

Abstract
This paper reports on the development and psychometric properties of the Adolescent Sexual Expectancies Scale (ASEXS). Data were obtained from three annual longitudinal surveys of youth aged 10 – 17 at the first administration (N = 932 at Wave 3). Confirmatory factor analyses indicated that four correlated factors corresponding to Social Risk, Social Benefit, Health Risk, and Pleasure adequately represented the expectancy items. High alpha coefficients and stability across survey waves indicated good internal and test-retest reliability for these factors. Latent variable autoregressive analyses indicated that Social Risk expectancies predicted changes in sexual behavior over the course of the study. Multi-group analyses established that the measurement and predictive models were equivalent for males and females and across age groups. The ASEXS provides researchers with a useful measure for examining adolescents’ expectancy beliefs about the consequences of sexual behavior.
Expectancies are beliefs about the likelihood that engaging in a behavior will lead to specific personal consequences (Olson, Roese, & Zanna, 1996). That is, they are subjective representations of anticipated rewards and punishments associated with that behavior. Expectancies are central concepts in many contemporary social-psychological theories (e.g., Ajzen, 2001; Bandura, 1986). A basic assumption of these theories is that individuals act in ways they believe will maximize positive outcomes and minimize negative outcomes. Expectancies are thus guides to future behavior and may affect how an individual attends to and interprets information, responds to and interacts with others, and selects and interprets social and environmental contexts (e.g., Olson, et al., 1996). Importantly, expectancies are malleable beliefs. They are acquired and modified through experience, communication from others, or observation. Expectancy beliefs may also derive from other logically related beliefs a person holds (e.g., Olson, Roese, & Zanna, 1996). For example, having unfavorable normative beliefs about having sex (e.g., my parents would disapprove) may affect expectancy beliefs regarding the likelihood of social consequences (e.g., getting into trouble). Expectancies not only help explain and predict behaviors, but may be an important focus for interventions designed to prevent or reduce problem behaviors or encourage healthy behaviors (Kamb, et al., 1998; Rhodes, et al., 2007).
Expectancy beliefs have received considerable attention as predictors of an array of health-related behaviors among adolescents, including alcohol use (Chen, Grube, & Madden, 1994; Goldman, et al., 1999; Leigh & Stacy, 2004; Grube & Agostinelli, 1999), drug use (Aarons, Brown, Stice, & Coe, 2001; Vangsness, Bry, & LaBouvie, 2005), and smoking (Lewis-Esquerre, Rodrigue, & Kahler, 2005; Wahl, Turner, Mermelstein, & Flay, 2005). Expectancy measures are less well developed in the area of adolescent sexuality. Some studies have included scales or individual items relating to expectancies (e.g., perceived risks, perceived benefits of sex) as correlates of adolescents’ sexual behaviors (e.g., Martino, et al., 2005; O’Donnell, O’Donnell, et al., 2003; Ott, Millstein, Ofner, & Halpern-Felsher, 2006; Small, Silverberg, & Kerns, 1993; Widdice, Cornell, Liang, & Halpern-Felsher, 2006) and condom and contraception use (Gebhardt, Kuyper, & Greunsven, 2003; Gilmore, et al., 1994; Sieving, et al., 2007; Widdice, et al., 2006). Research focusing on developing standardized and comprehensive measures of sexual expectancies, however, is rare.
Sexual expectancy research
A cross-sectional study of rural youth from Wisconsin indicated that the perceived costs and benefits of sex differentiated between sexually active and sexually non-active youth (Small, Silverberg, & Kerns, 1993). The measures for this study comprised 10 items representing two scales: positive and negative consequences (αs > .87). Consistent with expectancy theories, it was found that sexually active youth perceived greater benefits and fewer costs for having sex. Interestingly, perceived benefits were negatively correlated with age among sexually active youth, but were not related to age among sexually non-active youth. Conversely, perceived costs were negatively correlated with age for sexually non-active youth, but not significantly correlated with age among youth who were sexually active. Overall, females perceived fewer benefits and more costs associated with sex then did males.
The Cognitive Appraisal of Risky Events (CARE) scale (Fromme, Katz, & Rivet, 1997; Katz, Fromme, D’Amico, 2000) targets a range of behavioral domains including illicit drug use, aggressive and illegal behaviors, risky sexual activities, heavy drinking, high risk sports, and academic/work behaviors. Unlike most expectancy measures, however, this instrument does not measure the perceived likelihood of experiencing specific consequences. Rather, it presents respondents with a list of behaviors within each domain (e.g., leaving a social event with someone I just met; sex without protection against pregnancy, sex without protection from sexually transmitted diseases) and asks them to rate how likely it is that each behavior will generally result in costs and benefits and how likely they are to engage in that behavior (expected involvement). As a result, the CARE provides global measures of perceived benefits and costs, but does not take into account the possibility that beliefs about costs or benefits may be multidimensional. While the CARE has been shown to be highly reliable, the costs and benefits scales only modestly predicted sexual behaviors once past sexual experience is taken into account (Fromme, et al., 1997; Katz, et al., 2000).
More recently, the perceived risks of oral and vaginal sex were investigated by presenting adolescents with sexual scenarios, asking them to imagine themselves in each situation, and to rate each according to the likelihood (0% – 100%) that it would result in 12 positive (e.g., experience pleasure) and negative (e.g., become pregnant) consequences (Halpern-Felsher, Cornell, Kropp, & Tschann, 2005). The results indicated that, overall, oral sex was perceived as less risky, but also less pleasurable than vaginal sex. This study, however, was focused on differences in beliefs about oral and vaginal sex and did not investigate these expectancies as predictors of sexual behavior or changes in sexual behavior nor did it explore the dimensionality of sexual expectancies or the psychometric properties of these measures.
