

Abstract
Gingival recession is a condition that affects a large portion of the young and adult population and negatively affects the aesthetic aspects of the smile. Many factors are related to its development, including orthodontic movement beyond the osseous limits. Many treatment options have been proposed to cover the exposed root surface. The aim of this article was to describe three cases where a subepithelial connective tissue graft was performed, using a microsurgical technique, in the treatment of deep gingival recession after orthodontic treatment. This technique resulted in successful root coverage and keratinized tissue gain, improving the gingival esthetic pattern.
1. Introduction
Gingival recession can be defined as the location of marginal periodontal tissues apical to the cementoenamel junction [1]. This condition is prevalent in the young and adult populations [2]. The prevalence, extension, and severity of gingival recession have been observed to increase with age, affecting 79% of adults >40 years old in a representative sample of the Brazilian population [3]. It occurs in patients with either good or poor oral hygiene [4] and has multiple etiological factors [5] like traumatic tooth brushing [6], dehiscence, smoking, biological width invasion, inflammation, occlusal trauma, piercings [7], and orthodontic movement.
Although controversial, the scientific evidence demonstrates that gingival recession can develop in patients who undergo orthodontic movement [8, 9]. Furthermore, some studies have confirmed a positive correlation between the increase of severity and extension of gingival recession and orthodontic treatment [10].
The main factors related to the occurrence of gingival recession related to orthodontic movement are tooth movement beyond the osseous limits of the alveolar process and excessive tooth proclination during treatment, especially in adult patients [11, 12].
Thin gingival biotypes and the gingival inflammation associated with biofilm were observed as the risk factors for the development of gingival recession associated with orthodontic treatment [13].
There are several options for the treatment of gingival recession, including the free gingival graft [14], the sliding flap [15], the double pedicle flap [16], the subepithelial connective tissue graft [17], the enamel matrix derivative, the acellular dermal matrix, and growth factors [18–20].
The scientific evidence shows that the subepithelial connective tissue graft promotes higher levels of root coverage, high predictability and provides more gingival thickness [18–20].
As new techniques and materials are developed, new surgical approaches are necessary to minimize the surgical trauma and overcome the limitations related to the manual ability and natural vision of the surgeons. The incorporation of a surgical microscope to periodontal plastic surgery provides better illumination and adequate magnification to increase the precision of a surgeon's surgical skill. Thus, minimally invasive techniques were developed to minimize tissue trauma and allow primary wound closure [21–23].
The aim of this study is to report three cases where a subepithelial connective tissue graft was performed using a microsurgical approach to treat deep gingival recession after orthodontic treatment.
2. Case Reports
Three patients from a private dental clinic with aesthetic complaints related to deep gingival recession were included in this report. All patients were healthy and nonsmokers and signed an informed consent. The details about each patient are described as follows.
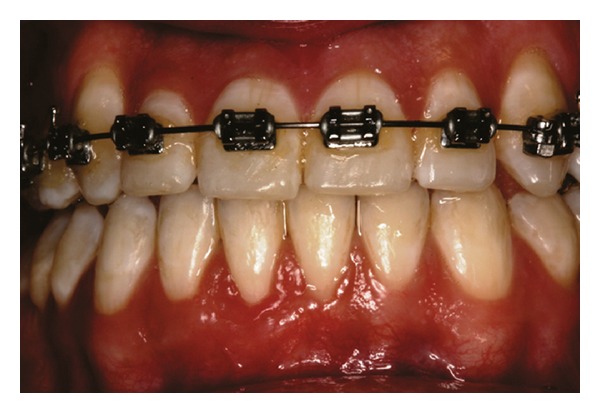
Patient 1: 27-year-old white female, having previous orthodontic treatment over a period of 5 years, presenting with a thin gingival biotype [24] and Miller [25] Class III gingival recession at the mandibular central incisors (Figure 1).
Figure 1.

Initial aspect of patient 1 showing Miller Class III localized gingival recessions at the mandibular central incisors.
Patient 2: 26-year-old white female, who started orthodontic treatment approximately 3 years earlier, presenting with a thick gingival biotype [24] and Miller [25] Class III gingival recession at the left mandibular central incisor (Figure 10).
Figure 10.

Initial aspect of patient 2 showing Miller class III localized gingival recession at the mandibular central left incisor.
Patient 3: 26-year-old white male, who started orthodontic treatment approximately 2 years earlier, presenting with a thin gingival biotype [24] and Miller [25] Class II gingival recession at the right mandibular central incisor (Figure 17).
Figure 17.

