

Abstract
Background: Effective team performance is essential in the delivery of high-quality health-care. Leadership skills therefore are an important part of physicians’ everyday clinical life. To date, the development of leadership skills are underrepresented in medical curricula. Appropriate training methods for equipping doctors with these leadership skills are highly desirable.
Objective: The review aims to summarize the findings in the current literature regarding training in leadership skills in medicine and tries to integrate the findings to guide future research and training development.
Method: The PubMED, ERIC, and PsycArticles, PsycINFO, PSYNDEX and Academic search complete of EBSCOhost were searched for training of leadership skills in medicine in German and English. Relevant articles were identified and findings were integrated and consolidated regarding the leadership principles, target group of training and number of participants, temporal resources of the training, training content and methods, the evaluation design and trainings effects.
Results: Eight studies met all inclusion criteria and no exclusion criteria. The range of training programs is very broad and leadership skill components are diverse. Training designs implied theoretical reflections of leadership phenomena as well as discussions of case studies from practice. The duration of training ranged from several hours to years. Reactions of participants to trainings were positive, yet no behavioral changes through training were examined.
Conclusions: More research is needed to understand the factors critical to success in the development of leadership skills in medical education and to adapt goal-oriented training methods. Requirements analysis might help to gain knowledge about the nature of leadership skills in medicine. The authors propose a stronger focus on behavioral training methods like simulation-based training for leadership skills in medical education.
Keywords: Education Medical (MeSH [I02.358.399]), Leadership (MeSH [F01.752.609]), training
Zusammenfassung
Hintergrund: Eine effektive Zusammenarbeit in Teams ist eine wichtige Voraussetzung für qualitativ hochwertige Versorgung im Gesundheitswesen. In diesem Zusammenhang spielen auch Führungskompetenzen von Ärztinnen und Ärzten im klinischen Alltag eine wichtige Rolle. Bisher wurde die Entwicklung von Führungskompetenzen in medizinischen Curricula in der Aus- und Weiterbildung von Ärztinnen und Ärzten jedoch kaum systematisch abgebildet. Die Entwicklung adäquater und effektiver Trainingsmethoden für die Vermittlung von Führungskompetenzen ist daher wünschenswert.
Ziel: Das Review soll vorliegende Ergebnisse der Literatur zu Trainings von Führungskompetenzen in der Medizin zusammenfassen und integrieren, um zukünftige Forschung und Trainingsentwicklung anzuregen.
Methode: Die Datenbanken PubMED, ERIC, PsycArticles, PsycINFO, PSYNDEX und dem Academic search complete durch EBSCOhost wurden auf Deutsch und Englisch nach Trainings von Führungskompetenzen in der Medizin durchsucht. Relevante Artikel wurden identifiziert und die Studienergebnisse hinsichtlich des zugrundeliegenden Führungsverständnisses, der Zielgruppe und Teilnehmeranzahl, der zeitlichen Ressourcen, sowie der Inhalte und Methoden des Trainings, des Evaluationsdesigns und der berichteten Trainingseffekte zusammengefasst.
Ergebnisse: Auf acht Studien trafen alle Einschluss- und kein Ausschlusskriterium zu. Die Trainings selbst sowie die thematisierten Führungskompetenzen differenzieren jedoch stark voneinander. Die Trainingsdesigns beinhalten im Schwerpunkt die theoretische Auseinandersetzung mit dem Thema Führung sowie die Diskussion von Fallstudien aus der Praxis. Die Dauer der Trainings reicht von mehrstündigen bis hin zu mehrjährigen Veranstaltungen. Die selbst eingeschätzte Reaktion der Teilnehmer auf alle Trainings war positiv; es fand jedoch bisher keine systematische Überprüfung des Trainingserfolgs in Bezug auf konkrete Verhaltensänderungen der Teilnehmer statt.
Schlussfolgerungen: Es bedarf weiterer Forschung, um die Erfolgsfaktoren für die Vermittlung von Führungskompetenzen in der medizinischen Aus- und Weiterbildung zu verstehen und die Trainingsmethoden gezielt anzupassen. Anforderungsanalysen könnten helfen, Führungskompetenzen in der Medizin besser zu erfassen. Weiterhin schlagen die Autoren vor, den Fokus zukünftig mehr auf verhaltensnahe Trainingsmethoden wie simulationsbasierte Trainings zu legen.