Another recent study (Guilamo-Ramos, et al., 2007) asked 6th, 7th, and 8th grade inner city students to rate the likelihood of outcomes related to having sex such as interfering with school, getting a bad reputation, or satisfying curiosity. These sex expectancy items were found to differ by gender, correlate with sexual experience, and to predict adolescents’ reports of parental sexual communication. While this work contributes to a more nuanced understanding of sexual expectancies, it also has several important limitations. First, the study was cross-sectional and did not explore the predictive ability of expectancies for sexual behavior nor did it investigate impact of sexual experience on later sexual expectancies. Second, dimensions underlying the items were not explored. Rather, each item was considered separately.
Expectancy beliefs must be considered in the context of other factors. Some theorists (e.g., Goldman, et al., 1999) propose that expectancies are a primary mediator of social and environmental influences on behavior. Thus, media, peers, and family, for example, are assumed to affect behavior because they affect young people’s expectancy beliefs. More comprehensive theories (e.g., Ajzen, 2001; Bandura, 1986) recognize that expectancies are one of many influences. From this perspective, sexual expectancies should be related to, but have effects on behavior that are independent of other influences such parental disapproval of or peer involvement in sexual behavior and sexual efficacy beliefs (perceptions of one’s ability to perform a sexually-related behavior). Motivations or reasons for having sex are closely related to, although not identical with, sexual expectancies. The desire for pleasure as a reason for engaging in sex, for example, implies an expectation that sex is likely to lead to pleasure. Research has suggested that adolescents’ motivations for sex include intimacy, coping, affirmation, partner approval, peer approval, and physical and emotional enhancement (Cooper, Shapiro, & Powers, 1998). Importantly, this research showed that these motivational dimensions were invariant regardless of sex, age, and sexual experience. Males, however, were more likely to endorse all motivations for sex except intimacy, which did not differ by gender. Age was positively related to intimacy motives and negatively related to partner and peer approval motives. These motives showed complex relations with sexual behaviors. Enhancement motives, for example, were negatively related to age of first consensual sex, but positively related to lifetime frequency, number of partners, risky behaviors, unplanned pregnancies, and sexually transmitted infections (STIs). In contrast, intimacy motives were positively related to lifetime frequency of sex, but negatively related to number of partners and risky behaviors. Such relations were observed both cross-sectionally and longitudinally (Cooper, Shapiro, & Powers, 1998).
Overall, the available research suggests that sexual expectancies may be important for understanding adolescents’ sexual behaviors. Few, if any, studies, however, have focused on developing comprehensive measures of adolescents’ sexual expectancies or have thoroughly investigated psychometric properties of such measures. The present paper reports on the development and validation of a measure of adolescents’ sexual expectancies, the Adolescent Sexual Expectancy Scale (ASEXS). Confirmatory factor analyses of three annual waves of data from a large longitudinal survey of youth were used to investigate the factor structure underlying the items in the ASEXS. Latent variable autoregressive structural equation modeling (LVSEM) was then used to investigate the stability of adolescents’ sexual expectancies over time, the relationships among the dimensions of sexual expectancies, and their relationship with sexual behaviors. Multi-group analyses were used to investigate the equivalence of the models for males and females and by age group. The overall goal was to develop a reliable and valid measure of sexual expectancies for adolescents that can be used in research and applied settings.
Method
Sample and Procedures
Participants
Data were obtained through a three-wave longitudinal study conducted annually in the San Francisco Bay Area and Los Angeles County, California. The sample was nearly evenly divided between females (48.2%) and males (51.8%), and consisted of 11.7% Latino, 6.6% African American, 7.1% Asian American (including Native Hawaiian and Pacific Islander), 3.7% American Indian or Alaskan Native, and 70.9% European American (White). Participants’ ages ranged from 10 to 17 at Wave 1 (M = 14.1). At Wave 1, 10.9% reported having engaged in oral sex, 8.0% vaginal intercourse, and 2.0% anal sex. The corresponding prevalence rates at Wave 2 were 21.4% for oral sex, 14.9% for vaginal intercourse, and 3.3% for anal sex. At Wave 3, these rates increased to 31.1% for oral sex, 24.3% for vaginal intercourse, and 6.3% for anal sex. Data from the 2001 California Health Interview Survey (CHIS, 2005) reported similar prevalence rates of sexual intercourse (25.7% of 15–17 year olds) as those we found for our third wave data (26.9% of 15–17 year olds), suggesting that our data are consistent with those of other recent state studies.
Sampling
A list-assisted sample of households from the greater San Francisco Bay Area (Alameda, Contra Costa, Marin, Napa, San Francisco, San Mateo, Santa Clara, Solano, and Sonoma counties) and Los Angeles County in California was used to recruit study participants. Specifically, households were sampled from a purchased list that consisted of households identified as likely to contain respondents in the target age range. Household composition, howver, could not be definitely determined until contact was made. The use of multiple listed samples from credit card, utility companies, magazine subscription lists, and other sources, screened for overlap, increases efficiency and coverage, substantially reduces costs, while at the same time producing samples comparable to those obtained through other less efficient techniques (Brick, Waksberg, Kulp, & Starer, 1995; Tucker, et al., 2002).
Data collection took place over three-month periods from September 2002 through November 2002 (Wave 1), September 2003 through November 2003 (Wave 2), and October 2004 through February 2005 (Wave 3) using Computer Assisted Self Interviews (CASIs) administered in the home. The CASI methodology has advantages over other survey techniques. It allows more sophisticated branching procedures making the interview process more efficient and increasing data quality. The branching capabilities also allow younger or sexually inexperienced respondents to skip over questions that are inappropriate for their age level and experience. Because the respondent interacts directly with a computer, without mediation through an interviewer, greater confidentiality can be assured, potentially improving the validity of self-reports of sensitive behaviors (Turner, Ku, Rogers, Lindberg, Pleck, & Sonenstein, 1998; Romer, et al., 1997). Recent research suggests that adolescent respondents are more likely to report risky behavior when they are interviewed with either web or computer-based CASI procedures than with a paper and pencil questionnaire or direct interviews, particularly for more sensitive attitudes and behaviors (Newman, Des Jarlais, Turner, Gribble, Cooley, & Paone, 2002; Turner et al., 1998).
