

Abstract
Rising stroke and higher mortality among Indian population needs focused attention for prevention and early management of stroke. In India, very few studies have been carried out to determine the causes of deficiencies in knowledge, attitude and practice (KAP) of stroke among Indians. Study on KAP is essential to improve the awareness about stroke, early diagnosis and institution of appropriate management. In this article, we have reviewed the existing literature on this issue and tried to compare it with those of developed countries and suggested the measures we need to adopt in India to improve awareness and knowledge base.
Key Words: Awareness, risk factors, prevention strategies, stroke, India
Introduction
Globalization and industrialization witnessed over the last two decades have influenced life-styles of people particularly in developing countries. In addition, demographic transitions have added non-communicable diseases with existing communicable ones, thus causing double burden of diseases. Stroke is a major non-communicable disease. It is the most common cause of mortality and a significant cause of adult disability.[1,2] Stroke may also compromise cognitive, mood, functional abilities and quality-of-life.[3,4,5,6,7] It also results in caregiver burden[4] and economic stress at individual,[4] familial and national level. In India, current data suggests that each year approximately 1.5 persons per1000 subjects are developing stroke and approximately upto 41.08% (male, 38.18%; women, 43.24%) of stroke victims may die following acute stroke.[1] Thus, from the current Indian population of about 1.2 billion, approximately 1.8 million people may suffer from stroke annually and about one-third of them may die. This entails the issue of prevention and treatment of stroke serious attention for developing countries.[8]
Treatments of acute ischemic stroke with thrombolytics can reverse the acute paralysis in many patients.[9,10] However, such therapeutic opportunities can be utilized only within the window period of four and half hours with good infrastructural support; such expenditure being quite high too. For maximum utilization of thrombolysis within the golden time period, the identification of stroke-sufferers and knowledge of the treating physician as well as that of the general mass is absolutely essential. It is deemed wiser to focus attention on preventive measures considering the limitation of infrastructure and magnitude of the problem.
General knowledge (K) about stroke improves quick and correct identification and adds to the body of technical knowledge. Attitude (A) or outlook toward stroke is affected by the knowledge along with the practices (P) undertaken by people to prevent and treat stroke. Accurate knowledge of stroke risk factors and warning signs, right attitude and proper practices of stroke prevention or the immediate action that is necessary in dealing with a stroke patient can arrest both mortality and morbidity among the public. Thus, to check high stroke mortality in developing countries particularly in India, it is essential to prevent delay in hospitalization, which is primarily caused due to ignorance about stroke, incorrect attitude and poor infrastructure.[11]
It is important to review public awareness regarding existing knowledge, attitude and practices (KAP) to prevent mortality-morbidity of stroke in the community. In case of inadequate knowledge among the mass, governmental and non-governmental efforts to empower the mass with adequate knowledge, effective practice and the right attitude may help reach this objective. Against this background, this review article attempts to summarize and compare people's perception of stroke across nations and highlight the recommendations for stroke-prevention strategies put forward by standard guidelines for the general mass.
Studies on KAP
Studies conducted globally
Studies on KAP have mostly been undertaken in developed countries across all continents, assessing hospital-based patients or similar set-ups, or community-dwellers through house-to-house survey.[12,13,14,15,16,17,18,19] The Asian studies have also been mainly undertaken in the developed countries such as South Korea and Hong Kong.[17,18] Studies conducted in developing countries have been limited in few countries such as Brazil, Iran, Oman, Pakistan and India across continents.[20,21,22,23,24,25]
No operational definition of knowledge, attitude or practice has been provided in any of the publications. Addressing this topic, researchers have explored the issues of risk factors in stroke, warning symptoms, source of knowledge and practices undertaken by community-dwellers. Through statistical means, authors have looked into associations between the above parameters and demographic details of the participants. Based upon their findings, the authors have attempted to provide effective suggestions applicable for their respective populations.
