicobacter pylori infection—the Maastricht IV/Florence consensus report. Gut. 2012;61(5):646–664. doi: 10.1136/gutjnl-2012-302084. [DOI] [PubMed] [Google Scholar]
- 31.Nakajima F, Sakaguchi M, Amemoto K, et al. Helicobacter pylori in patients receiving long-term dialysis. The American Journal of Nephrology. 2002;22(5-6):468–472. doi: 10.1159/000065278. [DOI] [PubMed] [Google Scholar]
- 32.Sato R, Murakami K, Okimoto T, Watanabe K, Kodama M, Fujioka T. Development of corpus atrophic gastritis may be associated with Helicobacter pylori-related idiopathic thrombocytopenic purpura. Journal of Gastroenterology. 2011;46(8):991–997. doi: 10.1007/s00535-011-0416-8. [DOI] [PubMed] [Google Scholar]
- 33.Zhou X, Zhang C, Wu J, Zhang G. Association between Helicobacter pylori infection and diabetes mellitus: a meta-analysis of observational studies. Diabetes Research and Clinical Practice. 2013;99:200–208. doi: 10.1016/j.diabres.2012.11.012. [DOI] [PubMed] [Google Scholar]
- 34.Block GA, Raggi P, Bellasi A, Kooienga L, Spiegel DM. Mortality effect of coronary calcification and phosphate binder choice in incident hemodialysis patients. Kidney International. 2007;71(5):438–441. doi: 10.1038/sj.ki.5002059. [DOI] [PubMed] [Google Scholar]
- 35.Neithercut WD, Rowe PA, el Nujumi AM, Dahill S, McColl KEL. Effect of Helicobacter pylori infection on intragastric urea and ammonium concentrations in patients with chronic renal failure. Journal of Clinical Pathology. 1993;46(6):544–547. doi: 10.1136/jcp.46.6.544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.de Vecchi AF, Quatrini M, Boni F, et al. Epidemiology of Helicobacter pylori in dialysis patients. Peritoneal Dialysis International. 1995;15(2):178–179. [PubMed] [Google Scholar]
- 37.Paimela H, Stenman S, Kekki M. Chronic gastritis and gastric acid secretion in uraemic and renal transplant patients. Hepatogastroenterology. 1985;32(1):15–19. [PubMed] [Google Scholar]
- 38.Hwang IR, Kodama T, Kikuchi S, et al. Effect of interleukin 1 polymorphisms on gastric mucosal interleukin 1β production in Helicobacter pylori infection. Gastroenterology. 2002;123(6):1793–1803. doi: 10.1053/gast.2002.37043. [DOI] [PubMed] [Google Scholar]
- 39.Nakajima F, Sakaguchi M, Oka H, et al. Prevalence of Helicobacter pylori antibodies in long-term dialysis patients. Nephrology. 2004;9(2):73–76. doi: 10.1111/j.1440-1797.2004.00239.x. [DOI] [PubMed] [Google Scholar]
- 40.Antoniou S, Dimitriadis A, Kliridou M, Pavlitou K, Batzili H, Malaka E. Prevalence of Helicobacter pylori antibodies in CAPD patients. Nephron. 1997;75(3):358–359. doi: 10.1159/000189563. [DOI] [PubMed] [Google Scholar]
- 41.Mortazavi F, Rafeey M. Endoscopic findings and Helicobacter pylori in children on long-term hemodialysis. Pakistan Journal of Biological Sciences. 2008;11(14):1840–1843. doi: 10.3923/pjbs.2008.1840.1843. [DOI] [PubMed] [Google Scholar]
- 42.Rasmi Y, Farshid S, Makhdomi K. Effect of duration on hemodialysis on prevalence of Helicobacter pylori infection. Saudi Journal of Kidney Diseases and Transplantation. 2012;23(3):489–492. [PubMed] [Google Scholar]
- 43.de Bustillo EM, Tomero JAS, Sanz JC, et al. Eradication and follow-up of Helicobacter pylori infection in hemodialysis patients. Nephron. 1998;79(1):55–60. doi: 10.1159/000044992. [DOI] [PubMed] [Google Scholar]
- 44.Offerhaus GJA, Kreuning J, Valentijn RM, et al. Campylobacter pylori: prevalence and significance in patients with chronic renal failure. Clinical Nephrology. 1989;32(5):239–241. [PubMed] [Google Scholar]
- 45.Marsenic O, Peco-Antic A, Perisic V, Virijevic V, Kruscic D, Kostic M. Upper gastrointestinal lesions in children on chronic haemodialysis. Nephrology Dialysis Transplantation. 2003;18(12):2687–2688. doi: 10.1093/ndt/gfg468. [DOI] [PubMed] [Google Scholar]
- 46.Emir S, Bereket G, Boyacioğlu S, Varan B, Tunali H, Haberal M. Gastroduodenal lesions and Helicobacter pylori in children with end-stage renal disease. Pediatric Nephrology. 2000;14(8-9):837–840. doi: 10.1007/s004679900254. [DOI] [PubMed] [Google Scholar]
- 47.Ala-Kaila K, Vaajalahti P, Karvonen AL, Kokki M. Gastric Helicobacter and upper gastrointestinal symptoms in chronic renal failure. Annals of Medicine. 1991;23(4):403–406. doi: 10.3109/07853899109148082. [DOI] [PubMed] [Google Scholar]
- 48.Tokushima H, Tamura H, Murakawa M, et al. Eradication of Helicobacter pylori restores elevation of serum gastrin concentrations in patients with end-stage renal disease. Internal Medicine. 1998;37(5):435–439. doi: 10.2169/internalmedicine.37.435. [DOI] [PubMed] [Google Scholar]
- 49.Tokushima H. Role of Helicobacter pylori in gastro-duodenal mucosal lesions in patients with end-stage renal disease under dialysis treatment. Nippon Jinzo Gakkai Shi. 1995;37(9):503–510. [PubMed] [Google Scholar]
- 50.Seyyedmajidi M, Falaknazi K, Mirsattari D, et al. Correlation between creatinine clearance and Helicobacter pylori infection eradication with sequential and triple therapeutic regimens: a randomised clinical trial. Arab Journal of Gastroenterology. 2011;12(3):150–153. doi: 10.1016/j.ajg.2011.07.004. [DOI] [PubMed] [Google Scholar]