

Abstract
Background:
Headache, musculoskeletal symptoms, and vitamin D deficiency are common in the general population. However, the interrelations between these three have not been delineated in the literature.
Materials and Methods:
We retrospectively studied a consecutive series of patients who were diagnosed as having chronic tension-type headache (CTTH) and were subjected to the estimation of serum vitamin D levels. The subjects were divided into two groups according to serum 25(OH) D levels as normal (>20 ng/ml) or vitamin D deficient (<20 ng/ml).
Results:
We identified 71 such patients. Fifty-two patients (73%) had low serum 25(OH) D (<20 ng/dl). Eighty-three percent patients reported musculoskeletal pain. Fifty-two percent patients fulfilled the American College of Rheumatology criteria for chronic widespread pain. About 50% patients fulfilled the criteria for biochemical osteomalacia. Low serum 25(OH) D level (<20 ng/dl) was significantly associated with headache, musculoskeletal pain, and osteomalacia.
Discussion:
These suggest that both chronic musculoskeletal pain and chronic headache may be related to vitamin D deficiency. Musculoskeletal pain associated with vitamin D deficiency is usually explained by osteomalacia of bones. Therefore, we speculate a possibility of osteomalacia of the skull for the generation of headache (osteomalacic cephalalgia?). It further suggests that both musculoskeletal pain and headaches may be the part of the same disease spectrum in a subset of patients with vitamin D deficiency (or osteomalacia), and vitamin D deficiency may be an important cause of secondary CTTH.
Key Words: Chronic daily headache, chronic musculoskeletal pain, chronic pain, chronic tension-type headache, osteomalacia, pain, vitamin D
Introduction
Chronic pain is a common symptom within the community, with an estimated prevalence up to 15%.[1] A number of studies have demonstrated a link between the chronic pain and hypovitaminosis D.[2] A recent cross sectional study demonstrated significantly low level of serum vitamin D in non-migraine headache.[3] A few case reports and small observations also suggest that hypovitaminosis D may be related with headache.[4,5,6,7] In a meta-analysis on the prevalence of headache, we noted an increasing prevalence with increasing latitude.[8] One possible explanation could be lower level of serum vitamin D at higher latitude.
There is a well-established link between the low serum vitamin D and musculoskeletal pain due to osteomalacia.[9] Earlier we reported eight patients with vitamin D insufficiency having symptoms of both osteomalacia and chronic tension-type headache (CTTH).[4]
Herein, in this retrospective study, we tried to look for the interrelations of CTTH with vitamin D deficiency and osteomalacia.
Materials and Methods
This study was conducted as a retrospective chart review of prospectively collected data of patients seen in the neurology department from January 2009 to November 2012. The study constitutes a consecutive series of adult patients (>18 years) who were diagnosed as having CTTH according to ICHD-II criteria (2nd edition of The International Headache Classification)[10] and were subjected to the estimation of serum vitamin D level.
In our previous observation,[4] we noted eight patients with CTTH who also had vitamin D deficiency and osteomalcia. We suggested that every patient with CTTH should be examined for muscle-aches, weakness (especially proximal), and bone tenderness.[4] Therefore, as a departmental policy, all patients with CTTH are routinely subjected to full medical history and detail musculoskeletal system examinations (especially for the muscle pain, muscle tenderness, bone tenderness, and muscle weakness). Sites of the musculoskeletal pain were recorded according to the American College of Rheumatology (ACR) criteria for chronic widespread pain (CWP).[11]
Clinical Examinations
Muscle palpation for muscle tenderness was carried out on three pericranial muscles and three extracephalic points. Pericranial muscles: (i) Anterior temporalis muscle, (ii) frontalis muscle, just above the supraorbital notch (iii) sub occipital muscles at the suboccipital fossa. Extra cephalic muscles: (i) Achilles tendon, 1 cm above the calacaneum, (ii) elbow, 2 cm distal to the lateral epicondyle, (iii) medial fat pad of the knee, proximal to the joint line. These points were in accordance with the literature.[12,13] Symmetrical muscles were palpated. Tenderness was rated on a scale from 0-3. The scoring was defined as follows: 0 = no visible facial reaction and denial of tenderness; 1 = no visible facial reaction but, verbal report of discomfort or mild pain; 2 = verbal report of painful tenderness with facial expression of discomfort; and 3 = marked grimacing or withdrawal, verbal report of marked painful tenderness. A Total Tenderness Score (TTS) was calculated for each patient by simple summation of the scores from the palpated muscle. As studies have not demonstrated any side-to-side differences, only measurements carried out on one side were taken into the account.[8]
A physical examination to elicit bone tenderness was also carried out. We applied firm pressure with the thumb or forefinger on the anterior tibia, and radius or ulna (as suggested by Holick).[14] To the best of our knowledge, the literature is silent regarding the grading of bone tenderness. Therefore, we graded bone tenderness as we rated tenderness for muscle and TTS for bone was calculated separately. The neurological examination was carried out in details with special focus for proximal muscle weakness. Patients having proximal muscle weakness were subjected to estimation of serum creatine phosphokinase (CPK) and electromyography (EMG) test. Further investigations and management decisions were made at the discretion of the treating physicians. The study did not require approval by the local ethics committee as per the local regulations for retrospective observation.