Survey procedures
Potential participants and their parents were first contacted through a mailed letter and fact sheet that described the study and invited them to take part. A follow-up telephone call was used to schedule interviews. Up to 10 telephone contact attempts were made before a number was retired from the sample. Once telephone contact was made with a household a brief enumeration was conducted to ensure eligibility (e.g., presence of a youth in the target age range; located in the targeted geographical areas). If a household included more than one eligible individual, the youth with the most recent birthday was selected. At each in-home session, a trained interviewer explained the purpose of the survey to youth participants, showed them how to proceed through the computer program, and then left them in a private location to complete it. Parents were given a self-administered questionnaire to complete in another room to further ensure privacy for the youth respondents. The youth surveys averaged 25 to 35 minutes to complete. Active parental consent was obtained for all respondents and adolescents were given a $30 incentive for participating in each survey wave.
Response rates
Altogether, 1,105 youth respondents completed the Wave 1 survey. The estimated response rate was 75% using the CASRO method to distribute non-contacted telephone numbers were distributed between eligible and ineligible in the same proportions as for the numbers that were contacted (CASRO, 1982). This approach is conservative because it is likely that a greater proportion of the non-contacted numbers are ineligible (e.g., not working numbers). The cooperation rate (N completed interviews/N known eligible numbers) was considerably higher (88%). The completion rate was 92% (N = 1,012) at Wave 2 and 92% (N = 932) at Wave 3.
Measures
Sex expectancies
Expectancy items were initially created based on a review of previous studies. The sex expectancy scale at Wave 1 included 14 items. Using the stem “In your opinion, how likely or unlikely is it that each of the following things would happen to you personally if you were to have sexual intercourse? (If you’ve never had sexual intercourse, please try to imagine and make your best guess.)” The items were presented on a four-point scale (“very unlikely”, “somewhat unlikely”, “somewhat likely”, and “very likely”). The original 14 items included 1) get pregnant or get someone pregnant, 2) enjoy it, 3) get a sexually transmitted disease, 4) feel guilty, 5) be more popular, 6) get into trouble with your parents, 7) get a bad reputation, 8) feel more loved and wanted, 9) lose your self-respect, 10) feel more attractive, 11) keep your boyfriend or girlfriend from breaking up with you, 12) feel closer to your partner, 13) fit in more with your friends, and 14) disappoint people who are important to you. Preliminary analysis suggested that “fit in more with your friends” overlapped with measures of peer norms and this item was dropped from subsequent waves. At Wave 2, four items were added: get HIV/AIDS, feel happy, have fun, and feel more grown up. Between Waves 2 and 3, we elaborated “feel happy” to capture other more specific elements of pleasure-related expectancies: feel excited, feel satisfied, and feel pleasure.
Sexual behavior
Items measuring sexual behavior used progressive questioning, from going out alone with a boy/girl, holding hands, kissing or making out, through oral, vaginal and anal sex. In the current analysis, sexual activity was measured using three questions asking frequency of ever engaging in oral, vaginal, and anal sex (lifetime questions at each wave).
Background and demographic variables
Background variables included gender (male/female), age, race, and ethnicity (Latino/Hispanic). Because most of the racial groups contained too few respondents for meaningful analyses, race was coded as a single dummy variable (1 = White). These background variables were included in the models, where appropriate, as controls.
Missing data
Analysis of missing data among expectancy questions revealed items missing at random among those who had responded in each wave. The EM (expectation-maximization) estimation procedure in SPSS 14.0 for Windows was used to impute values for participants who were missing on individual items and who did not have structurally missing data.
Results
Confirmatory Factor analyses
Sexual expectancies
Preliminary analysis suggested that four-correlated factors reasonably captured the structure of the expectancy items. The four factors corresponded to Social Risk, Social Benefit, Health Risk, and Pleasure expectancies.1 Based on these results, the four-factor solution was imposed on each of the waves in confirmatory factor analyses using EQS 6.1 (Bentler, 1995). The four-factor structure was found to provide a good fit to the items at Wave 1, χ2 (66, N = 932) = 161.7, p < .001, NFI = .96, CFI = .97, RMSEA = .04, Wave 2 χ2 (107, N = 932) = 329.1, p < .001, NFI = .96, CFI = .97, RMSEA = .05, and Wave 3 χ2 (138, N = 932) = 395.2, p < .001, NFI = .95, CFI = .97, RMSEA = .05. One item (“How likely or unlikely is it that you would feel closer to your partner?”) significantly and consistently cross-loaded on both the Pleasure and Social Benefit factors.
Sexual behaviors
Additional confirmatory factor analysis was also conducted for the three sexual behavior items at each survey wave: frequency of oral, vaginal, and anal sex. These three items formed a single factor (see Table 1).
Table 1.