Authors
First two authors have contributed equally to this manuscript.
Background
"Nothing in a doctor’s medical education qualifies him to be a leader" - Larry L. Mathis [1].
Yet from their very first day at work, physicians* are expected to take on the role of a leader, to bear responsibility and to make important medical decisions facing a heterogenenous environment. As they do this, taking an active leadership role and implementing managerial behavior contribute to more effective teamwork and good patient care [2], [3]. In order to avoid conflicts and delays in operational procedure, it is indispensable to implement training sessions on effective leadership behavior adequate to diverse settings and targets [4], [5]. These findings show the need for young physicians to be introduced to their leadership roles in the context of their training, by targeted support for and development of leadership skills as part of the medical curriculum.
The concept of leadership here comprises exercising conscious, goal-oriented social influence on people for the purpose of performing shared tasks in pursuit of common goals, and focuses on leading subordinates, colleagues and teams [6], [7]. The active adoption of a leadership role and the associated implementation of leadership skills include (cf. Schmidt-Huber [8]; Frey, Peus & Weisweiler [9]):
formulating visions of the future together with tasks and goals
motivating and supporting staff members and colleagues
establishing trust and building up viable work relationships
organizing work activities
communicating confidence, developing participants (e.g. by giving feedback)
delegating responsibility
ensuring good quality of work and
managing change and conflict.
The relevance of specific requirements varies according to the degree of responsibility (e.g. for formulating visions), but also displays many things in common, even across hierarchies.
Despite the importance of systematic teaching of leadership skills in the undergraduate and continuing training of young doctors, its content is yet only taken into account in medical training to a limited extent. It is true that in the catalogue of learning objectives published worldwide, skills can be found that display parallels with leadership skills, but the latter are rarely tackled directly. A review of the extent to which leadership skills are embedded in the catalogues of learning objectives published worldwide is shown in Table 1 (Tab. 1). For the purpose of comparing the content of learning objective catalogues, the outlined conceptual definition of leadership – as intentional influence over other people to guide, structure, and facilitate activities and relationships in a group or organization– is employed.
Table 1. A review of the extent to which leadership skills are embedded in the catalogues of learning objectives published worldwide.

In the Canadian CanMeds Framework [10] and the Swiss Catalogue of Learning Objectives [11], leadership skills are described within the collaborator’s role as a physician. In the Dutch Framework, published in 2009, leadership skills are not explicitly taken to be part of the doctor's role. It may be surmised that leadership skills are included [12] in the above-mentioned definition in the physician's roles of collaborator and communicator. In the catalogue of learning objectives of Scotland's The Scottish Doctor, leadership skills are explicitly given as a subsidiary item in the collaboration of the doctor in the interdisciplinary health-care team. In the British catalogue of learning objectives Tomorrow’s Doctors, the importance of leadership skills in the doctor's actions, though absent in earlier versions of this catalogue of learning objectives, is mentioned in the present edition. As in Scotland, leadership skills are explicitly shown in the category of learning and working within the interdisciplinary team [13]. It must be stressed that in this publication, in the learning-objective category of leadership skills, following a leader of higher rank in the hierarchy is also mentioned. This is also done in the catalogue of learning objectives of the USA, Learning Objectives for Medical Student Education, though here it is embedded in the role of the conscientious doctor [14]. In the catalogue of learning objectives of the World Federation of Medical Education, leadership is described as an element in clinical knowledge and skills [15].
Despite the undisputed importance of training of leadership skills in medical curricula for professional collaboration as well as patient care, it is under-represented in the selected catalogues of learning objectives [1]. There is a correspondingly low number of findings as to how the development of leadership skills can be integrated into medical training and what effects the development measures can aim to attain.
In the scientific discourse of research into doctors' undergraduate and continuing education only a very limited number of publications and contributions draw attention to the fact that to date there has been very little integrated and conceptualized knowledge for the training of leadership skills. The authors aim to bridge this gap in this review paper.