Exclusion criteria included: (a) CTTH-like headache with acute onset (to exclude new daily persistent headache); (b) patients with a history suggestive of migraine headache; (c) patients with medication overuse headache; (c) patients who were never subjected to neuroimaging; and (d) patients who received vitamin D supplementation in the past 4 weeks.
Vitamin D deficiency was defined as serum 25 (OH) D levels less than 20 ng/ml (as suggested by Holick).[15] Biochemical osteomalacia was determined according to Jenkins et al. criteria,[16] Bingham and Fitzpatrick criteria,[17] and McKenna et al. osteomalacic index.[18]
Statistics
Descriptive statistics for the clinical characteristics and laboratory values were tabulated for the entire study sample and separately for patients with serum 25(OH) D <20 ng/ml and >20 ng/ml. We compared the patients with vitamin serum 25(OH) D levels of <20 ng/ml with that of >20 ng/ml. Data are presented as percentages or as arithmetic mean with SD. Student's t-test was used to compare the continuous data. The Chi-square test with Yate's correction was used for categorical data.
To evaluate associations between serum 25(OH) D concentration and various clinical and laboratory variables, we used Pearson's correlation co-efficients and simple logistic regression (or scatter plot) as appropriate to the nature and distribution of the variables. We constructed a multiple linear regression model for serum 25(OH) D concentrations using all predictors of the interest, whether significant or not in the simple regression. The predictors of interest included clinical signs, age, gender, body mass index, smoking, seasonality, residence, education, and associated comorbid conditions (diabetes, hypertension, depression anxiety). Confounding relationships were evaluated by whether the co-efficient and statistical significance changed substantially when a suspected confounder was added or removed from the model. All P values were two-tailed, and a P < 0.05 was defined as statistically significant.
Results
We identified 87 patients with a diagnosis of CTTH. Eight patients were excluded as they were not subjected to serum vitamin D estimation. Three patients were excluded as they were never subjected to neuroimaging. Three patients were excluded because of the incomplete data entry. Two patients were further excluded as they received Vitamin D supplementation in the recent past. Finally, seventy-one patients with a diagnosis of CTTH were identified.