Methodological differences between studies
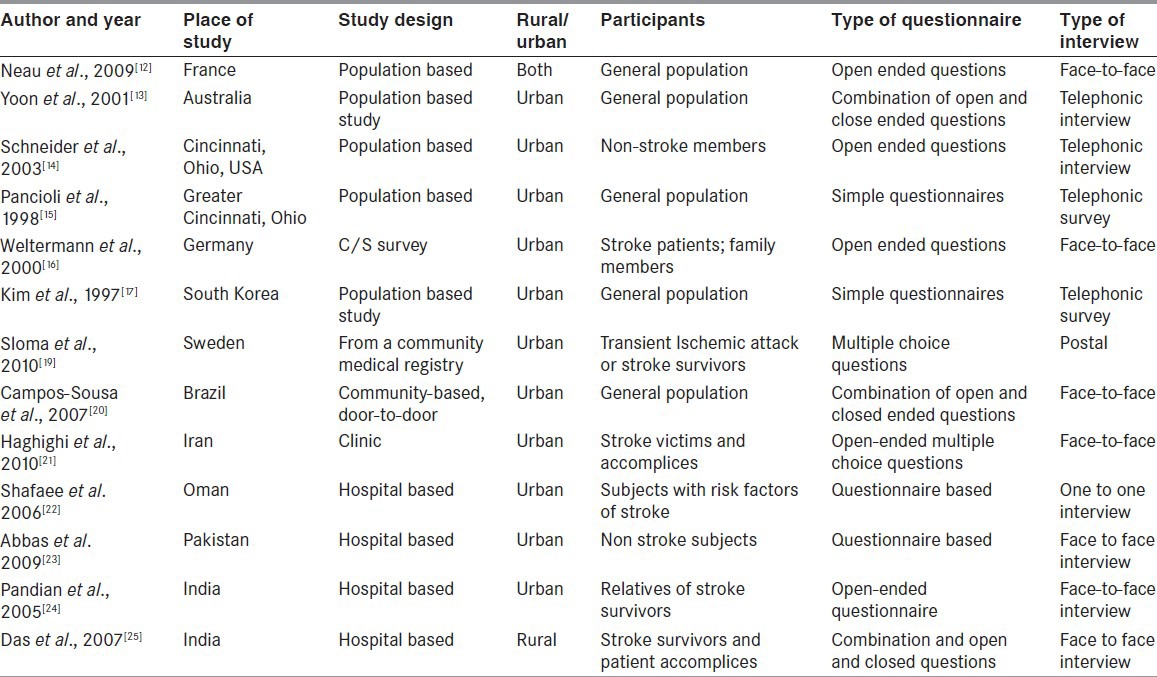
The questionnaires employed and the interview patterns vary amongst studies [Table 1]. Discrepancies between studies depend to a great extent upon the type of interview: face-to-face interview[12,16,20,21,23,24,25] telephonic[13,14,15,17,18] or postal surveys;[19] upon the type of questionnaires employed: open-ended[12,14,16,21,24] combination of open and closed-ended questionnaires[13,20,25] or ticking potential responses/multiple-choice-questions[19] and simple questions testing the knowledge of the respondent.[15,17,18,25]
Table 1.
Study methodologies undertaken to explore knowledge, attitude and practice of stroke
Sites of involvement
Majority of respondents [Table 1] in the studies comprising of stroke-survivors, relatives of stroke survivors and non-stroke participants, identified “brain” as the affected area in stroke[12,13,16,26] with some demonstrating very poor knowledge,[24] followed by a very few who believed that stroke was a heart problem.[12,13]
Risk factors
A number of studies have assessed knowledge of stroke among the general population across different nations. Studies have documented predominantly inadequate knowledge about stroke risk factors and stroke warning signs among their respective participants globally [Table 1].
It is alarming to learn that knowledge about stroke risk factors (hypertension [HTN], smoking, alcohol, diabetes, ischemic heart disorder, atrial fibrillation) is observed to be poorest among those with the highest risk for stroke.[16] Further, studies on stroke or transient ischemic attack patients have indicated poor knowledge about risk factors when evaluated a few months after stroke[27,28] and also among patients undergoing rehabilitation.[29]
Different studies show different risk factor knowledge as provided in Table 2. Highest response rate was observed among Australians followed by Germans, Indians and Brazilians.[13,16,20,24] Respondents from USA showed variable knowledge about risk factors.[15,30]
Table 2.