Sexual expectancy confirmatory factor analysis across three annual survey waves
| Item | Wave 1 | Wave 2 | Wave 3 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| I | II | III | IV | Sex | I | II | III | IV | Sex | I | II | III | IV | Sex | |
| Expectancies | |||||||||||||||
| Lose your self-respect | .83 | .85 | .84 | ||||||||||||
| Feel guilty | .73 | .75 | .83 | ||||||||||||
| Get a bad reputation | .72 | .76 | .76 | ||||||||||||
| Disappoint important people | .69 | .72 | .80 | ||||||||||||
| Get into trouble with parents | .57 | .51 | .67 | ||||||||||||
| Feel more attractive | .75 | .81 | .79 | ||||||||||||
| Feel more loved and wanted | .68 | .78 | .80 | ||||||||||||
| Prevent break up | .45 | .45 | .44 | ||||||||||||
| Feel closer to partner | .38 | .33 | .33 | .37 | .41 | .36 | |||||||||
| Fit in more with friends | .46 | ||||||||||||||
| Be more popular | .42 | .49 | .48 | ||||||||||||
| Feel more grown up | .72 | .69 | |||||||||||||
| Get a STD | .73 | .88 | .91 | ||||||||||||
| Get (someone) pregnant | .66 | .51 | .54 | ||||||||||||
| Get HIV/AIDS | .84 | .88 | |||||||||||||
| Enjoy it | .88 | .67 | .77 | ||||||||||||
| Have fun | .73 | .82 | |||||||||||||
| Feel excited | .81 | ||||||||||||||
| Feel satisfied | .79 | ||||||||||||||
| Feel pleasure | .80 | ||||||||||||||
| Feel happy | .86 | ||||||||||||||
| Behaviors | |||||||||||||||
| Oral Sex | .95 | .94 | .89 | ||||||||||||
| Vaginal Sex | .86 | .88 | .92 | ||||||||||||
| Anal Sex | .48 | .44 | .45 | ||||||||||||
Note: I = Social Risk II = Social Benefit III = Health Risk IV = Pleasure Sex = Sexual Behaviors. Table entries are standardized factor loadings.
Wave 1: χ2 (104) = 238.5, p < .00, BNFI = .94, CFI = .96, RMSEA = .04
Wave 2: χ2 (154) = 434.1, p < .00, BNFI = .95, CFI = .97, RMSEA = .04
Wave 3: χ2 (191) = 534.2, p < .00, BNFI = .95, CFI = .97, RMSEA = .04
Gender
A multi-group analysis with equality constraints on the corresponding unstandardized factor loadings was conducted for each wave to compare the factor structures for males and females. Results for the fully constrained models indicated that the same factor structure fit equally well for both genders at Wave 1 χ2 (141, Ns = 454, 477) = 292.5, p < .001, NFI = .92, CFI = .95, RMSEA = .05, Wave 2 χ2 (226, N s= 454, 477) = 547.1, p < .001, NFI = .92, CFI = .95, RMSEA = .06, and Wave 3 χ2 (291, Ns = 454, 477) = 591.3, p < .001, NFI = .93, CFI = .96, RMSEA = .05. That is, there was factor equivalence for males and females.
Age
A multi-group analysis with equality constraints on the corresponding unstandardized factor loadings was conducted for each wave to compare the factor structures for three groups based on Wave 1 age (≤13 years, 14–15, ≥16). The youngest group (age 13 and under) reported no experiences of anal sex at Wave 1. Therefore, this variable was deleted from the model for that group only at Wave 1. Equality constraints were included for the age groups of 14 to 15 year olds and the 16 and over groups since they reported anal sex at all three waves. Results indicated that the same factor structure fit equally well for all ages for Wave 1 χ2 (216, Ns = 363, 382, 187) = 354.6, p < .001, NFI = .90, CFI = .96, RMSEA = .05, Wave 2 χ2 (349, Ns = 363, 382, 187) = 586.0, p < .001, NFI = .92, CFI = .97, RMSEA = .05, and Wave 3 χ2 (446, N = 363, 382, 187) = 734.7, p < .001, NFI = .91, CFI = .96, RMSEA = .05.
Correlational analyses
Inter-factor correlations were then examined to determine relationships among the expectancy and sexual behavior factors. Correlations were significant among the factors within and across waves in the expected directions: Social Risk and Health Risk expectancies were positively correlated, Social Benefit and Pleasure expectancies were positively correlated, and the former were negatively correlated with the latter. Social Risk and Health Risk expectancies were negatively correlated with frequency of sexual behavior. Pleasure expectancies were positively correlated with sexual behavior. Only the relationships between Social Benefit expectancies and sexual behavior were consistently non-significant within and across waves.
Gender
Equivalence of the correlational models for males and females was assessed using multi-group modelingto compare models that included constraints on covariances among factors and the factor loadings and a second model that was unconstrained. The fully constrained model fit reasonably well χ2 (3120, N = 454, 477) = 4805.5, p < .001, NFI = .84, CFI = .93, RMSEA = .03 as did the unconstrained model χ2 (2952, N = 454, 477) = 4376.6, p < .001, NFI = .85, CFI = .94, RMSEA = .03. Although the difference in χ2 between the models is statistically significant (Δ χ2[168] = 428.9, p < .01), the change in other fit statistics was not substantive enough to warrant using the unconstrained model. Thus, the same model appears to hold for males and females. Correlations are presented in Table 2.
Table 2.
Correlations among sexual expectancies and sexual behaviors
| Wave 1 | Wave 2 | Wave 3 | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Soc Risk | Soc Ben | Hlth Risk | Pleas | Sex | Soc Risk | Soc Ben | Hlth Risk | Pleas | Sex | Soc Risk | Soc Ben | Hlth Risk | Pleas | Sex | ||
| Wave 1 | Soc Risk | 1.0 | ||||||||||||||
| Soc Ben | −.23 | 1.0 | ||||||||||||||
| Hlth Risk | .48 | −.08 | 1.0 | |||||||||||||
| Pleas | −.55 | .48 | −.18 | 1.0 | ||||||||||||
| Sex | −.39 | −.04 | −.27 | .32 | 1.0 | |||||||||||
| Wave 2 | Soc Risk | .72 | −.21 | .40 | −.52 | −.33 | 1.0 | |||||||||
| Soc Ben | −.18 | .65 | −.16 | .33 | −.00 | −.20 | 1.0 | |||||||||
| Hlth Risk | .37 | −.13 | .70 | −.30 | .17 | .48 | −.11 | 1.0 | ||||||||
| Pleas | −.52 | .47 | −.26 | .73 | .27 | −.69 | .68 | −.30 | 1.0 | |||||||
| Sex | −.47 | .10 | −.31 | .39 | −.73 | −.48 | .03 | −.32 | .44 | 1.0 | ||||||
| Wave 3 | Soc Risk | .69 | −.19 | .37 | −.48 | −.30 | .81 | −.19 | .38 | −.63 | −.28 | 1.0 | ||||
| Soc Ben | −.07 | .48 | −.10 | .21 | −.01 | −.05 | .75 | −.11 | .43 | −.04 | −.10 | 1.0 | ||||
| Hlth Risk | .34 | −.13 | .63 | −.29 | .16 | .43 | −.15 | .74 | −.34 | −.17 | .47 | −.12 | 1.0 | |||
| Pleas | −.39 | .34 | −.21 | .61 | .18 | −.49 | .49 | −.24 | .87 | .22 | −.56 | .50 | −.32 | 1.0 | ||
| Sex | −.50 | .11 | −.32 | .46 | .58 | −.54 | −.09 | −.29 | .51 | .75 | −.46 | −.01 | −.30 | .40 | 1.0 | |
Note. Italicized values are non-significant (absolute values between .00 and .07).