Aims of the study
The central aim of the study was to analyze articles with empirical research that integrated the training of leadership skills in physicians’ undergraduate and continuing medical education. The work identified should reveal what components of leadership skills have been identified and trained. In addition, after analysis of the training methods, it should be possible to infer effective procedures and development measures that can be adduced as standards of reference for future training programs.
Method
The implementation of this review is in line with BEME Guide No. 13 [16], which describes clear guidelines for a systematic search strategy in medical and educational/psychological databases.
Data sources
Between April and September 2012, the two authors (ACK, JK) conducted a systematic literature search in the PubMed, ERIC and EBSCO HOST (databases: Academic search complete, PsycINFO, PsycArticles, PSYNDEX), with the following search terms, in the title, abstract and keywords: Training (training), Führungskompetenzen (leadership competency/competencies, skill/skills), Medizin (medicine). In addition, a systematic internet search for relevant scientific articles was undertaken. The search was conducted in publications written in German and English. Only those articles were included that focused on the training of leadership skills in medical studies and physicians' further training (in American studies, including those described as Interns and Residents).
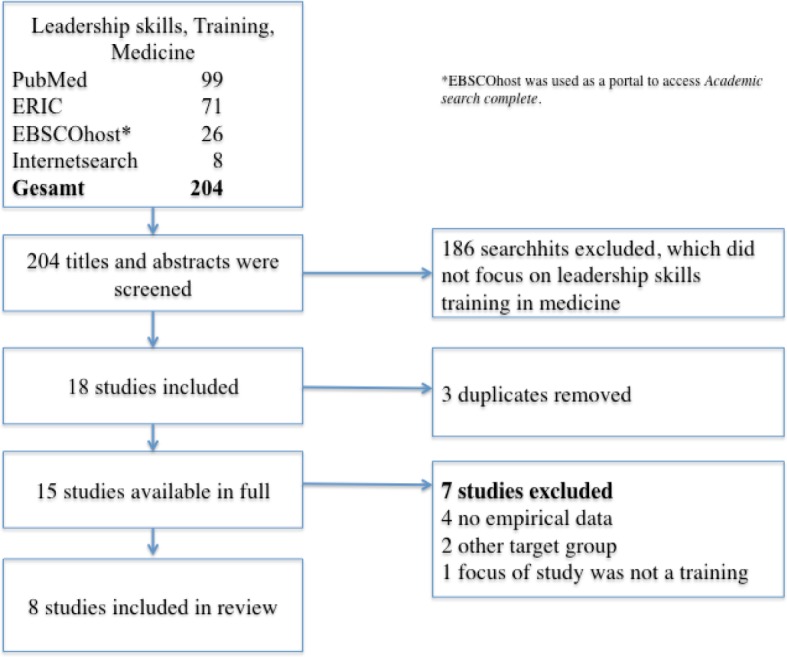
The articles researched (N=204) were examined by the two authors (JK and ACK) with respect to their titles, keywords and abstracts for the relevance of their themes. Only those studies were included that namely focused on the training of leadership skills in medicine and that interpreted leadership in the sense of guiding co-workers and not in the sense of guiding patients. Studies that were restricted to leadership scenarios with the focus solely on intensive and emergency care were excluded, as these relate to a specialized area of medical leadership. The specialization in which the leadership skills were developed was not relevant to inclusion in the study. Only empirical studies that reported the results of their training assessments were included. A summary of the system of inclusion and exclusion of studies is found in Figure 1 (Fig. 1). The preliminary selection on these criteria contained a total of 15 studies.
Figure 1. Summary of inclusion and exclusion of studies.
Data extraction
In the next stage of selection, text analysis was used to exclude all articles that reported no empirical data (N=4), that focused on a target group other than medical students, Interns and Residents (N=2) or in which the central focus of the study did not include an assessment of the training. After this exclusion step, eight studies were included in the further analysis (cf. Table 2 (Tab. 2))
Table 2. Summary of the studies included in the review.

Data analysis and results
The coding and content analysis of the studies included was oriented towards the aims of the article and, hence, related to the following criteria:
the basic understanding of leadership
the target group undergoing the training and number of participants
temporal resources of the training
training content and methods
evaluation design
reported effects of the training
Tab. 3 (see attachment ) gives an overview of the results, oriented according to the analysis criteria. In general, only studies from the USA, published between 1994 and 2011, met the criteria for inclusion. In the filtering process, it also became clear that the concept of leadership was very often understood in the sense of the hierarchical structure of an organization, and only rarely as direct leadership of staff or colleagues.