Awareness about risk factors in different countries
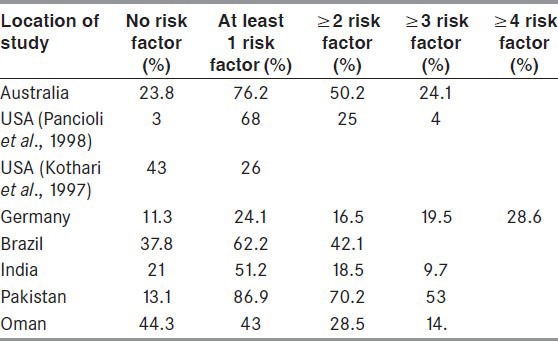
HTN[14,15,18,19,20,21,24,25,31] and smoking[13,14,17,19,21] are identified as the common risk factors globally by participants. Alcohol consumption is identified as a risk factor by responders across different developed and developing countries with American responders ascribing a marginal role.[12,14,25] Poor understanding of diabetes as a risk factor is a common documentation.[31,32] Not even half of the Swedish participants recognized ischemic heart disease and diabetes as a major risk factor[19] and a still lesser number of American and French participants reported the same.[12,14] However, contrarily, Indian stroke-survivors as well as non-stroke healthy people identify diabetes as an important factor.[25] Atrial fibrillation was identified as an important factor by almost half of the Swedish subjects; however, those who recognized the symptom had experience with the condition.[19] Vascular rupture was cited as the third most important factor only by the Iranians[21] after HTN and smoking. Life-style related factors were commonly listed as risk factors by Swedish stroke-survivors and non-stroke participants.[19] High cholesterol and wrong diet were seldom documented as important risk factors except a few studies.[12,14] Researchers report better knowledge of a specific risk factor among those affected by it, which could be resultant of frequent contacts with medical personnel for regular monitoring and treatment.[12,14]
A Swedish study report only 62% of the stroke-survivors to be aware that a previous episode of stroke was a risk factor.[19] It is important to note that stroke-survivors or those at risk were observed to have poorer knowledge than non-stroke individuals.[16,19,33]
Summing up the global view, it is revealed that major population-based studies report HTN to be the most established stroke risk factor cited by 45-89.7% of respondents from India[24] Hong Kong[18] Australia[13] and USA.[14] However, HTN, smoking and alcohol are also documented by some as less important risk factors for stroke.[13,15,17,34] Interestingly, individuals in both developed and developing countries perceive psychological stress to be a risk factor for stroke.[13,15,19,24]
Psychological stress as a risk factor is well-established in coronary heart disease. However, literature is scanty on the relationship of stroke and psychological stress.[35,36] A case-control study conducted in a developed country reveals an independent association of self-perceived psychological stress and ischemic stroke.[36] Hence, additional research in this area is necessary to bring clarity to this association.
Warning symptoms
Studies reveal that knowledge about warning symptoms is worse among people in comparison with their knowledge about risk factors. A French study reported poor knowledge about stroke warning signs among its participants, although their knowledge about risk factors was moderate[12] and is depicted in Table 3. About half of the French respondents were able to recognize one or more stroke warning signs. The study from Brazil revealed that 41.1% of respondents had no knowledge about warning symptoms.[20] Similar study in Australia[13] revealed that 23.8% of the respondents could not figure out any warning symptoms and the rest could point to some as depicted in Table 3.
Table 3.