Age
Two models were compared, one that included constraints on covariances among factors and the factor loadings across the age groups and a second model that was unconstrained. The fully constrained model fit reasonably well χ2 (4708, N = 363, 382, 187) = 6810.9, p < .001, NFI = .77, CFI = .91, RMSEA = .04 as did the unconstrained model χ2 (4373, N = 363, 382, 187) = 5929.6, p < .001, NFI = .80, CFI = .94, RMSEA = .03. While the difference in χ2 between the models is statistically significant (Δ χ2[335] = 881.3, p < .01), the change in other fit statistics was not substantive enough to warrant using the unconstrained model. Thus, the same model appears to hold across age groups.
Reliability
Internal consistency was assessed for each of the subscales at each wave using Cronbach’s α for scales with at least three items and Pearson’s r for scales with only two items (see Table 3). The internal reliabilities were good, with αs ranging from .74 to .89 and inter-item correlations ranging from .44 – .49. The same tests were run on males and female separately, with αs ranging from .72 to .89 and correlations from .42–.51. Test-retest reliability was assessed by regressing each factor on itself from the previous wave one yearearlier. The resulting model was a good fit χ2 (1541, N = 932) = 2954.4, p < .001, NFI = .90, CFI = .94, RMSEA = .03. Even though the precise content of some of the scales changed over the course of the study as items were added or deleted, the stability coefficients were very good, ranging from .66 to .83 and accounting for 43%–69% of the variance in the factors across the waves.
Table 3.
Scale reliability and inter-item correlations
| Factor | Wave 1 | Wave 2 | Wave 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| M | F | All | M | F | All | M | F | All | |
| Health Risk | .42 | .51 | .49 | .74 | .79 | .78 | .79 | .82 | .81 |
| Social Benefit | .73 | .72 | .74 | .81 | .80 | .81 | .81 | .79 | .80 |
| Social Risk | .83 | .79 | .83 | .86 | .79 | .85 | .88 | .88 | .89 |
| Pleasure | .42 | .44 | .44 | .79 | .86 | .84 | .82 | .87 | .86 |
Note: Table entries are Cronbach’s alphas except for Wave 1 Health Risk and Pleasure scales, which are inter-item correlations because the scales comprised only two items.
Gender
Again, two multi-group models were run comparing males and females, one with equality constraints on factor loadings and stability coefficients and one without. Equality of the stability coefficients would indicate substantive equivalence of the relations among the factors over time and test-retest reliability. The fit was reasonable for both the constrained χ2 (3165, N = 454, 477) = 5044.9, p < .001, NFI = .83, CFI = .93, RMSEA = .04 and unconstrained models χ2 (3082, N = 454, 477) = 4776.3, p < .001, NFI = .84, CFI = .93, RMSEA = .04. Although the difference in χ2 was statistically significant between the constrained and unconstrained models (Δ χ2[83] = 268.6, p < .01), the change in other fit statistics was not substantive enough to warrant using the unconstrained model.
Age
Multi-group models were also run comparing the three age groups. The fit was satisfactory for both the constrained χ2 (4733, N = 363, 382, 187) = 6630.9, p < .001, NFI = .77, CFI = .92, RMSEA = .04 and unconstrained models χ2 (4568, N = 363, 382, 187) = 6288.1, p < .001, NFI = .79, CFI = .93, RMSEA = .04. Although the difference in χ2 was statistically significant between the models (Δ χ2[165] = 342.8, p < .01), the change in other fit statistics was not substantive enough to warrant using the unconstrained model.
Longitudinal analyses
The time ordered relations among expectancies and sexual behaviors were investigated with autoregressive latent variable structural equation modeling. Background variables gender, age, race (White/non-White), and ethnicity (Latino/non-Latino) were included as covariates. In the first model, in addition to the effects of each expectancy and behavior regressed on themselves, all expectancies at Wave 1 were entered into the equation predicting sexual behavior at Wave 2 and all expectancies at Wave 2 were entered into the equation predicting sexual behavior at Wave 3. Only Social Risk expectancies were found to be significant in predicting changes in later sexual behavior so the model was simplified to include only these expectancy effects. The resulting model had a reasonable fit χ2 (1753, N = 932) = 3474.9, p < .001, NFI = .88, CFI = .94, RMSEA = .03. Sexual behavior at the prior wave was then added to each equation predicting later sexual expectancies. Sexual behavior at Wave 2 was found to predict both Pleasure and Social Benefit expectancies at Wave 3 (see Figure 1) and the model was also a good fit χ2 (1753, N = 932) = 3752.9, p < .001, NFI = .89, CFI = .94, RMSEA = .04.
Figure 1.
