

Abstract
Background
Health care workers (HCWs) are at the interface between hospitals and communities. The survey for methicillin-resistant Staphylococcus aureus (MRSA) carriage among HCWs has mostly been conducted to investigate outbreaks or endemics. Community-associated MRSA are prevalent among children in Taiwan. We conducted this study to better understand the carriage rate of MRSA among pediatricians in non-outbreak situations in Taiwan,.
Methods
A total of 220 pediatricians from Taiwan who attended the annual meeting of Taiwan Pediatric Association in April, 2010 were recruited to participate in this study and were sampled from the nares for the detection of MRSA by polymerase chain reaction (PCR) and further by culture. The following molecular analyses were performed, including pulsed-field gel electrophoresis (PFGE), multilocus sequence typing (MLST), typing of staphylococcal cassette chromosome mec (SCCmec) and the presence of Panton-Valentine leukocidin (PVL) genes.
Results
MRSA was detected from 15 attendees (6.8%) by PCR. MRSA-colonized attendees had a significantly lower rate (0.041) of working in the medical center, while borderline significantly higher rate of working in the Regional Hospital (p=0.056), than those without MRSA colonization. From those 15 samples, 12 MRSA isolates were identified by culture and molecularly characterized. Three PFGE patterns, two sequence types (ST 59, ST 508), and two SCCmec types (IV and VT) were identified, respectively. Five isolates, including three carrying SCCmec types VT, were PVL-positive. All 12 isolates were susceptible to vancomycin, teicoplanin, linezolid, fusidic acid, trimethoprim/sulfamethoxazole, and doxycyclin, and resistant to penicillin.
Conclusion/significance
Around seven percent of pediatricians in Taiwan harbored CA-MRSA in their nares.
Introduction
Methicillin-resistant Staphylococcus aureus (MRSA) is a concern for most hospitals worldwide due to its increasing prevalence [1,2]. MRSA is usually considered a hospital pathogen, but increasingly, it is acquired in the community [3,4]. MRSA infections, though acquired in the community, were traditionally confined to individuals with health care-associated risk factors such as residence in long term care facility, recent hospitalization or surgery, indwelling catheter or hemodialysis [5]. However, the changing epidemiology of MRSA became evident in the 1990s when MRSA infections occurred in previously healthy children without established risk factors for MRSA acquisition [3-5], namely community-associated MRSA (CA-MRSA). CA-MRSA has started to spread from the community into hospitals, where outbreaks have occurred [6,7]. CA-MRSA strains have been recognized as a pathogen which is often genetically different from the healthcare-associated (HA) MRSA, such as relatively limited antibiotic resistance, mostly possessing Panton-Valentine leukocidin genes, usually carrying type IV or V staphylococcal cassette chromosome etc. [3,4].
In Taiwan, CA-MRSA infections have been increasingly reported in pediatric patients since first reported in 2002. MRSA accounting for CA S. aureus infections in children without risk factors increased from 9.8% in 1997-2000 to 56% during 2004-05 [8]. Likewise, the nasal MRSA carriage rate for well-child healthcare visits and/or in school children increased from 1.9% in 2001 to ~10.2 % in 2007-2008 [8]. CA-MRSA infections were relatively uncommonly reported in adults in Taiwan and the carriage rate among adults was also relatively low, around 3.8% [8]. Up to 2008, most CA-MRSA isolates in Taiwan shared common molecular characteristics and >80% of the isolates belonged to the clonal complex 59 (sequence type 59 and its variants) [8].
Health care workers (HCWs) are at the interface between hospitals and communities. The survey for MRSA carriage among HCWs has mostly been conducted to investigate outbreaks or endemics but not in non-outbreak situations [9]. Since a substantial proportion of children in Taiwan had nasal MRSA colonization, we conducted this study to better understand the extent of nasal MRSA carriage rate among pediatricians in Taiwan who cared for these children.
Materials and Methods
The study was approved by the institutional review board of Chang Gung Memorial Hospital. All participants of the Joint Meeting of 196th Annual Meeting of Taiwan Pediatric Association and 6th Annual Conference of Asian Society of Pediatric Research, April 23-26, 2010, which were held in Taipei, Taiwan, were eligible and were invited to participate in this study. A total of 220 pediatricians from Taiwan were recruited and sampled from the nares after a written consent was obtained and a questionnaire including the demographics and medical facilities they work for was obtained.