Initial aspect of patient 3 showing Miller Class II localized gingival recession at the mandibular central right incisor.
2.1. Initial Therapy
All patients were submitted to a plaque control program, which included oral hygiene instructions, scaling and root planning using an ultrasonic device, and crown polishing.
2.2. Surgical Therapy
All surgical procedures were performed by a single operator. A single 8 mg dose of dexamethasone was given to each patient one hour before surgery. Extraoral antisepsis was performed with a degerming agent and intraoral antisepsis was performed with a 0.12% chlorhexidine rinse. Mepivacaine (2.0%) with 1 : 100.000 epinephrine was used as an anesthetic solution.
All cases were performed using the microsurgical approach for root coverage, as described by De Campos et al. [22]. Initially, the exposed root surface was planned with a McCall 13/14 curette, followed by finishing burs. Citric acid gel (pH 1) was applied for 3 minutes. The surface was then washed for 45 seconds with a physiologic solution.
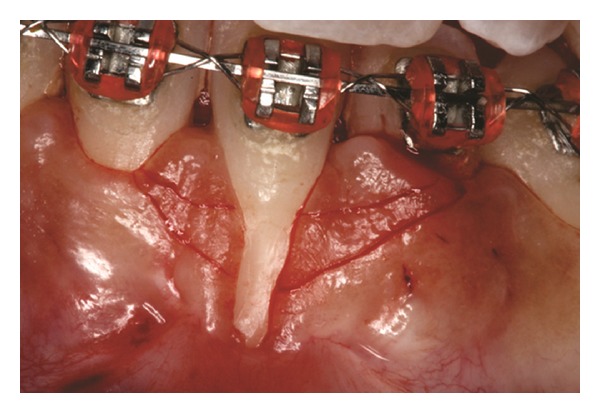
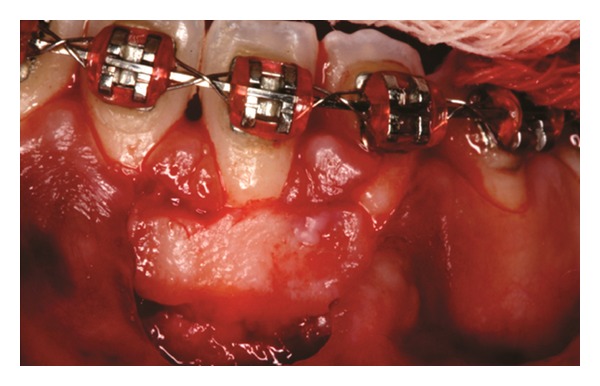
Both papillae adjacent to the recession were incised at buccal aspect. The first papillary incisions were horizontal at the level of the cementoenamel junction. The second papillary incisions were oblique and made at an apical level from those previously performed (Figures 2, 11 and 18). A third intrasulcular incision was performed to connect the papillary incisions. A partial thickness flap was performed from the second incision, allowing the removal of the gingival epithelium between the two incisions using Castroviejo scissors.
Figure 2.

First and second incisions.
Figure 11.
First and second incisions.
Figure 18.