The leadership concept taken as a basis
Altogether, the studies contained widely differing concepts of leadership and leadership skills. Two studies contained no detailed descriptions of the leadership skills taught, but considered leadership skills embedded in a more general skill like the skill to teach [17] or the capacity for teamwork [18]. The majority of the studies focused individual aspects of leadership skills, such as feedback behavior [19], [20], [21], communication [21], [22], [23] or ability to deal with conflict [19], [20]. In addition, motivation and coaching [19], monitoring and self-management [21], knowledge of leadership styles, analysis of situations, decision making and problem solving [23], integrity and delegation [22], team management, dealing with different personalities and leading group discussions [24] were brought into focus for consideration distinct leadership skills.
In most of the articles included [17], [20], [22], [23], [24], the authors stressed the need to avoid training leadership skills in isolation from the specialized context and to take account explicitly of everyday clinical requirements and cooperation in the medical team (N=5).
Target group, participants and temporal resources
Most of the training programs were conducted for Interns and Residents [17], [18], [20], [22], [24] and students following combined PhD/MD programs19 (N=6). In only two studies was the training offered to medical students [18], [23] (see Tab. 3 in the attatchment ). The temporal resources allocated also varied widely, from sessions lasting three hours [8] or individual workshops in the framework of programs lasting several years6 to sessions taking several days [13].
Training content and methods
To implement the content of the training, for the most part, in addition to the theoretical content, interactive discussion groups were instituted. These either contained a generally moderated discussion of the principles and skills of leadership (N=4) [18], [21], [23], [24], or the observation of effective leadership behavior using a fictitious case from everyday clinical practice as an example (N=3) [17], [19], [20]. Role-play as training for real leadership behavior was found in three studies [17], [19], [24]. Three other studies [20], [21], [23] incorporated training in leadership and teaching skills in the context of preparation and implementation of a mini-teaching project related to actual practice. In individual cases, other methods such as lectures [19], mentoring and self-reflection [24] or team development measures [18] were employed. One study did not name any concrete approach to imparting the content of the training [22].
Assessment and effects of the training
Altogether, analysis of the assessment concept showed that strikingly diverse methods of assessment were employed. In four studies, assessment concepts were reported that included pre- and post-training evaluations [8], [9], [10], [12], in three articles post-training tests alone were used [7], [11], [13] and one study gave no data regarding the assessment concept [6]. In all the studies, the only data recorded consisted of the participants' self-assessments obtained by means of a questionnaire.
Essentially, all the studies reported positive participant reactions to the training concerned (e.g. satisfaction [7], positive evaluation of the quality of the training [13]). Furthermore, two studies included the effectiveness in everyday clinical practice of the content imparted as perceived several months after the training took place. Here the participants reported a detectable long-term effect of the training [20], [23]. In addition, one study described increased self-confidence in the participants subsequent to the training (self-assessment report by the participants) [24]. Similarly, one study [22], using a validated questionnaire, observed an improvement in values relating to communication, integrity and the capacity to give orders.
Discussion
Regarding the importance of appropriate leadership behavior in everyday clinical practice, the systematic training of leadership skills should be integrated into medical training curricula. This study aimed at analyzing prior findings concerning the development of leadership skills in medical training, and a comparison of the content of training programs and the methods employed. Thus, an understanding of the implementation of effective training methods to strengthen leadership skills in physicians' undergraduate and continuing medical education should be obtained.
The small number of studies included in the review shows that the systematic and evidence-based development of leadership skills does not currently play a prominent role in the training of physicians. Considering the content of the medical curriculum for training physicians in Germany shows that this is particularly true in physicians' undergraduate medical education. In the pre-final version to be found in the national skill-based catalogue of learning objectives in medicine (NLKM), training in leadership skills has not been mentioned up to now. This impression is confirmed by the lack of studies into the assessment of leadership training studies in the German-speaking countries.