For each subject, nasal swab specimen was collected from the anterior nares using 2 separate dry Copan Transystem Liquid Stuart swabs (Venturi Transystem; Copan Diagnostics, Corona, CA). Each swab was rubbed inside the anterior nares, first into one side and then into the other, ensuring that each swab contained specimens of both nares of each subject. These swabs were then transported at room temperature and processed within 4 hours. A polymerase chain reaction test (BD GeneOhmTM Staph SR Assay; Becton Dickinson, NJ, USA) was used to detect MRSA first. For those with positive PCR results, the swabs were further put into Mueller Hinton Broth (Becton, Dickinson and Co.) in CO2 incubator at 37°C overnight and then was subcultured into TSA II 5% SB plate (Becton, Dickinson and Comapany, Sparks, MD) to obtain MRSA isolates for molecular characterization. After incubation and subcultivation, coagulase test were conducted by using rabbit plasma to ensure the identification of S. aureus. Cefoxitin test was then used to distinguish the MRSA from methicillin-susceptible S. aureus (MSSA) based on the recommendation of Clinical and Laboratory Standards Institute (CLSI) [10]. Once MRSA was isolated, the strains were frozen until the processing for molecular characterization.
The susceptibility test was performed on Mueller–Hinton agar with disk-diffusion method following the protocol of CLSI [10] and included oxacillin, doxycyclin, vancomycin, teicoplanin, penicillin, trimethoprim/sulfamethoxazole, erythromycin, clindamycin, linezolid, fusidic acid [10].
The extraction and purification of MRSA chromosomal DNA were conducted by using DNA kit (QIAamp® DNA Blood Mini Kit, QIAGEN). Pulsed-field gel electrophoresis (PFGE) with SmaI digestion was used to fingerprint all MRSA isolates according to the procedure described previously [11,12]. Staphylococcal chromosome cassette mec (SCCmec) type, and the presence of Panton-Valentine leukocidin (PVL) genes were determined by PCR assays according to the procedure described previously [11-15]. Multilocus sequence typing (MLST) [16] and spa typing [17] were performed for strains of representative PFGE patterns as described elsewhere. The procedure for the detection of sasX gene followed that described by Li et al and the primers used were sasX-f agaattagaagtacgtctaaatgc and sasX-r gctgattatgtaaatgactcaaatg [18].
Statistical analyses were performed with the Statistical Package for the Social Sciences (SPSS software for Windows, version 15.0). Statistical significance was based on a significance level of less than 0.05.
Results
Of the 220 participants, 139 (63.2%) were male. Most attendees aged between 31-60 years (80%). Table 1 illustrates the demographics and medical facilities of the participants. 66 participants (30%) worked in medical centers, and 94 (42.7%) worked in clinics.
Table 1. Comparison of demographics between participants with and without methicillin-resistant Staphylococcus aureus colonization.
| Characteristics | Total (n=220) No. (%) | Colonized (n=15) No. (%) | Un-colonized (n=205) No. (%) | p value |
|---|---|---|---|---|
| Male gender | 139 (63.2) | 11 (73) | 128 (62) | NS |
| Age (yrs) | ||||
| <30 | 8 (3.6) | 0 | 8 (3.9) | NS |
| 31-40 | 78 (35.5) | 7 (47) | 71 (35) | NS |
| 41-50 | 55 (25.0) | 2 (13) | 53 (26) | NS |
| 51-60 | 42 (19.1) | 2 (13) | 40 (20) | NS |
| >60 | 37 (16.8) | 4 (27) | 33 (16) | NS |
| Medical career (yrs) | ||||
| <5 | 14 (6.4) | 2 (13) | 12(5.9) | NS |
| 6-10 | 56 (25.5) | 4 (26) | 52 (25) | NS |
| 11-20 | 60 (27.3) | 4 (26) | 56 (27) | NS |
| 21-30 | 46 (20.9) | 3 (20) | 43 (21) | NS |
| >30 | 44 (20.0) | 2 (13) | 42 (20) | NS |
| Clinician | 210 (95.5) | 14 (93) | 196 (96) | NS |
| Health care units | ||||
| Medical center | 66 (30.0) | 1 (6.7) | 65 (32) | 0.041 |
| Regional hospital | 35 (15.9) | 5 (33) | 30 (15) | 0.056 |
| Local hospital | 19 (8.6) | 1 (6.7) | 18 (8.8) | NS |
| Clinics | 94 (42.7) | 8 (53) | 86 (42) | NS |
| Others | 6 (2.7) | 0 | 6 (2.9) | NS |
MRSA was detected by PCR in 15 participants, with a carriage rate of 6.8%. Comparing the demographics between those with and without MRSA colonization (Table 1), we found that MRSA-colonized participants had a significantly lower rate of working in the medical center (p=0.041), while a higher rate of working in the regional hospital (p=0.056), than those without MRSA colonization.