Epidemiological features
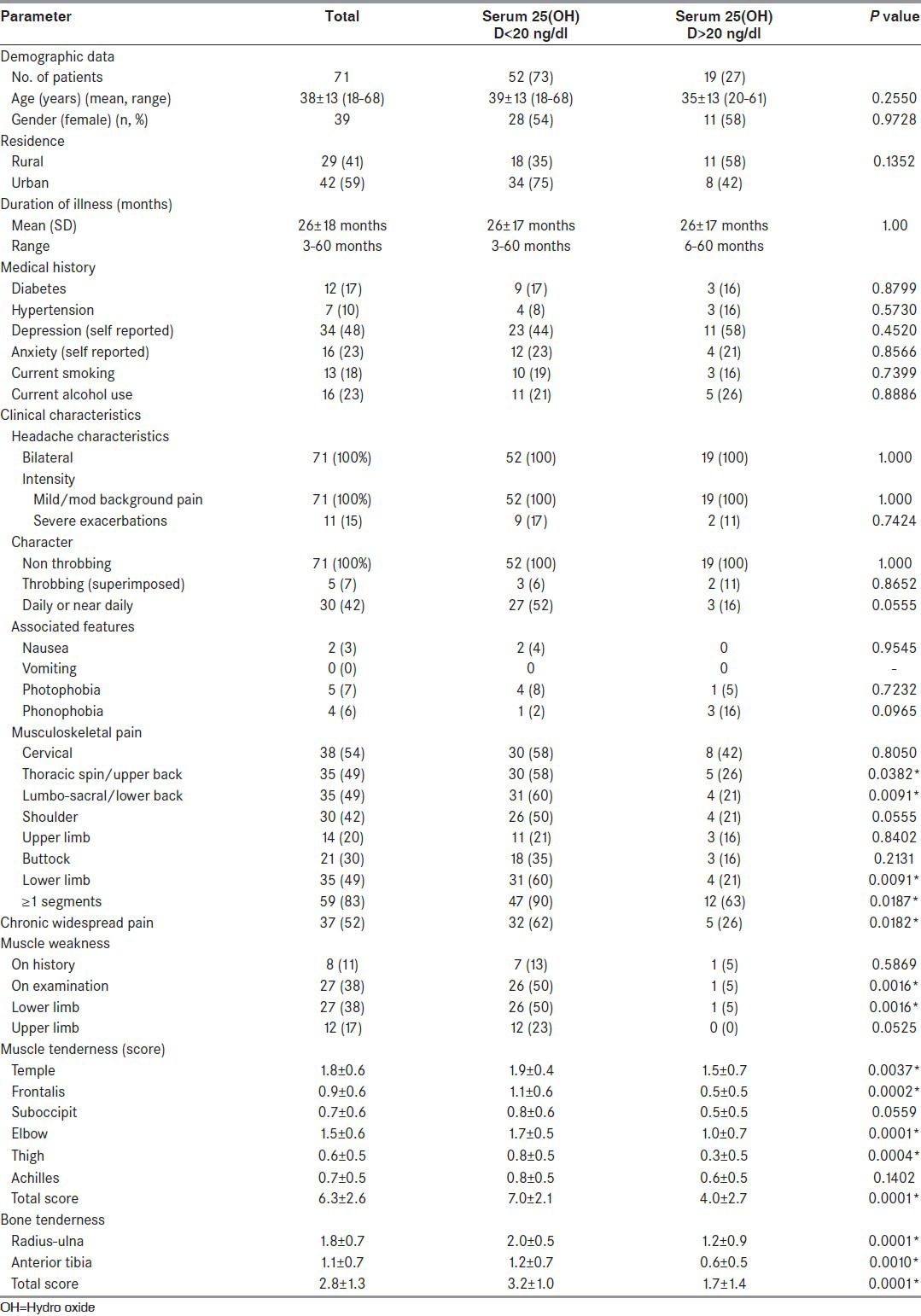
Descriptive statistics for clinical characteristics and laboratory values were tabulated for the entire study sample and separately for patients with serum 25(OH) D levels of <20 ng/ml and >20 ng/ml [Table 1]. The mean age of participants was 38 years, 55% were female. Seventy-three percent patients had low serum 25(OH) D level (<20 ng/ml). A comparison of patients with serum 25(OH) D levels of <20 ng/ml and ≥20 mg/ml was done. There were no significant differences between the groups with respect to age, gender, residence, smoking habit, alcohol habit, body mass index, duration of illness, and associated comorbid conditions (diabetes, hypertension, self-reported depression, and anxiety).
Table 1.
Descriptive data according to categories of 25 vitamin D
Clinical features
The headache characteristics (side, site, intensity, character, and associated nausea, photophobia, and phonophobia) were similar in both groups. Daily or near daily headache was more prevalent in patients with hypovitaminosis D (52% vs. 16%) (Statistically not significant) (P = 0. 0555).
Musculoskeletal pain was more prevalent in patients with hypovitaminosis D. Twenty-nine patients (56%) with hypovitaminosis D and 26% patients with serum vitamin D levels of > 20 ng/ml reported pain in multiple regions that satisfied the ACR criteria for CWP.[10] The difference between the groups were statistically significant (P < 0.0046). The pain was common at all sites (neck, upper back, lower back, shoulder, upper limb, buttock, and lower limbs) in patients with hypovitaminosis D. However, the differences were statistically significant for pain in the upper back (P = 0. 0382), lower back (P = 0. 0091) and lower limb pain (P = 0. 0091).
TTS was significantly higher in patients with hypovitaminosis D (P < 0.0001). Muscle tenderness score was higher in patients with CWP and this was statistically significant (P = 0. 0041). Bone tenderness was also significantly higher for patients with hypovitaminosis D.
Only 8 (11%) patients gave a history of limb weakness. However, on examination, weakness was noted in 27 (38%) patients in the total sample. The prevalence of proximal weakness was significantly higher in patients with hypovitaminosis D (50% vs. 5%; P = 0. 0016).