The diverse concepts underlying leadership skills in medical training also show little agreement as to what content should be emphasized in the development of leadership skills, especially in the first stage of training. The results reveal a clear need for verified findings relating to the content for developing leadership skills, especially in physicians' undergraduate and early continuing medical education. For this purpose, there is a primary need for a structured analysis of requirements, involving the various persons involved in everyday clinical practice (e.g. medical practitioners, both with and without leadership responsibilities, care staff, medical students and other participants: vgl. Dieckmann [25]).
In the analysis of training content, a focus on the imparting of theoretical content is also noticeable. Only in three of the analyzed studies theoretical trainings were complemented by role play or experimental learning. This holds the question of whether, on the contrary, a focus on role-play and simulations with intensive feedback, backed up by specialized and interdisciplinary aspects of the knowledge, might not lead to more lasting implementation in practice. Findings in the literature on simulation-based training [3], e.g. for developing effective teamwork [5], makes a strong point for the effectiveness of these interactive training methods. This can be successful, for example, in the form of simulation-based training modules that contain leadership situations from everyday clinical practice that are critical for success and that can be effected with the assistance of professional role-play partners and video feedback. In this way, the individual behavioral repertoires of the participants can be improved systematically.
Furthermore, none of the studies included any detailed examination of the requirements of trainers in order for them to be able to give training in leadership skills. Because of the necessary specialist knowledge and background experience, it is questionable to what extent specialist medical staff is sufficiently qualified to train leadership skills unless backed by an expert in matters of leadership. For example, targeted cooperation with professional trainers could be a solution for effective training. Alternatively, train-the-trainer seminars for leadership skills could be embedded in postgraduate medical further training courses, such as the Master of Medical Education.
Positive effects of trainings were reported in all the studies. However, all the effects were evaluated as simple self-assessments on the part of the participants. On the other hand, the criteria of success recorded represent the simplest evaluation step in Kirkpatrick’s established evaluation model [26] (Step 1: Reaction of participants; Step 2: Learning effects; Step 3: Changes in behavior and Step 4: Organizational effects). Only two of the included studies used validated questionnaires [22] or knowledge tests [20] to assess the learning and transfer effects in addition to the self-reported satisfactory reactions of the participants. Yet the focus was not on concrete leadership behavior, but on the self-confidence and self-efficacy of the participants. Thus the results show a clear need for intervention studies on the effects of training on leadership skills. These should assess both the pre- and post-training performance of the participants and also their motivation and the transfer of content to everyday clinical practice. Evaluations should further contain antecedents for the effects aimed at, such as how closely the training reflects reality, or the utility of the content. This can be achieved by qualitative methods, such as participants' diaries between individual sessions or longitudinal control group concepts.
The limitations of this review paper
Certain limitations of this review paper should be taken into consideration in interpreting the results. First, the search criteria considered precisely those studies that focus on the development of leadership skills in medicine. The research concentrated on published articles. Thus, the possibility remains that isolated studies of equivalent relevance, now appearing or recently published, may have been excluded. The small number of studies included limits the generalizability of this review paper. Also, although both German and English search terms were employed, only studies from the USA could be included. This poses the question of how far the results of evaluated programs would have been similarly successful in Germany.
Conclusions
The results of the study indicate that the development of leadership skills at present clearly does not constitute a central element of content in research into physicians' undergraduate and continuing medical education in Europe and the USA. This is apparent not only in the small number of published training studies, but also on the sole basis of the programs published in the USA.
For a clear outline of which leadership skills a physician needs a requirement analyses should be conducted at different hierarchical levels and with all those involved in day-to-day clinical practice. The authors hope that this review paper will stimulate research regarding the effectiveness and relevance to success of leadership skills in everyday clinical practice. In this context, investigations should also examine what specific aspects of leadership skills should be taken up in medical training and how these can be effectively imparted. Further, more effort should be devoted to integrating training in leadership skills as an established component in medical training. Training in leadership skills and the transmission of positive role models provide an opportunity to prepare prospective physicians specifically for their future leadership roles and responsibilities, since awareness of the importance of ethical, well thought-out leadership behavior will be enhanced, and the construction of an effective behavioral repertoire supported.
Further, the results of the studies indicate that more research is needed into the effects of training leadership skills in medical education. Up to now, in particular, case reviews and discussions of general principles of leadership and the associated consideration of one's own role seem to have led to positive reactions by participants. However, whether leadership behavior can be learned in medical education and then transferred and applied in practice is a question that cannot be fully grasped through the studies included in this paper, and will need to be approached in future studies.