The nasal specimens from the PCR-positive participants were further cultured and MRSA were isolated from 12 specimens. All 12 isolates were molecularly characterized and the detailed molecular characteristics and antibiograms of the 12 MRSA isolates are shown in Figure 1. Three PFGE patterns (type C for 6 isolates, type D for 4 and type AK for 2), two sequence types (ST 59 for PFGE type C and D, and ST 508 for PFGE type AK), three spa types (t437 and t441 for ST 59, and t15 for ST 508/PFGE type AK), and two SCCmec types (IV for 9 isolates and VT for 3) were identified, respectively. Three isolates carrying SCCmec VT and two isolates with SCCmec IV were PVL-positive. All 12 isolates were susceptible to vancomycin, teicoplanin, trimethoprim/sulfamethoxazole, linezolid, fusidic acid, and doxycyclin, and resistant to penicillin, respectively (Figure 1). Only two isolates were susceptible to clindamycin and one of them was also susceptible to erythromycin. None of the 12 MRSA isolates carried the sasX gene.
Figure 1. Molecular characterization of the 12 MRSA isolates.
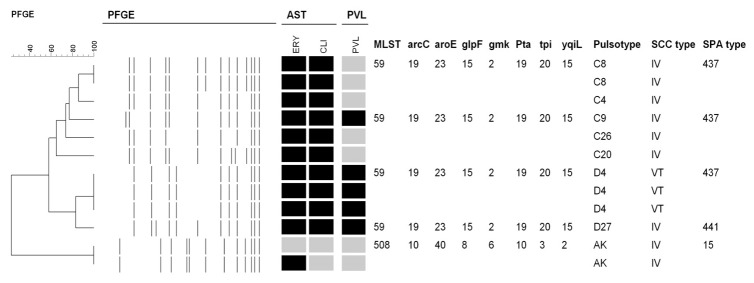
All 12 isolates were susceptible to vancomycin, teicoplanin, linezolid, fusidic acid, trimethoprim/sulfamethoxazole, and doxycyclin, and resistant to penicillin. Antimicrobial susceptibility tests (AST): black indicates resistance, and grey indicates susceptibility. Abbreviations are as follows: clindamycin (CLI), and erythromycin (ERY). PFGE, pulsed-field gel electrophoresis. PVL: black indicates that the Panton-Valentine leukocidin genes were detected. SCCmec, staphylococcal cassette chromosome mec elements; MLST, multilocus sequence type.
Discussion
Results from the present study indicate that 6.8% of pediatricians in Taiwan had MRSA carriage in the nares. The rate was comparable to that among HCWs reported from Taiwan previously, which ranged from 5.0% among those working in ordinary wards to 7.8% among those working in endemic neonatal intensive care units [19-21]. However, the rate of nasal MRSA carriage for pediatricians in the present study was higher than that for general adult population in Taiwan. For example, the rate of nasal MRSA carriage was 3.6% for healthy adults [21], 3.8% for 296 adult patients receiving hemodialysis [22], 3.8% for 502 adult patients visiting emergency room [23], 3.8% for 3098 adults for health examination [24] and 4.8% for 500 parturient mothers [25]. But the rate was lower than that for healthy children, ranging from 6.2% to 9.5% between 2005 and 2008 [26]. But, for contacts, previous reports from Taiwan indicated that the nasal MRSA carriage rate was found to be 13.6% for 66 contacts with a severe case of CA-MRSA infection [20], and 25%for 121 household contacts [27]. The issue whether contact with children or patients with MRSA infection is associated with a higher MRSA carriage rate for pediatricians needs further investigations.