Investigations
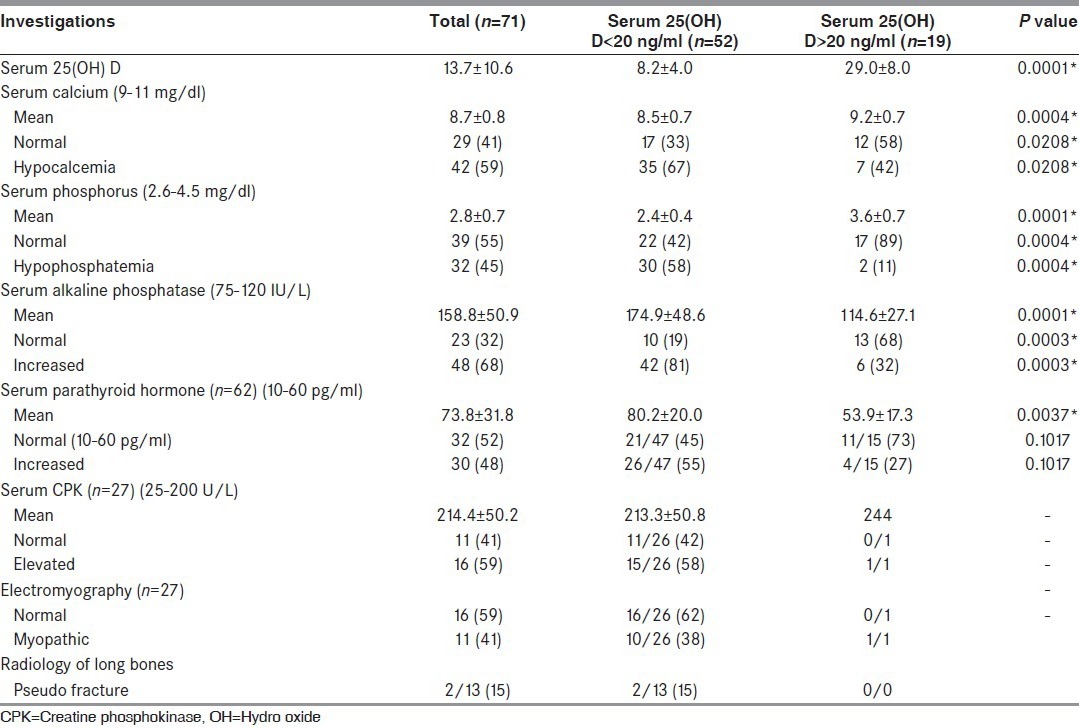
There were statistically significant differences in serum calcium, serum phosphate, and serum alkaline phosphatase (ALP) between the groups [Table 2]. Serum estimation for parathyroid hormone (PTH) was carried out for only 62 patients. Mean serum PTH levels were higher (statistically not significant) in patients with hypovitaminosis D. Patients having proximal weakness were subjected to estimation of serum CPK and EMG. Fifteen patients (58%) had a high serum CPK. Myopthic changes were noted in 10 patients. Thirteen patients were subjected to X-rays of long bones. Two patients demonstrated pseudo-fracture.
Table 2.
Biochemical and other laboratory abnormalities according to categories of serum 25 vitamin D
Evidence of osteomalacia
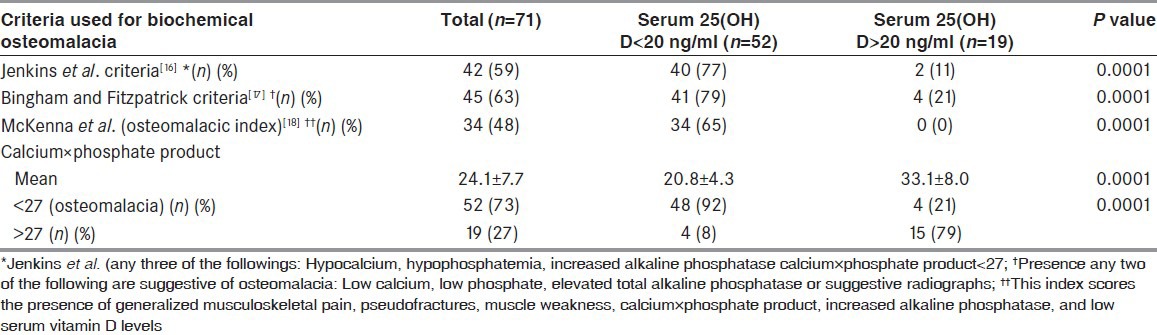
We used Jenkins et al. criteria,[16] Bingham and Fitzpatrick criteria[17] and McKeena et al.'s osteomalcic index[18] to determine the prevalence of the biochemical osteomalacia [Table 3]. A total of 48-63% patients (depending on the criteria used) had evidence of the biochemical osteomalacia. A significantly greater proportion of the patients in hypovitaminosis D group had biochemical osteomalacia.
Table 3.
Prevalence of biochemical osteomalacia according to various criteria
Subgroup analyses
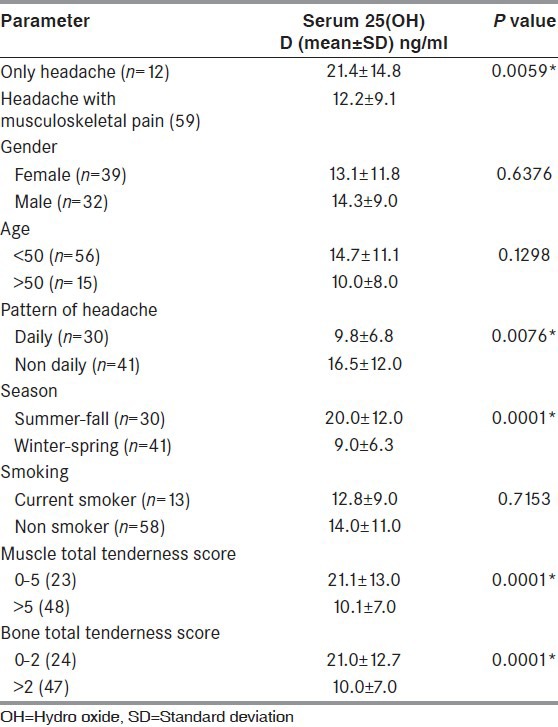
We divided the patients in various groups according to the epidemiological and the clinical features [Table 4]. There were no statistically significant differences in serum vitamin D levels (mean) according to age, gender, and smoking habit. However, the patients presented in winter – spring had significantly lower serum vitamin D levels. We compared patients having “headache only” with patients having both headache and musculoskeletal pain. Subjects with both “musculoskeletal pain and headache” had significantly lower mean 25(OH) D levels than those who have only headaches (12.2 vs. 21.4; P = 0. 0059). In the same line, patients having daily headache (9.8 vs 16.5; P = 0. 0076) had significantly lower serum vitamin D levels that those who had intermittent headaches. The patients with high muscle TSS and bone tenderness also had significantly lower mean 25(OH) D levels.
