

Abstract
Poland syndrome is a rare congenital anomaly classically consisting of unilateral hypoplasia of the sternocostal head of the pectoralis major muscle and ipsilateral brachysyndactyly. It was first described by Alfred Poland in 1840 and may occur with different gravity. Our patient is an eight-year-old Nigerian girl with left-sided anterior chest wall defect with no detectable structural heart abnormality but presented with repeated episodes of syncopal attacks following minor trauma to the anterior chest wall.
Keywords: Nigeria, pectoralis major, Poland, syndrome
Introduction
Poland syndrome is a rare congenital anomaly classically consisting of the combination of unilateral aplasia or hypoplasia of the sternocostal heads of the major pectoral muscles and ipsilateral brachysyndactyly.[1,2,3] Other usual anomalies in Poland syndrome are malformations of the anterior chest wall and breast. Dextrocardia, lung herniation, renal, vertebral and lower limb malformations have also been described in rare cases.[4] Furthermore, reports of Poland syndrome associated with other known syndromes in the same individual are not uncommon. In fact, associations with Moebius syndrome, facio-auriculo-vertebral dysplasia and frontonasal dysplasia have been described.[5] The incidence of Poland syndrome has been reported to be 1 in 30,000 live births.[6] Poland syndrome affects the right side of the chest in 67-75% of cases,[7,8] with a female-to-male ratio of 1:3 reported by Fraser et al.,[7] while equal sex distribution was documented by Uster.[9] However only few cases of Poland syndrome have been reported in patients in the sub-Saharan Africa.[10,11,12] We therefore report a case of Poland syndrome in an eight-year-old girl with an associated brachial fistula.
Case Report
An eight-year-old girl first seen at the Paediatric Out-Patient Department of Aminu Kano Teaching Hospital, Kano, with left anterior chest wall deformity since birth and recurrent loss of consciousness of two years duration. There was no history of breathlessness, paroxysmal nocturnal dyspnea or orthopnea. About a year ago, she developed a swelling on the left side of the jaw which was incised by a traditional barber and a thick whitish secretion was drained. However since then mother noticed that the site had been discharging clear fluid intermittently whenever She laughed, coughed, ate or cried. There was history of syncopal attacks lasting for few minutes noticed whenever she was carried on the back and the left side of the chest is compressed and also during play when she is being hit or pushed on the chest. She was a product of full-term gestation and pregnancy was not supervised. The pregnancy and delivery were not adversely eventful. The child was the fourth of the mother's five children in a polygamous family setting of a non-consanguineous marriage. There was no family history of congenital anomalies.
Examination findings revealed a girl with normal growth parameters and good mental status. She had an actively discharging tract at the region of the angle of the left mandible which was about 2 cm below the left earlobe [Figure 1]. A rudimentary accessory nipple was seen on the left side with depression of the left hemithorax. Pectoralis major muscle, the third, fourth and fifth ribs were absent on the left side [Figure 2]; the left scapula was hypoplastic and displaced upward [Figure 3], but the left latissimus dorsi was well preserved. No limbs abnormalities were seen. She had normal cardiovascular examination findings.
Figure 1.

The opening of the esophago-cutaneous fistula
Figure 2.

Left anterior chest wall defect with hypoplastic, displaced left nipple
Figure 3.

Posterior view of the patient showing hypoplastic displaced left scapula
She had a chest radiograph which showed absence of the left 3rd, 4th and 5th ribs [Figure 4]. Abdominal ultrasound, electrocardiogram and echocardiogram were normal. A diagnosis of Poland syndrome, esophago-cutaneous fistula and recurrent cardiac syncope was made. The patient and parents were counseled, and she is awaiting reconstructive surgery for the chest defect.
Figure 4.