In the present study, we used the BD GeneOhm StaphSR assay to detect nasal MRSA carriage first. As a screening method, the BD GeneOhm StaphSR assay could rapidly detect MRSA colonization in humans. In our previous study [28], we found a negative result of the assay could almost exclude S. aureus colonization, while a positive result should require culture to confirm it. However, Bartels et al [29] reported that some MRSA isolates with specific SCCmec could be missed by the BD GeneOhm StaphSR assay.
All the MRSA isolates available for molecular characterization were found to carry either type IV or V SCCmec, which suggests the isolates are community strains. Most isolates, though not as multi-resistant as HA-MRSA, were resistant to clindamycin and erythromycin. Further characterizations demonstrated that 10 of the 12 isolates belonged to ST 59 which is a typical community strains in Taiwan [8,13,26]. Again, these findings partly reflected that CA-MRSA was prevalent in Taiwan.
SasX gene is a novel staphylococcal gene encoding a surface-anchored protein and was increasingly identified in the MRSA strains of ST239 background during 2003 and 2011 in China [18]. It has been demonstrated that the SasX protein can promote nasal colonization and enhance virulence of S. aureus and was further proposed as the crucial factor contributing to the MRSA epidemic in Asia [18,30]. None of the 12 MRSA isolates in the present study carried this gene, which indicated that there was no evidence of transfer of sasX gene from ST239 MRSA isolates to those with other genetic background yet.
The role of HCWs on MRSA transmission is the source, vector or victim, which is an issue needed to be elucidated and explored. In addition, it is intriguing that HCWs working in medical centers had a significant lower nasal MRSA carriage rate, while those working in regional hospitals had a borderline significant higher carriage rate. This finding as well as its clinical implication needs to be further delineated.
Acknowledgments
The author are grateful to the staff working in Becton Dickinson Company of Taiwan, and the medical students of Chang Gung University College of Medicine, including Sheng-Yun Lu, Fang-Yu Chang, Ching-Chung Cheng and Chhong-Siin Chen, for their assistance of specimens sampling.
Funding Statement
This work was supported by a grant from Chang Gung Memorial Hospital (CMRPG 460113). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- 1. Fluit AC, Wielders CL, Verhoef J, Schmitz FJ (2001) Epidemiology and susceptibility of 3,051 Staphylococcus aureus isolates from 25 university hospitals participating in the European SENTRY study. J Clin Microbiol 39: 3727-3732. doi: 10.1128/JCM.39.10.3727-3732.2001. PubMed: 11574603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Klevens RM, Edwards JR, Tenover FC, McDonald LC, Horan T et al. (2006) Changes in the epidemiology of methicillin-resistant Staphylococcus aureus in intensive care units in US hospitals, 1992-2003. Clin Infect Dis 42: 389-391. doi: 10.1086/499367. PubMed: 16392087. [DOI] [PubMed] [Google Scholar]
- 3. David MZ, Daum RS (2010) Community-associated methicillin-resistant Staphylococcus aureus: epidemiology and clinical consequences of an emerging epidemic. Clin Microbiol Rev 23: 616-687. doi: 10.1128/CMR.00081-09. PubMed: 20610826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. DeLeo FR, Otto M, Kreiswirth BN, Chambers HF (2010) Community-associated meticillin-resistant Staphylococcus aureus . Lancet 375: 1557-1568. doi: 10.1016/S0140-6736(09)61999-1. PubMed: 20206987. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Naimi TS, LeDell KH, Como-Sabetti K, Borchardt SM, Boxrud DJ et al. (2003) Comparison of community- and health care-associated methicillin-resistant Staphylococcus aureus infection. JAMA 290: 2976-2984. doi: 10.1001/jama.290.22.2976. PubMed: 14665659. [DOI] [PubMed] [Google Scholar]