Table 4.
Subgroup analyses: Association of serum vitamin D levels with various subgroups of the patients
Correlation of serum vitamin D levels with various epidemiological, clinical, and biochemical parameters
Pearson's correlation co-efficient between vitamin D levels and various biochemical and the clinical parameters were calculated [Table 5]. It was found to be statistically significant for serum calcium (r = 0.687507; P < 0.0001), serum phosphorus (r = 0. 794581; P < 0.0001), serum ALP (r = −0.58277, P < 0.0001), calcium × phosphate product (r = 0.849417; P < 0.0001), osteomalacic index (r = −0.74444, P < 0.0001) muscle tenderness score (r = −76052; P < 0.0001) and bone tenderness (r = −76780; P < 0.0001). Scatter plot [Figure 1 and Figure 2] shows statistically significant negative correlation between serum 25(OH) D levels and osteomalacic index and TTS (muscle). In the multivariate linear regression analysis, estimated serum 25(OH) D levels were on average 9.6 ng/ml higher in summer than in other times of year (P = 0.0002). Other factors did not show any association with serum 25(OH) D levels (data not shown).
Table 5.
Pearson's correlation coefficient between serum 25(OH) D levels and various biochemical and clinical parameters
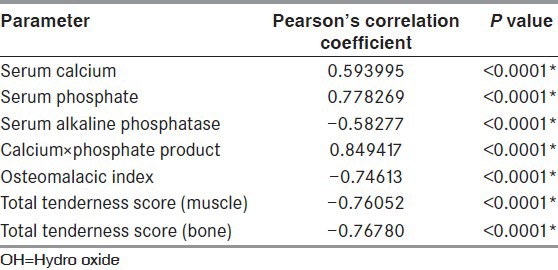
Figure 1.
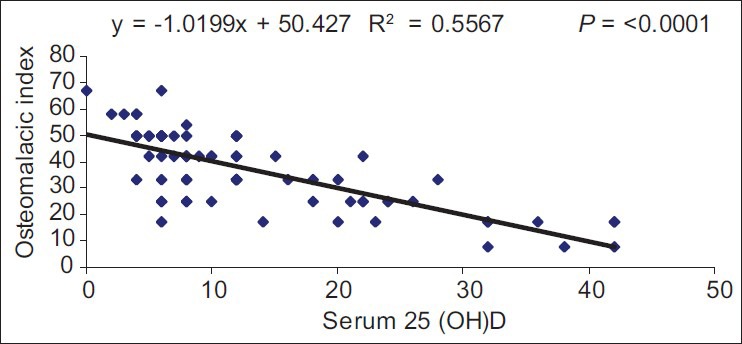
Scatter plot between serum 25(OH) D and osteomalacic index
Figure 2.
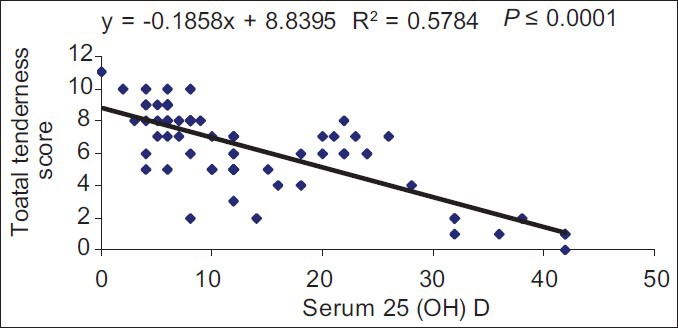
Scatter plot between serum 25(OH) D and total tenderness score (muscle)
Discussion
Headache, musculoskeletal symptoms and vitamin D deficiency are common in the general population. However, interrelation of these three has not been demonstrated in the literature. We, in this retrospective observation have tried to delineate the interrelations among three.