Note
* In the interests of improved legibility and, consequently, clarity, it was decided that only the generalizing masculine form would be used. However, both sexes are expressly addressed throughout.
Competing interests
The authors declare that they have no competing interests.
Supplementary Material
References
- 1.Mathis LL. The Mathis maxims: lessons in leadership. Lakeland/FL: Leadership Press; 2001. [Google Scholar]
- 2.Boyle DK, Kochinda C. Enhancing collaborative communication of nurse and physician leadership in two intensive care units. J Nurs Admin. 2004;34:60–70. doi: 10.1097/00005110-200402000-00003. Available from: http://dx.doi.org/10.1097/00005110-200402000-00003. [DOI] [PubMed] [Google Scholar]
- 3.McGaghie WC, Issenberg SB, Petrusa ER, Scalese RJ. A critical review of simulation-based medical education research: 2003–2009. Med Educ. 2009;44(1):50–63. doi: 10.1111/j.1365-2923.2009.03547.x. Available from: http://dx.doi.org/10.1111/j.1365-2923.2009.03547.x. [DOI] [PubMed] [Google Scholar]
- 4.Pizzi L, Goldfarb NI, Nash DB. Crew resource management and its applications in medicine. In: Henriksen K, Battles JB, Marks ES, Lewin DI, editors. Advances in Patient Safety: From Research to Implementation (Volume 4: Programs, Tools, and Products. Rockville (MD): Agency for Healthcare Research and Quality (US); 2005. pp. 511–519. Available from: http://www.ncbi.nlm.nih.gov/books/NBK20594/ [PubMed] [Google Scholar]
- 5.Chakraborti C, Boonyasai RT, Wright SM, Kern DE. A systematic review of teamwork training interventions in medical student and resident education. J Gen Intern Med. 2008;23(6):846–853. doi: 10.1007/s11606-008-0600-6. Available from: http://dx.doi.org/10.1007/s11606-008-0600-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rosenstiel L. Leadership und Change. In: Bruch H, Krummaker S, Vogel B, editors. Leadership—Best Practices und Trends. Heidelberg: Springer; 2006. pp. 145–156. [Google Scholar]
- 7.Yukl G, Gordon A, Taber T. A hierarchical taxonomy of leadership behavior: Integrating a half century of behavior research. J Leadership Organ Stud. 2002;9:15–32. doi: 10.1177/107179190200900102. Available from: http://dx.doi.org/10.1177/107179190200900102. [DOI] [Google Scholar]
- 8.Schmidt-Huber M. Die Entwicklung und Validierung eines Kompetenzmodells und Instruments zur Erfassung von effektivem Führungsverhalten. Bielefeld: Universität Bielefeld; 2011. [Google Scholar]
- 9.Frey D, Peus C, Weisweiler S. Ethikorientierte Führung als wertstiftendes Human Capital Management. In: Friederichs P, Armutat S, editors. Der Human Capital Auditor Schlüsselfunktion im modernen Personalmanagement. Bielefeld: Bertelsmann Verlag; 2012. [Google Scholar]
- 10.Frank JR. The CanMEDS 2005 Physician Competency Framework. Ottawa: The Royal College of Physicians and Surgeons of Canada; 2005. Available from: http://www.royalcollege.ca/portal/page/portal/rc/common/documents/canmeds/resources/publications/framework_full_e.pdf. [Google Scholar]
- 11.Bürgi H, Rindlisbacher B, Bader C, Bloch R, Bosman F, Gasser C, Gerke W, Humair JP, Im Hof V, Kaiser H, Lefebvre D, Schläppi P, Sottas B, Spinas GA, Stuck AE. Swiss Catalogue of Learning Objectives for Undergraduate Medical Training. Bern: University of Bern; 2008. Available from: http://sclo.smifk.ch/downloads/sclo_2008.pdf. [Google Scholar]
- 12.van Herwaarden CL, Laan FJ, Leunissen RR. The 2009 Framework for Undergraduate Medical Education in the Netherlands. Utrecht: Dutch Federation of University Medical Centres; 2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.General Medical Council. Tomorrow's Doctors - Outcomes and standards for undergraduate medical education. London: General Medical Council; 2009. Available from: http://www.gmc-uk.org/TomorrowsDoctors_2009.pdf_39260971.pdf. [Google Scholar]