First and second incisions.
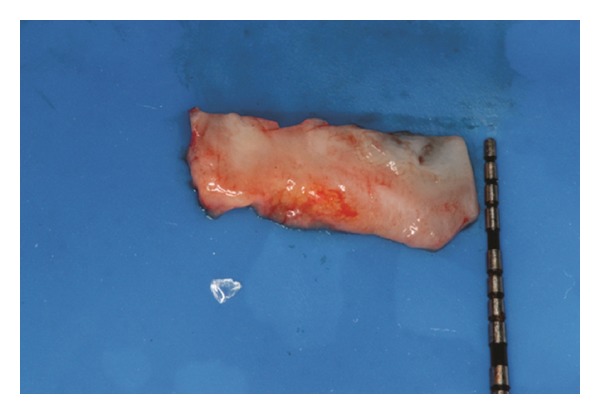
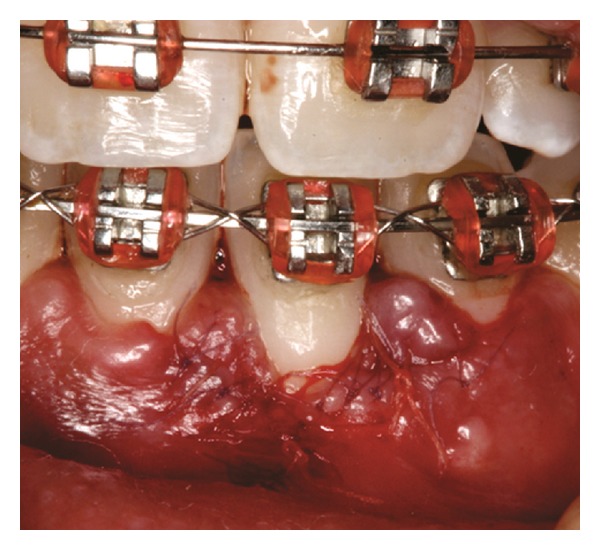
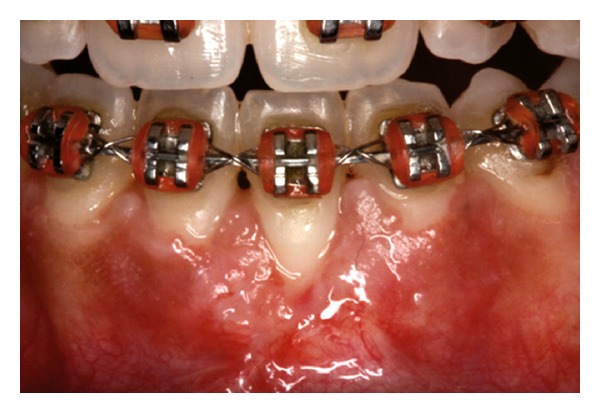
The recipient site was measured (Figure 3) using a periodontal probe and these measurements were transferred to the donor site. A palatal connective tissue graft was harvested from the area distal to the canine and anterior to the mesial aspect of the first molar on the same side of the surgery. The epithelium at the graft was removed (Figures 4 and 12). After stabilizing the graft in the correct position (Figures 5, 13, and 19) using 6-0 vicryl sutures, the microsutures for flap approximation and coaptation were performed using 6-0 and 8-0 vicryl sutures, respectively (Figures 6, 14, and 20). The palate was then sutured with a continuous basting suture using a 4-0 silk thread. A thin layer of periodontal dressing was applied at both surgical sites.
Figure 3.
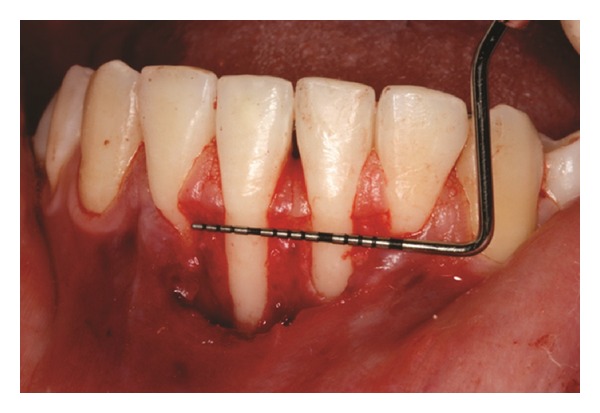
Measurement of recipient site after performing a partial thickness flap.
Figure 4.
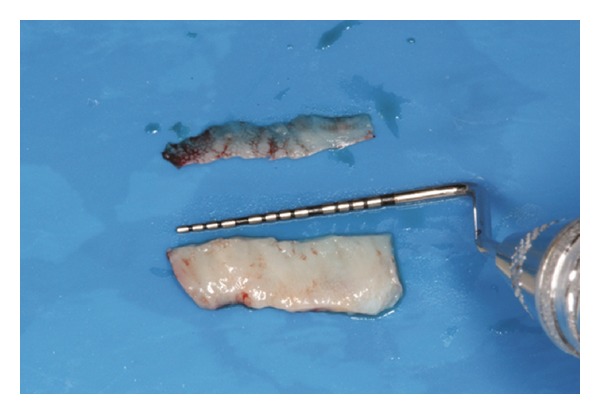
Connective tissue graft after the removal of the epithelium.
Figure 12.
Connective tissue graft after the removal of the epithelium.
Figure 5.

Graft stabilization at recipient site.
Figure 13.
Graft stabilization at recipient site.
Figure 19.

Graft stabilization at recipient site.
Figure 6.