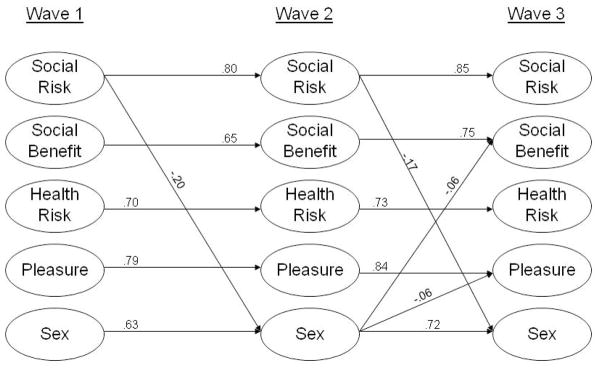
Standardized path diagram of the longitudinal relations among sexual expectancies and behaviors
Gender
Gender differences in the final model were again tested using two multi-group analyses. In this case, equivalence would indicate that the relations among expectancies and sexual behaviors over time were the same for both genders. That is, they are related in a similar fashion for both groups. Both models were a good fit for the data: constrained χ2 (3155, N = 454, 477) = 5497.3, p < .001, NFI = .82, CFI = .92, RMSEA = .04 and unconstrained χ2 (3082, N = 454, 477) = 5206.0, p < .001, NFI = .83, CFI = .93, RMSEA = .03. Again, although the difference in χ2 is statistically significant (Δ χ2[73] = 291.3, p < .01), the change in other fit statistics did warrant using the unconstrained model.
Age
Consistent with our prior findings, both the constrained and unconstrained models provided a satisfactory fit to the data across age groups: constrained χ2 (5245, N = 363, 382, 187) = 7448.1, p < .001, NFI = .76, CFI = .91, RMSEA = .04 and unconstrained χ2 (5039, N = 363, 382, 187) = 7017.4, p < .001, NFI = .77, CFI = .92, RMSEA = .04. Again, although the change in χ2 is statistically significant (Δ χ2[206] = 430.7, p < .01), the change in other fit statistics did not warrant using the unconstrained model.
Discussion
The current study examined the factor structure, reliability, and predictive validity of a new measure of sex expectancies, the Adolescent Sexual Expectancy Scale (ASEXS). The study also investigated the longitudinal relationships among sexual expectancies and sexual behavior over a three year period. Multi-group analyses were used to investigate gender and age differences in the factor structure of the items and the relations among the ASEXS factors and sexual behaviors. Confirmatory factor analyses indicated that four correlated factors were adequate to account for the sexual expectancy items. These factors corresponded to expectations regarding the likelihood of Social Risk, Social Benefit, Health Risk, and Pleasure. These subscales showed good internal consistency (α) and test-retest reliability. In longitudinal analyses, Social Risk expectancies were significantly related to sexual behavior after controlling for prior behavior and for background characteristics (e.g., age, ethnicity). Multi-group analyses indicated the factor structure, the relationships among factors, and the relationships between the factors and sexual behaviors were equivalent for males and females and across age groups.
Results suggest that sexual expectancies may influence sexual behaviors, which, in turn modify later expectancies. Specifically, Social Risk expectancies appear to function as a protective factor with adolescents who believe that sexual behavior is likely to have such negative consequences being less sexually active than those who believed such consequences were less likely. Recall that Social Risk expectancies consisted of items such as “lose your self-respect”, “disappoint people important to you”, and “get a bad reputation.” Although correlated cross-sectionally, Health Risk, Pleasure, and Social Benefit expectancies were not predictive of changes adolescent sexual behavior. It may be that adolescents give more weight to social and personal costs than to other considerations when making decisions about becoming sexually active. This serves as a reminder to parents about the critical role they play in affecting adolescent sexual behavior (Rafaelli, Bogenscheider & Flood, 1998; Whitaker & Miller, 2000). That is, parents may influence their child’s expectations regarding the social consequences of being sexually active through communication and thus discourage precocious or risky sexual behaviors. Additionally, from a prevention perspective, programs which highlight self-respect, parental expectations, and other social consequences may be more likely influence adolescent sexual activity than programs that emphasize other negative consequences. Similar to the findings of other studies (Guilano-Ramos, Jaccard, Dittus, Gonzalez, & Bouris, 2008), we found no relationship between health risk expectancies and sexual behavior. It is also important to note that health risk expectancies were not uniquely related to sexual behavior over time in the autoregressive model. This finding has significant implications given that many prevention programs stress negative health consequences associated with sexual behavior such as pregnancy and STIs as a deterrent strategy. Such efforts may be misplaced.
Sexual experience also modified expectancies. In particular, frequency of sexual activity at Wave 2 negatively predicted later Social Benefit and Pleasure expectancies, after controlling for prior sexual behaviors and expectancies. It seems that increased sexual experience might serve to disillusion teens of their unrealistic positive expectations for sex. Collectively, the findings highlight a dynamic relationship between expectancies and sexual behaviors, a relationship that educators should attend to as they facilitate the development of healthy sexual beliefs both among those who have had sexual experience as well as those who have not.
Finally, a strength of the ASEXS is the factorial invariance of the scale across age and gender groups. While there may be differences scale mean scores or developmental changes over time, the factor structure of sex expectancies and how they relate to sexual behavior is consistent among males and females, and older and younger adolescents.
Limitations
Some of the weaknesses of this study have been mentioned previously. One potential shortcoming of this new scale is the wording of the questions. We asked about participants’ expectations should they engage in vaginal intercourse. However, we did not note whether this was protected sex (i.e., sex with a condom), which has implications for the items related to STDs and pregnancy. Similarly, the expectancy items focused only on vaginal intercourse, excluding other sexual behaviors such as genital play, oral sex, and anal sex. Future studies should investigate whether the structure of expectancy beliefs differs between these behaviors and whether expectancies relate to them in the same way (cf. Halpern-Felsher et al., 2005).