Interrelation between headache and chronic musculoskeletal pains
Epidemiological evidence suggests a strong association between chronic headache and musculoskeletal symptoms.[19,20,21] A recent study has demonstrated a bidirectional relationship between CDH and chronic musculoskeletal symptoms.[21] Development of one symptom may predispose to other.[21]
ICHD-II classify tension-type headache into two types: Tension-type headache associated with pericranial tenderness and tension-type headache not associated with pericranial tenderness. Increased muscle tenderness has also been observed in extracephalic muscles. Most studies have demonstrated a positive relation between muscle tenderness and intensity and frequency of tension-type headache.[22] However, no studies have delineated any association of muscle tenderness (cephalic or extra cephalic) to generalized bodily pain. In our observation, we noted a significant association between the musculoskeletal pain and muscle tenderness (cephalic or extra cephalic). Patients with CWP had a higher muscle tenderness score (7.1 vs. 5.4; P = 0. 0041). This observation also strengthens the notion that CDH and chronic musculoskeletal pain may have common pathogenesis.
Chronic musculoskeletal pain and vitamin D deficiency and/or osteomalacia
According to several studies, 26-100% patients with musculoskeletal pain may have vitamin D deficiency.[23,24,25,26,27,28,29] In a number of studies, skeletal pain responded to vitamin D treatment[30] In our observation, 83% patient reported musculoskeletal pain. Mean serum 25(OH) D was significantly lower in patients with nonspecific skeletal pain (12.2 vs. 21.4; P = 0. 0059). The proportion of patients having deficiency of 25(OH) D (<20 ng/ml) was significantly higher in patients with musculoskeletal pain (90% vs. 63%; P = 0.0187) compared with patients without musculoskeletal pain. TTS (for both muscles and bones) was significantly associated with serum vitamin D levels.
Interrelation between headache and vitamin D deficiency
A recent cross sectional study demonstrated significantly low levels of serum vitamin D in non-migraine headaches (? Tension-type headache).[3] A few case reports and small observational studies have also suggested a role of vitamin D deficiency in headaches.[4,5,6,7] Turner et al.[23] studied the prevalence of vitamin D inadequacy among 267 patients with chronic pain, including headache (25 patients). The prevalence of vitamin D inadequacy among these 267 patients was 26%. In a small Norwegian study,[5] patients reporting headache (63 patients) had significantly lower serum 25(OH) D levels than the subjects without headache.
Interrelation among chronic musculoskeletal pains, headache, and osteomalacia (or vitamin D deficiency)
We reported eight patients with vitamin D insufficiency having symptoms of both osteomalacia and CTTH.[4] Both headache and osteomalcia responded to vitamin D and calcium supplementation in a few weeks’ durations. These observations indicate that both headache and musculoskeletal pain in the same patient may be because of vitamin D insufficiency.
Moreover, as we noted, there are evidences that musculoskeletal pain may be causally related to vitamin D deficiency. In the same way, a strong association between musculoskeletal pain and headache has also been noted. These indicate a possibility of interrelation among three.
Serum vitamin D levels are highest in the months of May to September and the lowest from November to March.[31,32] If vitamin D has any association with headache and musculoskeletal pain, the prevalence rate of headache and musculoskeletal pain should match with the usual seasonal variation of vitamin D levels. Marrelli et al.[33] studied the seasonal and meteorological factors in primary headache disorders. The overall frequency of headaches was the highest during winter and least in summer. Similar observations were also noted in patients with migraine.[34] Takala et al.[35] studied the effects of seasonal variation in the frequency and prevalence of neck and shoulder pain. They noted decrease in frequency of symptoms from December to May (autumn to spring). Most rheumatic diseases have a high prevalence in the winter and spring.[36] In our observations, mean serum vitamin D levels were significantly lower in the patients who presented during winter-spring. In the same line, TTS and prevalence of CWP were higher in patients presenting during the winter-spring. Increased frequency of attacks in winter-spring (October to January) and least attacks in summer indirectly suggests a role of vitamin D deficiency in the generation of headaches and musculoskeletal pain.
Pathogenesis
Musculoskeletal pain and headaches: A spectrum within a same disease (vitamin D deficiency or osteomalacia)
The generalized musculoskeletal pain in the patients with headache is usually explained by the development of central sensitization.[22] However, in our case series, a possibility of vitamin D deficiency is more likely for the musculoskeletal pain. It is suggested that musculoskeletal pain associated with vitamin D deficiency could be because of associated osteomalacia.[14]
Our observation raises a few questions. Are both musculoskeletal pain and headaches related to vitamin D deficiency? Is semiology of headache and musculoskeletal pain same? Are the mechanisms of musculoskeletal pain and of headache same? Is the headache because of osteomalacia of the skull? Does osteomalacia of skull exist?
Musculoskeletal pains are among the most common complaint in patients with osteomalacia.[9] Pain is typically in bone and or muscle (not in the joint).[37] Pain is typically dull, diffuses, and poorly localized.[9] The clinical characteristics of pain of CTTH and pain of osteomalacia are of the same types. The tenderness, associated with CTTH, is uniformly increased throughout the pericranial and extracephalic regions.[22] The association of headache with musculoskeletal symptoms increased with the increasing of headache episodes.[20] This suggests that both symptoms may be causally interrelated. Therefore, headache in patients with generalized body pain may the part of the symptom complex of generalized pain.