Microsutures.
Figure 14.
Microsutures.
Figure 20.

Microsutures.
2.3. Postoperative Care
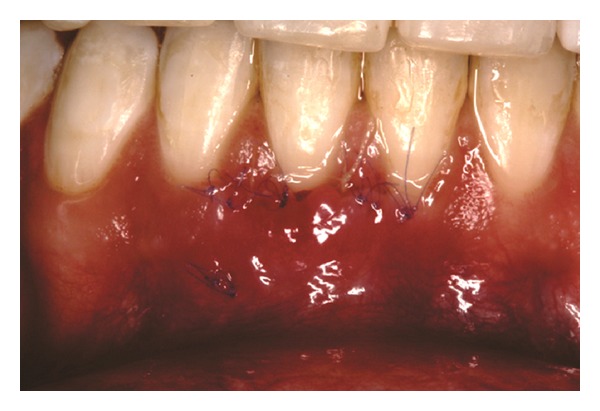
The patients were instructed to use Amoxicillin 500 mg t.i.d. for 7 days, Dexamethasone 4 mg b.i.d. in the first 24 hours and sodium dipyrone 1 g q.i.d. in the first 48 h. Furthermore, tooth brushing was discontinued around the surgical sites for three weeks and plaque control was provided by rinsing with a 0.12% chlorhexidine solution twice a day. After this period, the patients were instructed to use a unituft brush to clean the site. After 7 days, the periodontal dressing and sutures were removed (Figures 7, 8, and 15) and the patients were called for follow-up visits (Figures 9 and 16). During the follow-up visits, Patient 3 presented with incomplete root coverage after the initial surgical procedure. A second surgical procedure was performed to provide complete root coverage (Figures 21, 22, 23, and 24).
Figure 7.

Seven-day follow-up of recipient site.
Figure 8.

Seven-day follow-up of donor site.
Figure 15.

Seven-day follow-up of recipient site.
Figure 9.

Thirty-day follow-up.
Figure 16.
Thirty-day follow-up.
Figure 21.

Follow-up visit. Patient 3 presented incomplete root coverage.
Figure 22.