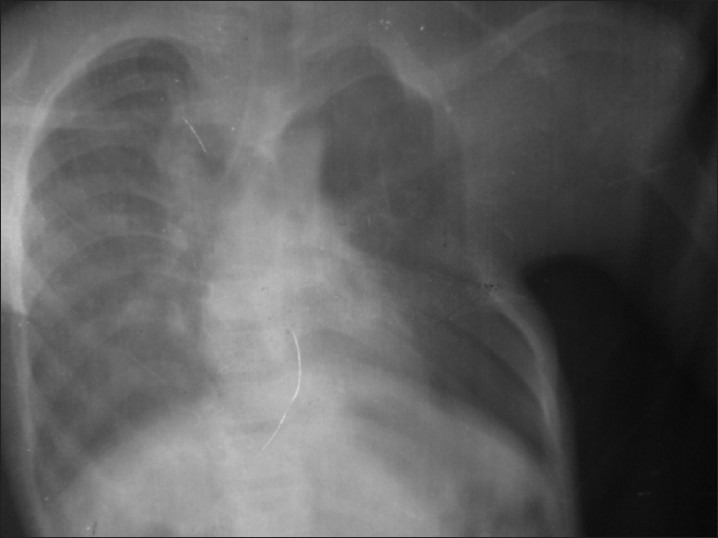
Chest X-ray showing left side anterior chest wall deformity with absent 3rd, 4th and 5th ribs
Discussion
Poland syndrome was first described in 1840 by Alfred Poland.[13] Geneticists currently hold the view that Poland syndrome is rarely inherited and generally occurs as a sporadic event; however, some authors have suggested an autosomal dominant pattern of inheritance.[14] It may occur in members of the same family.[14] However in our case, Poland syndrome occurred as a sporadic event. Although several theories have been advanced to explain the etiology of Poland syndrome, most evidence indicate that it results from a vascular event during the critical sixth week of gestation due to hypoplasia of the subclavian artery causing musculoskeletal malformations. The critical vascular event, known as subclavian artery supply disruption sequence (SASDS), occurs when the medial and forward growth of the ribs forces the subclavian vessel into a U-shaped configuration.[15]
Absence of the pectoralis major muscle is usually unilateral and almost always observed on the right side. In our case the defect was on the left side which is a rare occurrence. Gashegu et al.[12] in their case report also documented a left-sided defect. Poland syndrome often has associated abnormalities of the ribs ranging from hypoplasia to complete absence of the ribs.[16] Syndactyly is often a common association in Poland syndrome but was absent in this case, but she had an esophago-cutaneous fistula which was responsible for the discharging secretions.
Absence of the left third, fourth and fifth ribs in our patient may explain the recurrent syncopal attacks following blunt innocuous trauma to the left side of chest. This may be attributed to possible cardiac arrhythmia induced by the effect of the impact on the heart. This dysrhythmia could result in cardiac syncope or in severe cases commotio cordis. Commotio cordis is a nearly universally fatal condition that follows blunt non-penetrating trauma to the chest (e.g., from a baseball or hockey puck). It is commonly seen in young male athletes and so far there is no documented association with Poland syndrome. Occasionally, innocent-appearing chest blows incurred at home or at a playground may be fatal. Patients often experience immediate ventricular fibrillation that may be fatal. Though our patient always regained consciousness spontaneously, this made commotio cordis unlikely. However some commotio cordis events may abort spontaneously, especially when the blow causes a non-sustained arrhythmia, though this may be difficult to confirm if it occurs as an unwitnessed event; such cases have been recorded in the Minneapolis registry. This results in a slow pulse suggesting a transient complete heart block (or another bradyarrhythmia), as has been reported in laboratory settings, in which a blow to the chest is timed to occur during the QRS complex.[17,18]
Conclusion
We have therefore reported Poland syndrome in an eight-year-old Nigerian girl, a rare congenital anomaly that involved the left anterior chest, which is also an uncommon site of involvement that predisposed the child to an unusually cardiac manifestation of recurrent loss of consciousness following episodes of innocuous trauma to the chest.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Friedman T, Reed M, Elliot AM. The carpal bones in Poland syndrome. Skeletal Radiol. 2009;38:585–91. doi: 10.1007/s00256-008-0638-x. [DOI] [PubMed] [Google Scholar]