- 6. Saiman L, O'Keefe M, Graham PL, Wu F, Saïd-Salim R et al. (2003) Hospital transmission of community-acquired methicillin-resistant Staphylococcus aureus among postpartum women. Clin Infect Dis 37: 1313-1319. doi: 10.1086/379022. PubMed: 14583864. [DOI] [PubMed] [Google Scholar]
- 7. Maree CL, Daum RS, Boyle-Vavra S, Matayoshi K, Miller LG (2007) Community-associated methicillin-resistant Staphylococcus aureus isolates causing healthcare-associated infections. Emerg Infect Dis 13: 236-242. doi: 10.3201/eid1302.060781. PubMed: 17479885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Huang YC, Chen CJ (2011) Community-associated methicillin-resistant Staphylococcus aureus in children in Taiwan, 2000s. Inter J Antimicro Agent 38: 2-8. doi: 10.1016/j.ijantimicag.2011.01.011. [DOI] [PubMed] [Google Scholar]
- 9. Albrich WC, Harbarth S (2008) Health-care workers: source, vector, or victim of MRSA? Lancet Infect Dis 8: 289-301. doi: 10.1016/S1473-3099(08)70097-5. PubMed: 18471774. [DOI] [PubMed] [Google Scholar]
- 10. Clinical and Laboratory Standards Institute (2007) Performance standards for antimicrobial susceptibility testing; sixteenth informational supplement, 17th ed.. Clinical and Laboratory Standards Institute, Wayne, PA: . pp. M100-MS17 [Google Scholar]
- 11. Huang YC, Ho CF, Chen CJ, Su LH, Lin TY (2008) Comparative molecular analysis of community-associated and healthcare-associated methicillin-resistant Staphylococcus aureus isolates from children in northern Taiwan. Clin Microbiol Infect 14: 1167-1172. doi: 10.1111/j.1469-0691.2008.02115.x. PubMed: 19076845. [DOI] [PubMed] [Google Scholar]
- 12. Huang YC, Su LH, Wu TL, Lin TY (2006) Changing molecular epidemiology of methicillin-resistant Staphylococcus aureus bloodstream isolates from a teaching hospital in Northern Taiwan. J Clin Microbiol 44: 2268-2270. doi: 10.1128/JCM.00776-06. PubMed: 16757637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Kondo Y, Ito T, Ma XX, Watanabe S, Kreiswirth BN et al. (2007) Combination of multiplex PCRs for staphylococcal cassette chromosome mec type assignment: rapid identification system for mec, ccr, and major differences in junkyard regions. Antimicrob Agents Chemother 51: 264-274. doi: 10.1128/AAC.00165-06. PubMed: 17043114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Lina G, Piémont Y, Godail-Gamot F, Bes M, Peter MO et al. (1999) Involvement of Panton-Valentine leukocidin-producing Staphylococcus aureus in primary skin infections and pneumonia. Clin Infect Dis 29: 1128-1132. doi: 10.1086/313461. PubMed: 10524952. [DOI] [PubMed] [Google Scholar]
- 15. Oliveira DC, de Lencastre H (2002) Multiplex PCR strategy for rapid identification of structural types and variants of the mec element in methicillin-resistant Staphylococcus aureus . Antimicrob Agents Chemother 46: 2155-2161. doi: 10.1128/AAC.46.7.2155-2161.2002. PubMed: 12069968. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Enright MC, Day NP, Davies CE, Peacock SJ, Spratt BG (2000) Multilocus sequence typing for characterization of methicillin-resistant and methicillin-susceptible clones of Staphylococcus aureus . J Clin Microbiol 38: 1008-1015. PubMed: 10698988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Harmsen D, Claus H, Witte W, Rothgänger J, Claus H et al. (2003) Typing of methicillin-resistant Staphylococcus aureus in a university hospital setting by using novel software for spa repeat determination and database management. J Clin Microbiol 41: 5442-5448. doi: 10.1128/JCM.41.12.5442-5448.2003. PubMed: 14662923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Li M, Du X, Villaruz AE, Diep BA, Wang D et al. (2012) MRSA epidemic linked to a quickly spreading colonization and virulence determinant. Nat Med 18: 816-819. doi: 10.1038/nm.2692. PubMed: 22522561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Huang YC, Chou YH, Su LH, Lien RI, Lin TY (2006) Methicillin-resistant Staphylococcus aureus colonization and its association with infection among infants hospitalized in neonatal intensive care units. Pediatrics 118: 469-474. doi: 10.1542/peds.2006-0254. PubMed: 16882797. [DOI] [PubMed] [Google Scholar]