Awareness about warning symptoms
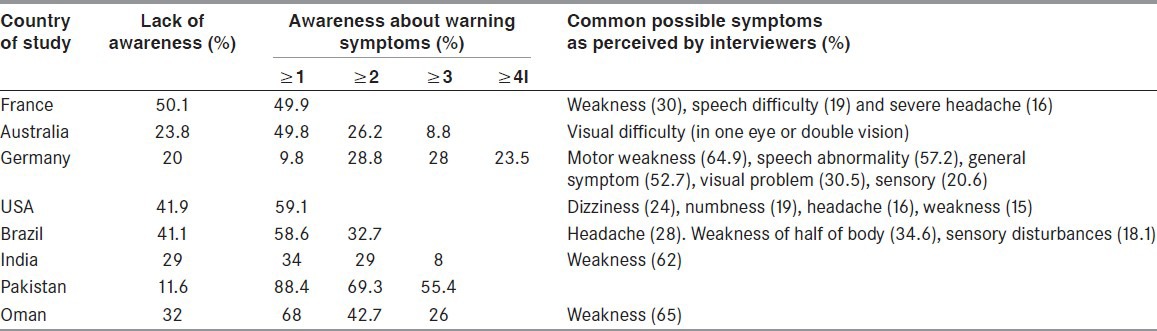
Very few Indians could correctly list stroke warning signs.[24,25] The Indian study documents 23% of its participants to be ignorant about stroke warning symptoms and the rest responded to various warning symptoms[24] as provided in Table 3. Many Indian patients reported that they were confused at the initial stage of stroke owing to the variable presentation of stroke symptoms, particularly when symptoms were headache, unilateral numbness, dizziness, visual and speech problems. Symptoms referable to carotid artery stroke such as hemiparesis are easily recognized as compared with posterior circulation stroke.[17,18,34]
Two studies exploring the knowledge about stroke risk factors and warning symptoms were undertaken in USA through telephonic interviews over a temporal difference of 5 years.[14,15] The only significant evolution was observed to be the knowledge of stroke symptoms.[14] However, the underlying reason for this enhancement of knowledge could be attributed to divulgence of information on stroke-symptoms in the media due to the approval of tissue plasminogen activator for acute treatment of stroke by the “Federal drug agency.”
Source of knowledge
The most frequently cited sources of knowledge about stroke among Americans[14] was employing mass media such as television (32%), magazines (24%) and newspapers (22%). Other sources of information were physicians, family member with stroke, medical books and information from friends who were stroke-survivors. The French,[12] Indians[24,25] and Australians[13] indicated the sources of knowledge from print and electronic media were superior rather than professionals (physicians, pharmacists or hospital information). However, the younger respondents were eager to get information through the internet. The role of doctors and health personnel in delivering such knowledge in Indian society remains unsatisfactory. Government or non-government organizations also played a limited role in disseminating knowledge of stroke among public.[25] Good knowledge about stroke was correlated with sources of information (books, magazines, newspapers).[12]
A study on community education on stroke awareness has shown that that information on stroke can be successfully increased by using media including television, magazines and newspapers as well as family and friends followed by health professionals and educational campaigns.[37] However, it remains unclear how intensive such campaigns should be and how frequently they should be repeated.[38].
Attitude and practice
Attitude toward stroke has been an almost unexplored area of research. Americans[14] and French[12] are more inclined to call their emergency services if they witnessed or suffered from a stroke. Call to the emergency services is the first option among 88% and 75% of French and American citizens, respectively. Similarly, few other studies[24,26,34] prefer to take their patients to the hospital emergency department in contrast to Koreans who are documented to prefer herbal medicine and other traditional methods of treatment.[17]
Most of the participants in an Iranian study believed that treatment of stroke is difficult and expensive that neither hospitals were suitable for stroke patients, nor Neurologists were available.[21] Among them, 89% reported that controlling blood pressure can prevent stroke, 8% did not have any information regarding it and only 3% reported that controlling blood pressure cannot prevent stroke. Nearly, 96% of Iranian participants want to be treated by a neurologist.
A large portion (93.6%) of Brazilian[20] and English[39] (96%) participants opined immediate treatment of stroke to be extremely important. They acknowledged the importance of issues such as early hospitalization and therapeutic intervention within the window period.
Among the Australians, 21% of respondents described “blood-clot-dissolving drug or blood-thinning drugs” and 12.1% of respondents described “blood pressure control, surgery, heart massage, other medications and natural therapies” as appropriate therapies for treating stroke. The rest could not identify any of these therapies.[13] Drug compliance related to antiplatelets and anticoagulants is very high among Swedish participants and only 3% do not take drugs.[19]
Indian participants were observed to hold an attitude that stroke could occur without any risk factors, simply being an event associated with senility[24] and hence consultation with health personnel was reportedly low. About more than half of the study participants reported that they did not know the appropriate treatment for stroke.[24] Approximately, 10.7% believed in indigenous modalities such as oil massage, faith healing and magic. This is suggested to be an underestimation by the authors since the study could not capture the rural population, where indigenous practices are expected to be higher due to lack of education, inadequacy of health infrastructure and awareness.