Most studies on osteomalcia are silent regarding the presence of headache.[37] To the best of our literature search, none of the studies have ever examined skull x-ray for the presence of osteomalacic changes.[9,38] However, bone abnormality in the skull is a well-known feature of rickets (vitamin D deficiency in children). Craniotabes with the abnormal consistency of the cranial vault is an important feature of rickets.[9,38] A recent observation suggests that craniotabes may be the earliest sign of sub clinical vitamin D deficiency.[39] Cephalometric analysis has demonstrated altered craniofacial morphology in a few studies on rickets patients.[40] Therefore, a possibility of osteomalacic changes exists in the adult population with vitamin D deficiency.
Osteomalacia (of bones other than skull) commonly presents with spontaneous body pain and muscle tenderness. Therefore, we speculate that headache and pericranial muscle (or bone) tenderness may be associated with osteomalacia of skull bone. It is postulated that there is swollen deposition of collagen rich osteoid on the periosteal surface of the skeleton. This swollen deposition puts an outward pressure on the periosteal covering that is innervated by sensory pain fibers (nociceptors). This is the most likely explanation for bone and muscle pain in patients with osteomalacia.[14] We speculate a similar abnormality in the skull bone and it may explain headache and pericranial muscle tenderness in a subset of patients with headache. Prolonged nociceptive inputs from the periphery because of swollen deposition of any bone (skull, long bones, or spine) may sensitize the second and third order neurons (central sensitization).[41] This sensitization may further exacerbate/induce both cephalic and extra cephalic pain. In this way, a bi-directional association of headache and musculoskeletal pain could be explained.
Vitamin D deficiency is also known to produce osteomalacic myopathy and type II muscle atrophy.[42] Atrophy of certain group of muscles may produce mechanical stress on the remaining muscle. The mechanical overloaded muscle may pre-dispose to the formation of myofascial trigger point (TrPs).[42] Therefore, active TrPs in mechanical overloaded muscle may further sensitize the second and third order neurons. Both peripheral and central sensitizations are well-known mechanisms for the generation of pain in the patients with CTTH.[41]
Recently, a new mechanism has been proposed for musculoskeletal symptoms because of vitamin D deficiency. Tague and Smith[43] have demonstrated vitamin D receptors in nociceptors (“pain sensing” nerves). In another study Tauge et al.[44] have demonstrated muscle hypersensitivity in rats receiving vitamin D-deficient diets. Morphometry of skeletal muscle innervations showed increased numbers of “pain sensing” nerve nociceptor axons (sensory hyperinnervation). These occurred before the onset of overt muscle or bone pathology. The authors concluded that muscle hypersensitivity and sensory hyperinnervation may be responsible for the generation of musculoskeletal pain and this deep muscle pain may be in the early stage of vitamin D deficiency and may precede the development of gross bone pathology. Muscular factors are considered to be of importance in tension-type headache. Therefore, a possibility of similar mechanisms (muscle hypersensitivity and sensory hyperinnervation) exists in a subset of patients with headache and vitamin D deficiency.
Another possible hypothesis for the generation of headache may be hypomagnesemia, as vitamin D deficiency is known to cause hypomagnesemia. About 40-50% patients with TTH may have low serum Mg. Almost similar percentage of patients with TTH have demonstrated a response to Mg therapy in various observations.[45]
Vitamin D has anti-inflammatory properties.[46] Therefore, patients with pain may get some relief by vitamin D supplementation.
Taken together, we speculate that the co-occurrence of body pain and headache in a patient may be a symptom complex of a single disease (may be vitamin D deficiency) rather than two different disease entities or two different mechanisms, at least in a subset of patients. Moreover, since a possibility of headache with pericranial tenderness exists with vitamin D deficiency, we speculate a possibility of osteomalcia of skull as a cause of (secondary) CTTH in a patient fulfilling the ICHD-II criteria for CTTH with pericranial tenderness.
Future perspectives: Osteomalacia is an under diagnosed condition
A possibility of diagnostic errors is very high for generalized musculoskeletal pain.[47] Fitzcharles and Boulos[48] reported “disturbing” inaccuracy in the diagnosis of fibromyalgia. In their cohort of patients referred to a Rheumatology clinic: Fibromyalgia was confirmed in only 34% of the patients presenting with musculoskeletal pain, with a diagnostic error of 66%. Fibromyalgia is a well-recognized entity with a widely accepted diagnostic criterion. The high rate of misdiagnosis/over diagnosis of fibromyalgia raises a possibility of under diagnosis of other causes of musculoskeletal pain (most have not definitive diagnostic criteria or a marker). Holick[14] suggests that the symptoms of osteomalacia are either dismissed or misdiagnosed as fibromyalgia by many physicians.