Second surgical procedure to achieve complete root coverage.
Figure 23.
Seven-day follow-up of recipient site.
Figure 24.
Thirty-day follow-up after the second intervention.
3. Discussion
Orthodontic movement is one of the important factors in the development of gingival recession. However, the scientific evidence related to this topic is scarce and controversial, since many studies use a limited sample and lack well-established evaluation criteria [11].
The results of several studies have demonstrated a higher prevalence and severity of gingival recession after orthodontic treatment. Nevertheless, some authors have observed that gingival recession related to orthodontic treatment affects a small portion of patients, and although there was an increase in severity, it did not result in severe clinical consequences [8, 10, 13].
It was observed that the proclination of incisors is related to the development of recession [11, 12]. However, Vasconcelos et al. [9] found that retroclination was also related to an increase in the severity of gingival recession. On the other hand, Djeu et al. [26] did not find a correlation between the proclination of mandibular central incisors and gingival recession.
With regards to gingival thickness, Yared et al. [12] observed that free gingival margins with a thickness <0.5 mm presented greater and more severe recession associated with mandibular central incisors. However, one study using a human sample found that the mean amount of initial keratinized gingiva did not predispose the mandibular incisors and canines to gingival recession [27]. An animal study found that central incisor sites submitted to gingival grafts showed less gingival recession and maintenance of gingival thickness after vestibular orthodontic movement [28].
Kao and Pasquinelli [24] classified the periodontal biotype as thin or thick. Thin biotypes present a thin underlying bone, characterized by bony dehiscence and fenestration, which reacts to insults and disease with gingival recession. The presence of a thin biotype was identified as a possible predictor of gingival recession in a study by Melsen and Allais [13]. The present study reported two cases, 1 and 3, which had thin biotypes, since a highly scalloped soft tissue and bony architecture and a minimal amount of attached gingiva were observed.
The surgical manipulation of thin gingival biotypes imposes some challenges for the surgeons, since there is a higher possibility of flap dilacerations and/or perforations, which can interfere in the final result of the surgical treatment. Thus, it is possible that the incorporation of microsurgical techniques using appropriate illumination and magnification for more precise flap elevation and sutures can lead to primary wound closure [21–23].
According to Miller's [25] classification, complete root coverage can be anticipated in Classes I and II, partial root coverage is expected in Class III and root coverage is not anticipated in Class IV. The presented cases were classified as Class II or III, and satisfactory root coverage was achieved in all cases. Patient 3 had a Miller Class II recession and was submitted to a second surgical procedure, since complete root coverage was not achieved with the first procedure and the gingival margin remained disharmonious. The reasons for this fact can be related to the initial recession depth as well as to the quality of the soft and hard tissue [18].
Within the limits of this study, a subepithelial connective tissue graft using a microsurgical approach resulted in successful root coverage and increased keratinized tissue, improving the gingival esthetic pattern in cases where deep gingival recession was associated with orthodontic movement.
Conflict of Interests
The authors declare that there is no conflict of interests regarding the publication of this paper.
Funding
This study was self-supported by the authors.
References
- 1.The American Academy of Periodontology. Glossary of Periodontal Terms. Chicago, Ill, USA: The American Academy of Periodontology; 2001. [Google Scholar]
- 2.Raetzke PB. Covering localized areas of root exposure employing the “envelope” technique. Journal of Periodontology. 1985;56(7):397–402. doi: 10.1902/jop.1985.56.7.397. [DOI] [PubMed] [Google Scholar]
- 3.Susin C, Haas AN, Oppermann RV, Haugejorden O, Albandar JM. Gingival recession: epidemiology and risk indicators in a representative urban Brazilian population. Journal of Periodontology. 2004;75(10):1377–1386. doi: 10.1902/jop.2004.75.10.1377. [DOI] [PubMed] [Google Scholar]
- 4.Löe H, Anerud A, Boysen H. The natural history of periodontal disease in man: prevalence, severity, and extent of gingival recession. Journal of Periodontology. 1992;63(6):489–495. doi: 10.1902/jop.1992.63.6.489. [DOI] [PubMed] [Google Scholar]
- 5.Borghetti A, Monnet-Corti V. Chirurgie Plastique Parodontale. Paris, France: Éditions CDP; 2000. [Google Scholar]
- 6.Rajapakse PS, McCracken GI, Gwynnett E, Steen ND, Guentsch A, Heasman PA. Does tooth brushing influence the development and progression of non-inflammatory gingival recession? A systematic review. Journal of Clinical Periodontology. 2007;34(12):1046–1061. doi: 10.1111/j.1600-051X.2007.01149.x. [DOI] [PubMed] [Google Scholar]