Role of social support groups
A study on social support groups of stroke from Germany reveal good symptom knowledge to be significantly more among those participants who are equal or less than 70 years than older patients, those with self-reported health status of good or fair quality, non-stroke participants and those with additional stroke education.[16] Members of stroke support groups exhibit greater knowledge and are well-informed about all aspects of modern stroke care than non-members.[16] The authors opine that the difference cannot be attributed to cultural or differences in the medical system, but that it may reflect a difference due to stroke experience.
Association of stroke risk factors and warning symptoms with study demography
Age
Variable knowledge about stroke risk factors and warning symptoms was associated with different age groups in different countries. Younger age predicted better knowledge in a community-based Australian study.[13] German participantsobserved good symptom and risk factor knowledge in subjects with ≤ 70 years of age.[16] Brazilian participants between 40 and 55 years were associated with more knowledge regarding stroke risk factors.[20] Americans also showed better knowledge about risk factors among persons aged ≤ 65.[30]
Education
Diverse information emerges regarding the relationship of education and knowledge about stroke. Majority of the studies do not find any association between educational level and knowledge of stroke risk factors and signs[12,18,21,37,40,41,42] while some studies observe significant association of higher education with better knowledge.[13,15,24,25] Brazilians are observed to put up with more knowledge among those educated until 12th standard.[20]
Gender
Female gender predicted better knowledge about stroke risk factors among Australians[13] and Americans,[15] but the reverse is common among Indians.[24] However, another study from USA did not observe any gender related differences in knowledge.[40]
Preventive Strategies
The spread of knowledge about stroke risk factors and warning signs is deemed important to prevent stroke morbidity and fatality. Most of the studies attempting to evaluate KAP about stroke did not undertake programs on preventive measures, but provided their own expert opinion,[12,24] recommendations put forward by their participants[14,31] and made suggestions from other studies undertaking such interventions.[20]
Accumulating studies in this area suggest community educational programs employing different media to play an important role in enhancing awareness. It has been shown that increasing stroke knowledge with means of public and professional education resulted in a shorter time of presentation to the emergency department following stroke onset.[43] Awareness about stroke significantly increased after informative campaigns.[37,30,44] Community stroke education holds the prospect to reduce delays in hospitalization and referral of stroke patients.[11,30,40] Significant improvement in awareness has resulted from educational campaign based on the television program in the community.[37,44] Hence, researchers propose the application of this method as a preventive measure.[14,45] Print media such as newspapers, books and magazines is often reported[37,43,45] to serve as an equally important source for creating awareness about stroke.
Based upon the information that members from the stroke-affected families are an important source of information, it could be useful to utilize the knowledge and experience of stroke survivors and their relatives to create awareness among the public in general and specifically the people at risk.[12,37] Participants in an Indian study also made a similar recommendation. Simultaneously, they emphasized the importance of improving the general education level.[25]
Common people also have reliance on physicians’ information.[14] Thus, multiple strategies to reinforce knowledge may be useful through verbal, written and other visual information and repeated educational encounters. Particularly, radio broadcasting is very important source of knowledge for the rural folk particularly in those inaccessible areas and without electricity. The role of physicians and health personnel are also important because of the reliance of the citizens on them as part of counseling to patients and their attendants when they get admitted and come for follow-up in addition to handing over an information leaflet on stroke preventions.
Public education promoting awareness of the seriousness of stroke, the urgency of stroke evaluation and the narrow therapeutic time window may lead toward changes in behavior and attitude of the public in general. Improved knowledge and changed attitude will advance the practice of stroke management, thereby reducing the burden of stroke in India and also developing countries. Thus, continued and intensified educational efforts to promote knowledge of stroke, particularly among high-risk groups, are needed by policymakers, as well as local and national organizations.