Recommendations
The current paper reports on the development and validation of a new instrument for measuring adolescent beliefs about anticipated consequences associated with sexual behavior in four domains. Although the analyses indicated only minor gender and age differences in the factor structure of these beliefs or in their relationships with one another and behavior, future research should consider whether such difference may emerge among ethnic or other socio-demographic groups. Further research should also investigate more thoroughly the developmental trajectories of sexual expectancies. The social processes through which sexual expectancies are acquired and modified are as of yet unclear, but may include parental, peer, and media influences as well as direct experience (Martino, et al., 2005). These issues should be addressed. Sex expectancies also need to be considered in the context of other important factors that influence young people’s sexual behavior such as family and peer influences and related beliefs. The extent to which these factors are mediated through expectancies or have independent effects is an open question that should be addressed. Finally, additional studies are needed to identify sexual expectancies that may not have been captured in the ASEXS and to ascertain their role in adolescent risky or health promoting sexual behaviors.
Acknowledgments
This publication was made possible by Grant HD38906 from the National Institute of Child Health and Human Development (NICHD). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of NIAAA or NIH.
Footnotes
Alternatively, the expectancy items might be conceptualized as hierarchically organized. That is, the four factors might be seen as being related through a second-order factor representing overall expectations about the costs-benefits of having sex. Statistically, such a hierarchical model cannot be distinguished from the model presented here.
Contributor Information
Beth Bourdeau, Prevention Research Center, Pacific Institute for Research and Evaluation, 1995 University Avenue, Suite 450, Berkeley, CA 94704.
Joel W. Grube, Prevention Research Center, Pacific Institute for Research and Evaluation, 1995 University Avenue, Suite 450, Berkeley, CA 94704
Melina M. Bersamin, Prevention Research Center, Pacific Institute for Research and Evaluation, 1995 University Avenue, Suite 450, Berkeley, CA 94704
Deborah A. Fisher, Pacific Institute for Research and Evaluation, Calverton Office Park, 11720 Beltsville Drive, Suite 900, Calverton, MD 20705
References
- Aarons GA, Brown SA, Stice E, Coe MT. Psychometric evaluation of the marijuana and stimulant effect expectancy questionnaires for adolescents. Addictive Behaviors. 2001;26:219–236. doi: 10.1016/s0306-4603(00)00103-9. [DOI] [PubMed] [Google Scholar]
- Ajzen I. Nature and operation of attitudes. Annual Review of Psychology. 2001;52:27–58. doi: 10.1146/annurev.psych.52.1.27. [DOI] [PubMed] [Google Scholar]
- Bandura A. Social Foundations of Thought and Action: A Social Cognitive Perspective. Englewood Cliffs, NJ: Princeton-Hall; 1986. [Google Scholar]
- Bentler PM. EQS Structural Equations Program Manual. Encino, CA: Multivariate Software, Inc; 1995. [Google Scholar]
- Brick JM, Waksberg J, Kulp D, Starer A. Bias in list-assisted telephone samples. Public Opinion Quarterly. 1995;59:218–235. [Google Scholar]
- Council of American Survey Research Organizations. Report of the CASRO Completion Rates Task Force. New York: Audits and Surveys Company, Inc; 1982. [Google Scholar]
- California Health Interview Survey. Data and findings. Los Angeles, CA: UCLA Center for Health Policy Research; 2005. Retrieved October 14, 2005 from http://www.chis.ucla.edu/ [Google Scholar]
- Chen MJ, Grube JW, Madden PA. Alcohol expectancies and adolescent drinking: Differential prediction of frequency, quantity, and intoxication. Addictive Behaviors. 1994;19:521–529. doi: 10.1016/0306-4603(94)90007-8. [DOI] [PubMed] [Google Scholar]
- Cooper ML, Shapiro CM, Powers AM. Motivations for sex and risky sexual behavior among adolescents and young adults: a functional perspective. Journal of Personality and Social Psychology. 1998;75:1528–1558. doi: 10.1037//0022-3514.75.6.1528. [DOI] [PubMed] [Google Scholar]
- Fromme K, Katz E, Rivet K. Outcome expectancies and risk-taking behavior. Cognitive Therapy and Research. 1997;21:421–442. [Google Scholar]
- Fromme K, Wendel J. Beliefs about the effects of alcohol on involvement in coercive and consenting sexual activities. Journal of Applied Social Psychology. 1995;25:2009–2117. [Google Scholar]
- Gebhardt WA, Kuyper L, Greunsven G. Need for intimacy in relationships and motives for sex as determinants of adolescent condom use. Journal of Adolescent Health. 2003;33:154–164. doi: 10.1016/s1054-139x(03)00137-x. [DOI] [PubMed] [Google Scholar]
- Gillmore MR, Morrison DM, Lowery C, Baker SA. Beliefs about condoms and their association with intentions to use condoms among youths in detention. Journal of Adolescent Health. 1994;15:228–237. doi: 10.1016/1054-139x(94)90508-8. [DOI] [PubMed] [Google Scholar]
- Goldman MS, Del Boca FK, Darkes J. Alcohol expectancy theory. In: Leonard KE, Blane HT, editors. Psychological Theories of Drinking and Alcoholism. New York: Guilford Press; 1999. pp. 203–246. [Google Scholar]
- Grube JW, Agostinelli GE. Perceived consequences and adolescent drinking: Nonlinear and interactive models of alcohol expectancies. Psychology of Addictive Behaviors. 1999;13:303–312. [Google Scholar]