- 7.Sardella A, Pedrinazzi M, Bez C, Lodi G, Carrassi A. Labial piercing resulting in gingival recession. A case series. Journal of Clinical Periodontology. 2002;29(10):961–963. doi: 10.1034/j.1600-051x.2002.291012.x. [DOI] [PubMed] [Google Scholar]
- 8.Closs LQ, Grehs B, Raveli DB, Rösing CK. Occurrence, extension, and severity of gingival margin alterations after orthodontic treatment. World Journal of Orthodontics. 2008;9(3):e1–e6. [PubMed] [Google Scholar]
- 9.Vasconcelos G, Kjellsen K, Preus H, Vandevska-Radunovic V, Hansen BF. Prevalence and severity of vestibular recession in mandibular incisors after orthodontic treatment: a case-control retrospective study. The Angle Orthodontist. 2012;82(1):42–47. doi: 10.2319/021411-108.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Slutzkey S, Levin L. Gingival recession in young adults: occurrence, severity, and relationship to past orthodontic treatment and oral piercing. The American Journal of Orthodontics and Dentofacial Orthopedics. 2008;134(5):652–656. doi: 10.1016/j.ajodo.2007.02.054. [DOI] [PubMed] [Google Scholar]
- 11.Joss-Vassalli I, Grebenstein C, Topouzelis N, Sculean A, Katsaros C. Orthodontic therapy and gingival recession: a systematic review. Orthodontics & Craniofacial Research. 2010;13(3):127–141. doi: 10.1111/j.1601-6343.2010.01491.x. [DOI] [PubMed] [Google Scholar]
- 12.Yared KFG, Zenobio EG, Pacheco W. Periodontal status of mandibular central incisors after orthodontic proclination in adults. The American Journal of Orthodontics and Dentofacial Orthopedics. 2006;130(1):6.e1–8.e1. doi: 10.1016/j.ajodo.2006.01.015. [DOI] [PubMed] [Google Scholar]
- 13.Melsen B, Allais D. Factors of importance for the development of dehiscences during labial movement of mandibular incisors: a retrospective study of adult orthodontic patients. The American Journal of Orthodontics and Dentofacial Orthopedics. 2005;127(5):552–561. doi: 10.1016/j.ajodo.2003.12.026. [DOI] [PubMed] [Google Scholar]
- 14.Björn H. Free transplantation of gingiva propria. Swedish Dental Journal. 1963;22:684–689. [Google Scholar]
- 15.Grupe J, Warren R. Repair of gingival defects by a sliding flap operation. Journal of Periodontology. 1956;27(2):290–295. [Google Scholar]
- 16.Harris RJ. The connective tissue and partial thickness double pedicle graft: a predictable method of obtaining root coverage. Journal of Periodontology. 1992;63(5):477–486. doi: 10.1902/jop.1992.63.5.477. [DOI] [PubMed] [Google Scholar]
- 17.Langer B, Calagna LJ. The subepithelial connective tissue graft. A new approach to the enhancement of anterior cosmetics. The International Journal of Periodontics & Restorative Dentistry. 1982;2(2):22–33. [PubMed] [Google Scholar]
- 18.Chambrone L, Sukekava F, Araújo MG, Pustiglioni FE, Chambrone LA, Lima LA. Root-coverage procedures for the treatment of localized recession-type defects: a Cochrane systematic review. Journal of Periodontology. 2010;81(4):452–478. doi: 10.1902/jop.2010.090540. [DOI] [PubMed] [Google Scholar]
- 19.Oates TW, Robinson M, Gunsolley JC. Surgical therapies for the treatment of gingival recession. A systematic review. Annals of Periodontology. 2003;8(1):303–320. doi: 10.1902/annals.2003.8.1.303. [DOI] [PubMed] [Google Scholar]
- 20.Roccuzzo M, Bunino M, Needleman I, Sanz M. Periodontal plastic surgery for treatment of localized gingival recessions: a systematic review. Journal of Clinical Periodontology. 2002;29, supplement 3:178–194. doi: 10.1034/j.1600-051x.29.s3.11.x. [DOI] [PubMed] [Google Scholar]
- 21.Belcher JM. A perspective on periodontal microsurgery. The International Journal of Periodontics and Restorative Dentistry. 2001;21(2):191–196. [PubMed] [Google Scholar]
- 22.de Campos GV, Bittencourt S, Sallum AW, Nociti Júnior FH, Sallum EA, Casati MZ. Achieving primary closure and enhancing aesthetics with periodontal microsurgery. Practical Procedures & Aesthetic Dentistry. 2006;18(7):449–454. [PubMed] [Google Scholar]
- 23.Shanelec DA. Periodontal microsurgery. Journal of Esthetic and Restorative Dentistry. 2003;15(7):402–407. doi: 10.1111/j.1708-8240.2003.tb00965.x. [DOI] [PubMed] [Google Scholar]
- 24.Kao RT, Pasquinelli K. Thick vs. thin gingival tissue: a key determinant in tissue response to disease and restorative treatment. Journal of the California Dental Association. 2002;30(7):521–526. [PubMed] [Google Scholar]
- 25.Miller PD., Jr. A classification of marginal tissue recession. The International Journal of Periodontics & Restorative Dentistry. 1985;5(2):8–13. [PubMed] [Google Scholar]
- 26.Djeu G, Hayes C, Zawaideh S. Correlation between mandibular central incisor proclination and gingival recession during fixed appliance therapy. The Angle Orthodontist. 2002;72(3):238–245. doi: 10.1043/0003-3219(2002)072<0238:CBMCIP>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 27.Closs LQ, Branco P, Rizzatto SD, Raveli DB, Rösing CK. Gingival margin alterations and the pre-orthodontic treatment amount of keratinized gingiva. Brazilian Oral Research. 2007;21(1):58–63. doi: 10.1590/s1806-83242007000100010. [DOI] [PubMed] [Google Scholar]
- 28.Holmes HD, Tennant M, Goonewardene MS. Augmentation of faciolingual gingival dimensions with free connective tissue grafts before labial orthodontic tooth movement: an experimental study with a canine model. The American Journal of Orthodontics and Dentofacial Orthopedics. 2005;127(5):562–572. doi: 10.1016/j.ajodo.2004.04.023. [DOI] [PubMed] [Google Scholar]