Footnotes
Source of Support: Nil
Conflict of Interest: Nil
References
- 1.Das SK, Banerjee TK, Biswas A, Roy T, Raut DK, Mukherjee CS, et al. A prospective community-based study of stroke in Kolkata, India. Stroke. 2007;38:906–10. doi: 10.1161/01.STR.0000258111.00319.58. [DOI] [PubMed] [Google Scholar]
- 2.Murray CJ, Lopez AD. Mortality by cause for eight regions of the world: Global burden of disease study. Lancet. 1997;349:1269–76. doi: 10.1016/S0140-6736(96)07493-4. [DOI] [PubMed] [Google Scholar]
- 3.Das S, Paul N, Hazra A, Ghosal M, Ray BK, Banerjee TK, et al. Cognitive dysfunction in stroke survivors: A community-based prospective study from Kolkata, India. J Stroke Cerebrovasc Dis. 2012 doi: 10.1016/j.jstrokecerebrovasdis.2012.03.008. DOI: 10.1016/03.008 PII: S1052-3057 (12) 00084-5. [DOI] [PubMed] [Google Scholar]
- 4.Das S, Hazra A, Ray BK, Ghosal M, Banerjee TK, Roy T, et al. Burden among stroke caregivers: Results of a community-based study from Kolkata, India. Stroke. 2010;41:2965–8. doi: 10.1161/STROKEAHA.110.589598. [DOI] [PubMed] [Google Scholar]
- 5.Gupta A, Pansari K, Shetty H. Post-stroke depression. Int J Clin Pract. 2002;56:531–7. [PubMed] [Google Scholar]
- 6.Lenzi GL, Altieri M, Maestrini I. Post-stroke depression. Rev Neurol (Paris) 2008;164:837–40. doi: 10.1016/j.neurol.2008.07.010. [DOI] [PubMed] [Google Scholar]
- 7.Sturm JW, Donnan GA, Dewey HM, Macdonell RA, Gilligan AK, Srikanth V, et al. Quality of life after stroke: The North East Melbourne stroke incidence study (NEMESIS) Stroke. 2004;35:2340–5. doi: 10.1161/01.STR.0000141977.18520.3b. [DOI] [PubMed] [Google Scholar]
- 8.Dalal PM, Bhattacharjee M. Stroke epidemic in India: Hypertension-stroke control programme is urgently needed. J Assoc Physicians India. 2007;55:689–91. [PubMed] [Google Scholar]
- 9.Davis S, Lees K, Donnan G. Treating the acute stroke patient as an emergency: Current practices and future opportunities. Int J Clin Pract. 2006;60:399–407. doi: 10.1111/j.1368-5031.2006.00873.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bushnell CD, Goldstein LB. Physician knowledge and practices in the evaluation of coagulopathies in stroke patients. Stroke. 2002;33:948–53. doi: 10.1161/01.str.0000014583.17714.e0. [DOI] [PubMed] [Google Scholar]
- 11.Srivastava AK, Prasad K. A study of factors delaying hospital arrival of patients with acute stroke. Neurol India. 2001;49:272–6. [PubMed] [Google Scholar]
- 12.Neau JP, Ingrand P, Godeneche G. Awareness within the French population concerning stroke signs, symptoms, and risk factors. Clin Neurol Neurosurg. 2009;111:659–64. doi: 10.1016/j.clineuro.2009.05.015. [DOI] [PubMed] [Google Scholar]
- 13.Yoon SS, Heller RF, Levi C, Wiggers J, Fitzgerald PE. Knowledge of stroke risk factors, warning symptoms, and treatment among an Australian urban population. Stroke. 2001;32:1926–30. doi: 10.1161/01.str.32.8.1926. [DOI] [PubMed] [Google Scholar]
- 14.Schneider AT, Pancioli AM, Khoury JC, Rademacher E, Tuchfarber A, Miller R, et al. Trends in community knowledge of the warning signs and risk factors for stroke. JAMA. 2003;289:343–6. doi: 10.1001/jama.289.3.343. [DOI] [PubMed] [Google Scholar]
- 15.Pancioli AM, Broderick J, Kothari R, Brott T, Tuchfarber A, Miller R, et al. Public perception of stroke warning signs and knowledge of potential risk factors. JAMA. 1998;279:1288–92. doi: 10.1001/jama.279.16.1288. [DOI] [PubMed] [Google Scholar]