- Guilamo-Ramos V, Jaccard J, Dittus P, Bouris A, Holloway I, Casillas E. Adolescent expectancies, parent-adolescent communication and intentions to have sexual intercourse among inner-city, middle school youth. Annals of Behavioral Medicine. 2007;34:56–66. doi: 10.1007/BF02879921. [DOI] [PubMed] [Google Scholar]
- Guilamo-Ramos V, Jaccard J, Dittus P, Gonzalez B, Bouris A. A conceptual framework for the analysis of risk and problem behaviors: The case of adolescent sexual behavior. Social Work Research. 2008;31(1):29–45. [Google Scholar]
- Halpern-Felsher BL, Cornell JL, Kropp RY, Tschann JM. Oral versus vaginal sex among adolescents: perceptions, attitudes, and behavior. Pediatrics. 2005;115:845–51. doi: 10.1542/peds.2004-2108. [DOI] [PubMed] [Google Scholar]
- Kamb ML, Fishbein M, Douglas JM, Rhodes F, Rogers J, Bolan G, et al. Efficacy of risk-reduction counseling to prevent human immunodeficiency virus and sexually transmitted diseases: a randomized controlled trial. Project RESPECT Study Group. Journal of the American Medical Association. 1998;280:1161–1167. doi: 10.1001/jama.280.13.1161. [DOI] [PubMed] [Google Scholar]
- Katz EC, Fromme K, D’Amico JD. Effects of outcome expectancies and personality on young adults’ illicit drug use, heavy drinking, and risky sexual behavior. Cognitive Therapy and Research. 2000;24:1–22. [Google Scholar]
- Leigh BC, Stacy AW. Alcohol expectancies and drinking in different age groups. Addiction. 2004;99:215–27. doi: 10.1111/j.1360-0443.2003.00641.x. [DOI] [PubMed] [Google Scholar]
- Lewis-Esquerre JM, Rodrigue JR, Kahler CW. Development and validation of an adolescent smoking consequences questionnaire. Nicotine and Tobacco Research. 2005;7:81–90. doi: 10.1080/14622200412331328475. [DOI] [PubMed] [Google Scholar]
- Martino SC, Collins RL, Kanouse DE, Elliott M, Berry SH. Social cognitive processes mediating the relationship between exposure to television’s sexual content and adolescents’ sexual behavior. Journal of Personality and Social Psychology. 2005;89:914–924. doi: 10.1037/0022-3514.89.6.914. [DOI] [PubMed] [Google Scholar]
- Newman JC, Des Jarlais DC, Turner CF, Gribble J, Cooley P, Paone D. The differential effects of face-to-face and computer interview modes. American Journal of Public Health. 2002;92:294–297. doi: 10.2105/ajph.92.2.294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- O’Donnell L, Myint-U A, O’Donnell CR, Stueve A. Long-term influence of sexual norms and attitudes on timing of sexual initiation among urban minority youth. Journal of School Health. 2003;73:68–75. doi: 10.1111/j.1746-1561.2003.tb03575.x. [DOI] [PubMed] [Google Scholar]
- Olson JM, Roese NJ, Zanna M. Expectancies. In: Higgins TE, Kruglanski AW, editors. Social psychology: Handbook of basic principles. New York: Guilford; 1996. pp. 211–238. [Google Scholar]
- Ott MA, Millstein SG, Ofner S, Halpern-Felsher BL. Greater Expectations: Adolescents’ Positive Motivations for Sex. Perspectives on Sexual and Reproductive Health. 2006;38:84–89. doi: 10.1363/psrh.38.084.06. [DOI] [PubMed] [Google Scholar]
- Rafaelli M, Bogenscheider K, Flood MF. Parent-teen communication about sexual topics. Journal of Family Issues. 1998;19(3):315–333. doi: 10.1177/019251398019003005. [DOI] [PubMed] [Google Scholar]
- Rhodes F, Stein JA, Fishbein M, Goldstein RB, Rotheram-Borus MJ. Using theory to understand how interventions work: Project RESPECT, condom use, and the Integrative Model. AIDS and Behavior. 2007;11:393–407. doi: 10.1007/s10461-007-9208-9. [DOI] [PubMed] [Google Scholar]
- Romer D, Hornick R, Stanton B, Black M, Li X, Ricardo I, Feigelman S. “Talking” computers: A reliable & private method to conduct interviews on sensitive topics with children. Journal of Sex Research. 1997;34:3–9. [Google Scholar]
- Sieving RE, Bearinger LH, Resnick MD, Pettingell S, Skay C. Adolescent dual method use: relevant attitudes, normative beliefs and self-efficacy. Journal of Adolescent Health. 2007;40:275, e15–e22. doi: 10.1016/j.jadohealth.2006.10.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Small SA, Silverberg SB, Kerns D. Adolescents’ perceptions of the costs and benefits of engaging in health-compromising behaviors. Journal of Youth and Adolescence. 1993;22:73–87. [Google Scholar]
- Tucker C, Lepkowski JM, Piekarski L. The current efficiency of list-assisted telephone sampling designs. Public Opinion Quarterly. 2002;66:321–338. [Google Scholar]
- Turner CF, Ku L, Rogers SM, Lindberg LD, Pleck JH, Sonenstein FL. Adolescent sexual behavior, drug use, and violence: Increased reporting with computer survey technology. Science. 1998;280:867–873. doi: 10.1126/science.280.5365.867. [DOI] [PubMed] [Google Scholar]
- Vangsness L, Bry BH, LaBouvie EW. Impulsivity, negative expectancies, and marijuana use: a test of the acquired preparedness model. Addictive Behaviors. 2005;30:1071–1076. doi: 10.1016/j.addbeh.2004.11.003. [DOI] [PubMed] [Google Scholar]
- Wahl SK, Turner LR, Mermelstein RJ, Flay BR. Adolescents’ smoking expectancies: psychometric properties and prediction of behavior change. Nicotine and Tobacco Research. 2005;7:613–623. doi: 10.1080/14622200500185579. [DOI] [PubMed] [Google Scholar]
- Whitaker DJ, Miller KS. Parent-adolescent discussions about sex and condoms. Journal of Adolescent Research. 2000;15(2):251–273. [Google Scholar]
- Widdice LE, Cornell JL, Liang W, Halpern-Felsher BL. Having sex and condom use: Potential risks and benefits reported by young, sexually inexperienced adolescents. Journal of Adolescent Health. 2006;39:588–595. doi: 10.1016/j.jadohealth.2006.03.016. [DOI] [PubMed] [Google Scholar]