- 14.No authors listed. Learning objectives for medical student education-guidelines for medical schools: Report I of the Medical School Objectives Project. Acad Med. 1999;74(1):13. doi: 10.1097/00001888-199901000-00010. [DOI] [PubMed] [Google Scholar]
- 15.World Federation for Medical Education. Basic Medical Education - WFME Global Standards for Quality Improvement. Copenhagen: WFME Office, University of Copenhagen; 2012. [Google Scholar]
- 16.Hammick M, Dornan T, Steinert Y. Conducting a best evidence systematic review. Part 1: From idea to data coding. BEME Guide No. 13. Med Teach. 2010;32(1):3–15. doi: 10.3109/01421590903414245. Available from: http://dx.doi.org/10.3109/01421590903414245. [DOI] [PubMed] [Google Scholar]
- 17.Wipf JE, Pinsky LE, Burke W. Turning interns into senior residents: preparing residents for their teaching and leadership roles. Acad Med. 1995;70(7):591–596. doi: 10.1097/00001888-199507000-00010. Available from: http://dx.doi.org/10.1097/00001888-199507000-00010. [DOI] [PubMed] [Google Scholar]
- 18.Stoller JK, Rose M, Lee R, Dolgan C, Hoogwerf BJ. Teambuilding and leadership training in an internal medicine residency training program. J Gen Intern Med. 2004;19(6):692–697. doi: 10.1111/j.1525-1497.2004.30247.x. Available from: http://dx.doi.org/10.1111/j.1525-1497.2004.30247.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ciampa EJ, Hunt AA, Arneson KO, Mordes DA, Oldham WM, Vin WooK, Owens DA, Cannon MD, Dermody TS. A workshop on leadership for MD/PhD students. Med Educ Online. 2011;16 doi: 10.3402/meo.v16i0.7075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Levine SA, Chao SH, Brett B, Jackson AH, Burrows AB, Goldman LN, Caruso LB. Chief Resident Immersion Training in the Care of Older Adults: An Innovative Interspecialty Education and Leadership Intervention. J Am Geriatr Soc. 2008;56(6):1140–1145. doi: 10.1111/j.1532-5415.2008.01710.x. Available from: http://dx.doi.org/10.1111/j.1532-5415.2008.01710.x. [DOI] [PubMed] [Google Scholar]
- 21.Smith KL, Petersen DJ, Soriano R, Friedman E, Bensinger LD. Training tomorrow's teachers today: a national medical student teaching and leadership retreat. Med Teach. 2007;29(4):328–334. doi: 10.1080/01421590701316530. Available from: http://dx.doi.org/10.1080/01421590701316530. [DOI] [PubMed] [Google Scholar]
- 22.Awad SS, Hayley B, Fagan SP, Berger DH, Brunicardi FC. The impact of a novel resident leadership training curriculum. Am J Surg. 2004;188(5):481–484. doi: 10.1016/j.amjsurg.2004.07.024. Available from: http://dx.doi.org/10.1016/j.amjsurg.2004.07.024. [DOI] [PubMed] [Google Scholar]
- 23.Devaul RA, Knight JA, Edwards KA. Leadership training in medical education. Med Teach. 1994;16(1):47–51. doi: 10.3109/01421599409108257. Available from: http://dx.doi.org/10.3109/01421599409108257. [DOI] [Google Scholar]
- 24.Lee MT, Tse AM, Naguwa GS. Building leadership skills in paediatric residents. Med Educ. 2004;38(5):559–560. doi: 10.1111/j.1365-2929.2004.01867.x. Available from: http://dx.doi.org/10.1111/j.1365-2929.2004.01867.x. [DOI] [PubMed] [Google Scholar]
- 25.Dieckmann P. Using simulations for education, training and research. Oberhaching-München: Dustri-Verlag; 2009. [Google Scholar]
- 26.Kirkpatrick DL. Evaluating training programs. Noida: Tata McGraw-Hill Education; 1975. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.