- 16.Weltermann BM, Homann J, Rogalewski A, Brach S, Voss S, Ringelstein EB. Stroke knowledge among stroke support group members. Stroke. 2000;31:1230–3. doi: 10.1161/01.str.31.6.1230. [DOI] [PubMed] [Google Scholar]
- 17.Kim JS, Yoon SS. Perspectives of stroke in persons living in Seoul, South Korea. A survey of 1000 subjects. Stroke. 1997;28:1165–9. doi: 10.1161/01.str.28.6.1165. [DOI] [PubMed] [Google Scholar]
- 18.Cheung RT, Li LS, Mak W, Tsang KL, Lauder IJ, Chan KH, et al. Knowledge of stroke in Hong Kong Chinese. Cerebrovasc Dis. 1999;9:119–23. doi: 10.1159/000015909. [DOI] [PubMed] [Google Scholar]
- 19.Sloma A, Backlund LG, Strender LE, Skånér Y. Knowledge of stroke risk factors among primary care patients with previous stroke or TIA: A questionnaire study. BMC Fam Pract. 2010;11:47. doi: 10.1186/1471-2296-11-47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Campos-Sousa RN, Soares VY, Almeida KJ, Carvalho LI, Jacobina KS, Athayde Netto AE, et al. Knowledge of stroke among a Brazilian urban population. Arq Neuropsiquiatr. 2007;65:587–91. doi: 10.1590/s0004-282x2007000400007. [DOI] [PubMed] [Google Scholar]
- 21.Haghighi AB, Karimi AA, Amiri A, Ghaffarpasand F. Knowledge and attitude towards stroke risk factors, Warning symptoms and treatment in an Iranian population. Med Princ Pract. 2010;19:468–72. doi: 10.1159/000320306. [DOI] [PubMed] [Google Scholar]
- 22.Shafaee MaA. Ganguly SS, Asdmi ARA. Perception of stroke and knowledge of potential risk factors among Omani patients at increased risk for stroke. BMC Neurology. 2006;6(38) doi: 10.1186/1471-2377-6-38. doi: 10.1186/1471-2377-6-38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Abbas K, Irfan A, Sheikh R, Shakir M, Kazim SF, Aziz F, et al. Awareness of stroke risk factors, signs and treatment in a Pakistani Population. Journal of Pakistan Medical Association. 2009;59:2009. [PubMed] [Google Scholar]
- 24.Pandian JD, Jaison A, Deepak SS, Kalra G, Shamsher S, Lincoln DJ, et al. Public awareness of warning symptoms, risk factors, and treatment of stroke in northwest India. Stroke. 2005;36:644–8. doi: 10.1161/01.STR.0000154876.08468.a0. reference 23 and 24 shifted from reference-45 and 46. [DOI] [PubMed] [Google Scholar]
- 25.Das K, Mondal GP, Dutta AK, Mukherjee B, Mukherjee BB. Awareness of warning symptoms and risk factors of stroke in the general population and in survivors stroke. J Clin Neurosci. 2007;14:12–6. doi: 10.1016/j.jocn.2005.12.049. [DOI] [PubMed] [Google Scholar]
- 26.Parahoo K, Thompson K, Cooper M, Stringer M, Ennis E, McCollam P. Stroke: Awareness of the signs, symptoms and risk factors: A population-based survey. Cerebrovasc Dis. 2003;16:134–40. doi: 10.1159/000070593. [DOI] [PubMed] [Google Scholar]
- 27.Croquelois A, Bogousslavsky J. Risk awareness and knowledge of patients with stroke: Results of a questionnaire survey 3 months after stroke. J Neurol Neurosurg Psychiatry. 2006;77:726–8. doi: 10.1136/jnnp.2005.078618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Samsa GP, Cohen SJ, Goldstein LB, Bonito AJ, Duncan PW, Enarson C, et al. Knowledge of risk among patients at increased risk for stroke. Stroke. 1997;28:916–21. doi: 10.1161/01.str.28.5.916. [DOI] [PubMed] [Google Scholar]
- 29.Stein J, Shafqat S, Doherty D, et al. Patient knowledge and expectations for functional recovery after stroke. Aerican Journal of Physical Medicine Rehabilitation. 2003;82:591–596. doi: 10.1097/01.PHM.0000078197.34363.02. [DOI] [PubMed] [Google Scholar]
- 30.Kothari R, Sauerbeck L, Jauch E, Broderick J, Brott T, Khoury J, et al. Patients’ awareness of stroke signs, symptoms, and risk factors. Stroke. 1997;28:1871–5. doi: 10.1161/01.str.28.10.1871. [DOI] [PubMed] [Google Scholar]