- 20. Huang YC, Su LH, Lin TY (2004) Nasal carriage of methicillin-resistant Staphylococcus aureus in contacts of an adolescent with community-acquired disseminated disease. Pediatr Infect Dis J 23: 919-922. doi: 10.1097/01.inf.0000141745.12941.ef. PubMed: 15602191. [DOI] [PubMed] [Google Scholar]
- 21. Lu PL, Chin LC, Peng CF, Chiang YH, Chen TP et al. (2005) Risk factors and molecular analysis of community methicillin-resistant Staphylococcus aureus carriage. J Clin Microbiol 43: 132-139. doi: 10.1128/JCM.43.1.132-139.2005. PubMed: 15634961. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Kang YC, Tai WC, Yu CC, Kang JH, Huang YC (2012) Methicillin-resistant Staphylococcus aureus nasal carriage among patients receiving hemodialysis in Taiwan: prevalence rate, molecular characterization and de-colonization. BMC Infect Dis 12: 284. doi: 10.1186/1471-2334-12-284. PubMed: 23116411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Lu SY, Chang FY, Cheng CC, Lee KD, Huang YC (2011) Methicillin-resistant Staphylococcus aureus nasal colonization among adult patients visiting emergency department in a medical center in Taiwan. PLOS ONE 6: e18620. doi: 10.1371/journal.pone.0018620. PubMed: 21695178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Wang JT, Liao CH, Fang CT, Chie WC, Lai MS et al. (2009) Prevalence of and risk factors for colonization by methicillin-resistant Staphylococcus aureus among adults in community settings in Taiwan. J Clin Microbiol 47: 2957-2963. doi: 10.1128/JCM.00853-09. PubMed: 19625471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Huang YC, Chao AS, Chang SD, Chen YJ, Peng MT et al. (2009) Association of Staphylococcus aureus colonization in parturient mothers and their babies. Pediatr Infect Dis J 28: 742-744. doi: 10.1097/INF.0b013e31819c132a. PubMed: 19633520. [DOI] [PubMed] [Google Scholar]
- 26. Chen CJ, Hsu KH, Lin TY, Hwang KP, Chen PY et al. (2011) Factors associated with nasal colonization of methicillin-resistant Staphylococcus aureus among healthy children in Taiwan. J Clin Microbiol 49: 131-137. doi: 10.1128/JCM.01774-10. PubMed: 21084507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Huang YC, Ho CF, Chen CJ, Su LH, Lin TY (2007) Nasal carriage of methicillin-resistant Staphylococcus aureus in household contacts of children with community-acquired diseases in Taiwan. Pediatr Infect Dis J 26: 1066-1068. doi: 10.1097/INF.0b013e31813429e8. PubMed: 17984820. [DOI] [PubMed] [Google Scholar]
- 28. Ho TH, Huang YC, Lin TY (2011) Evaluation of the BD GeneOhm StaphSR assay for detection of Staphylococcus aureus in patients in intensive care units. J Microbiol Immunol Infect 44: 310-315. doi: 10.1016/j.jmii.2010.08.008. PubMed: 21524966. [DOI] [PubMed] [Google Scholar]
- 29. Bartels MD, Boye K, Rohde SM, Larsen AR, Torfs H et al. (2009) A common variant of staphylococcal cassette chromosome mec type IVa in isolates from Copenhagen, Denmark, is not detected by the BD GeneOhm methicillin-resistant Staphylococcus aureus assay. J Clin Microbiol 47: 1524-1527. doi: 10.1128/JCM.02153-08. PubMed: 19297600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Otto M (2012) Molecular insight into how MRSA is becoming increasingly dangerous. Virulence 3: 521–522. doi: 10.4161/viru.21523. PubMed: 23076285. [DOI] [PMC free article] [PubMed] [Google Scholar]