- 2.Ferraro GA, Perrotta A, Rossano F, D’Andrea F. Poland syndrome: Description of an atypical variant. Aesth Plast Surg. 2005;29:32–3. doi: 10.1007/s00266-004-0047-z. [DOI] [PubMed] [Google Scholar]
- 3.Garcìa CC, Castilla AN, Jiménez EL, Garcìa IA. Dextrocardia associated with left-sided Poland syndrome. Am J Phys Med Rehabil. 2009;88:168. doi: 10.1097/PHM.0b013e318197e819. [DOI] [PubMed] [Google Scholar]
- 4.Moir CR, Johnson CH. Poland's syndrome. Semin Pediatr Surg. 2008;17:161–6. doi: 10.1053/j.sempedsurg.2008.03.005. [DOI] [PubMed] [Google Scholar]
- 5.Baban A, Torre M, Bianca S, Buluggiu A, Rossello MI, Calevo MG, et al. Poland syndrome with bilateral features: Case description with review of the literature. Am J Med Genet. 2009;149:1597–602. doi: 10.1002/ajmg.a.32922. [DOI] [PubMed] [Google Scholar]
- 6.Stevens DB, Fink BA, Prevel C. Poland's syndrome in one identical twin. J Pediatr Orthop. 2000;20:392–5. [PubMed] [Google Scholar]
- 7.Fraser FC, Teebi AS, Walsh S, Pinky L. Poland sequence with dextrocardia: Which comes first? Am J Med Genet. 1997;73:194–6. doi: 10.1002/(sici)1096-8628(19971212)73:2<194::aid-ajmg16>3.0.co;2-l. [DOI] [PubMed] [Google Scholar]
- 8.Smith DW. Philadelphia: WB Saunders Company; 1982. Poland sequence (Unilateral defect of pectoralis muscle and syndactly of hand) pp. 224–7. [Google Scholar]
- 9.Uster GD. Upper extremity. In: Mustarde’ JC, Jackson IT, editors. Plastic surgery in infancy and childhood. Edinburgh: Churchill Livingstone; 1988. pp. 565–7. [Google Scholar]
- 10.Lagbo JN. Poland syndrome: Report of a variant. J Natl Med Assoc. 2006;98:97–9. [PMC free article] [PubMed] [Google Scholar]
- 11.Hamidu AU, Musa A, Tahir MC. Poland's syndrome: An incidental finding at routine medical examination. Nig J Surg Res. 2006;8:97–8. [Google Scholar]
- 12.Gashegu J, Byiringiro JC, Nyundo M, Uwineza A, Mutesa L. Poland syndrome: A case report. East Cent Afr J Surg. 2009;14:112–5. [Google Scholar]
- 13.Upton J. Congenital anomalies of the hand forearm. In: McCarthy JG, editor. Plastic surgery. Philadelphia: WB Saunders Company; 1990. pp. 5301–5. [Google Scholar]
- 14.Darian VB, Argenta LC, Pasyk KA. Familial Poland's syndrome. Ann Plast Surg. 1989;23:531–7. doi: 10.1097/00000637-198912000-00010. [DOI] [PubMed] [Google Scholar]
- 15.Bavinck JN, Weaver DD. Subclavian artery supply disruption sequence: Hypothesis of a vascular etiology for Poland, Klippel-Feil, and Moebius anomalies. Am J Med Genet. 1986;23:903–18. doi: 10.1002/ajmg.1320230405. [DOI] [PubMed] [Google Scholar]
- 16.Gocmen H, Akkas Y, Doganay S. Poland syndrome: Rare presentation in two cases. JN ZMed Assoc. 2010;123:71–7. [PubMed] [Google Scholar]
- 17.Link MS, Wang PJ, Pandian NG, Bharati S, Udelson EJ, Man-Young L, et al. An experimental model of sudden death due to low-energy chest-wall impact (commotio cordis) N Engl J Med. 1998;338:1805–11. doi: 10.1056/NEJM199806183382504. [DOI] [PubMed] [Google Scholar]
- 18.Maron BJ, Pelliccia A. The heart of trained athletes: Cardiac remodeling and the risks of sportsincluding sudden death. Circulation. 2006;114:1633–44. doi: 10.1161/CIRCULATIONAHA.106.613562. [DOI] [PubMed] [Google Scholar]