- 31.Kraywinkel K, Heidrich J, Heuschmann PU, Wagner M, Berger K. Stroke risk perception among participants of a stroke awareness campaign. BMC Public Health. 2007;7:39. doi: 10.1186/1471-2458-7-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Maasland L, Koudstaal PJ, Habbema JD, Dippel DW. Knowledge and understanding of disease process, risk factors and treatment modalities in patients with a recent TIA or minor ischemic stroke. Cerebrovasc Dis. 2007;23:435–40. doi: 10.1159/000101468. [DOI] [PubMed] [Google Scholar]
- 33.Ferro JM, Canhão P, Peralta R. Update on subarachnoid haemorrhage. J Neurol. 2008;255:465–79. doi: 10.1007/s00415-008-0606-3. [DOI] [PubMed] [Google Scholar]
- 34.Reeves MJ, Hogan JG, Rafferty AP. Knowledge of stroke risk factors and warning signs among Michigan adults. Neurology. 2002;59:1547–52. doi: 10.1212/01.wnl.0000031796.52748.a5. [DOI] [PubMed] [Google Scholar]
- 35.Schneck MJ. Is psychological stress a risk factor for cerebrovascular disease? Neuroepidemiology. 1997;16:174–9. doi: 10.1159/000109684. [DOI] [PubMed] [Google Scholar]
- 36.Jood K, Redfors P, Rosengren A, Blomstrand C, Jern C. Self-perceived psychological stress and ischemic stroke: A case-control study. BMC Med. 2009;7:53. doi: 10.1186/1741-7015-7-53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Stern EB, Berman M, Thomas JJ, Klassen AC. Community education for stroke awareness: An efficacy study. Stroke. 1999;30:720–3. doi: 10.1161/01.str.30.4.720. [DOI] [PubMed] [Google Scholar]
- 38.Moser DK, Kimble LP, Alberts MJ, Alonzo A, Croft JB, Dracup K, et al. Reducing delay in seeking treatment by patients with acute coronary syndrome and stroke: A scientific statement from the American heart association council on cardiovascular nursing and stroke council. Circulation. 2006;114:168–82. doi: 10.1161/CIRCULATIONAHA.106.176040. [DOI] [PubMed] [Google Scholar]
- 39.Morgan LJ, Chambers R, Banerji J, Gater J, Jordan J. Consumers leading public consultation: The general public's knowledge of stroke. Fam Pract. 2005;22:8–14. doi: 10.1093/fampra/cmh709. [DOI] [PubMed] [Google Scholar]
- 40.Howard VJ, Lackland DT, Lichtman JH, McClure LA, Howard G, Wagner L, et al. Care seeking after stroke symptoms. Ann Neurol. 2008;63:466–72. doi: 10.1002/ana.21357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Williams LS, Bruno A, Rouch D, Marriott DJ. Stroke patients’ knowledge of stroke. Influence on time to presentation. Stroke. 1997;28:912–5. doi: 10.1161/01.str.28.5.912. [DOI] [PubMed] [Google Scholar]
- 42.Greenlund KJ, Neff LJ, Zheng ZJ, Keenan NL, Giles WH, Ayala CA, et al. Low public recognition of major stroke symptoms. Am J Prev Med. 2003;25:315–9. doi: 10.1016/s0749-3797(03)00206-x. [DOI] [PubMed] [Google Scholar]
- 43.Alberts MJ, Perry A, Dawson DV, Bertels C. Effects of public and professional education on reducing the delay in presentation and referral of stroke patients. Stroke. 1992;23:352–6. doi: 10.1161/01.str.23.3.352. [DOI] [PubMed] [Google Scholar]
- 44.Silver FL, Rubini F, Black D, Hodgson CS. Advertising strategies to increase public knowledge of the warning signs of stroke. Stroke. 2003;34:1965–8. doi: 10.1161/01.STR.0000083175.01126.62. [DOI] [PubMed] [Google Scholar]
- 45.Becker K, Fruin M, Gooding T, Tirschwell D, Love P, Mankowski T. Community-based education improves stroke knowledge. Cerebrovasc Dis. 2001;11:34–43. doi: 10.1159/000047609. [DOI] [PubMed] [Google Scholar]