Misdiagnosis and delayed diagnosis was noted in most studies of biopsy proven osteomalacia.[49,50,51,52] The misdiagnosis or under diagnosis may be because of unfamiliarity with the clinical picture of osteomalacia and not well-defined or widely accepted criteria for osteomalacia.[14] As musculoskeletal pain and tenderness of osteomalacia of bones (other than skull) match to the headache and pericephalic (and extracephalic) tenderness in patients with CTTH, a possibility of osteomalacia of skull exists. Bone abnormality in the skull (craniotabe) in rickets further strengthens the possibility of osteomalacoa of the skull. Therefore, it is also important to refine this symptom (osteomalacia of skull) in the adult population.
Limitations of the observation
A possibility of shared exogenous or endogenous factors is most likely for the development of multiple chronic pain conditions. However, it may be simple unidirectional causality–as one condition may cause or aggravate a second (through central sensitization). In addition, we don’t have a control group to compare the serum vitamin D levels. As the prevalence of vitamin D deficiency is very high in the general population, the observations may be simply because of the high background prevalence of hypovitaminosis D. The treatment was not standardized. Therefore, we couldn’t compare the effects of vitamin D between the groups. Although all common causes of secondary musculoskeletal pain were ruled out by careful history taking, the clinical examinations, and appropriate investigations; a possibility of other secondary causes of musculoskeletal pain cannot be ruled out completely.
This is a retrospective study, therefore, a number of weaknesses exist in our observations. The target population was not well-defined. We included consecutive series of adult patients who were diagnosed as having CTTH and were subjected to the estimation of serum vitamin D levels. A possibility of unrecognized selection bias also exists. The detail clinical examinations were carried out prospectively in all patients at the time of presentation as a departmental policy for such patients. However, because of the retrospective nature of the study, follow-up was not standardized and we could not assess the patients in follow-up. Moreover, our sample size was not large enough to reveal the true differences between the groups. In addition, our observations cannot be generalized as our sample of patients may not truly represent patients with CTTH due to referral and other biases. Although we have included a few confounders in the data analysis, a possibility of other unrecognized confounders cannot be ruled out. These problems may be resolved by doing a prospective study.
Despite a number of limitations in the study, our observation suggests that the chronic musculoskeletal pain and chronic headache shared a common pathology and both may be a part of the same disease in a subset of patients. We hope our observations may serve as a catalyst for prospective observations to clarify the issue.
Footnotes
Source of Support: Nil
Conflict of Interest: Nil
References
- 1.McBeth J, Jones K. Epidemiology of chronic musculoskeletal pain. Best Pract Res Clin Rheumatol. 2007;21:403–25. doi: 10.1016/j.berh.2007.03.003. [DOI] [PubMed] [Google Scholar]
- 2.Straube S, Andrew Moore R, Derry S, McQuay HJ. Vitamin D and chronic pain. Pain. 2009;141:10–3. doi: 10.1016/j.pain.2008.11.010. [DOI] [PubMed] [Google Scholar]
- 3.Kjaergaard M, Eggen AE, Mathiesen EB, Jorde R. Association Between Headache and Serum 25-Hydroxyvitamin D; the Tromsø Study: Tromsø 6. Headache. 2012;10:1499–1505. doi: 10.1111/j.1526-4610.2012.02250.x. [DOI] [PubMed] [Google Scholar]
- 4.Prakash S, Shah ND. Chronic tension-type headache with vitamin D deficiency: Casual or causal association? Headache. 2009;49:1214–22. doi: 10.1111/j.1526-4610.2009.01483.x. [DOI] [PubMed] [Google Scholar]
- 5.Knutsen KV, Brekke M, Gjelstad S, Lagerløv P. Vitamin D status in patients with musculoskeletal pain, fatigue and headache: A cross-sectional descriptive study in a multi-ethnic general practice in Norway. Scand J Prim Health Care. 2010;28:166–71. doi: 10.3109/02813432.2010.505407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.O’Brien H, Hershey AD, Kabbouche MA, Powers S, Cherney S, LeCates S, et al. Prevalence of vitamin D deficiency among pediatric patients with recurrent headaches. Headache. 2010;50:23. [Google Scholar]
- 7.Wheeler SD. Vitamin D deficiency in chronic migraine. Headache. 2008;48:52–3. [Google Scholar]
- 8.Prakash S, Mehta NC, Dabhi AS, Lakhani O, Khilari M, Shah ND. The prevalence of headache may be related with the latitude: A possible role of Vitamin D insufficiency? J Headache Pain. 2010;11:301–7. doi: 10.1007/s10194-010-0223-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Reginato AJ, Coquia JA. Musculoskeletal manifestations of osteomalacia and rickets. Best Pract Res Clin Rheumatol. 2003;17:1063–80. doi: 10.1016/j.berh.2003.09.004. [DOI] [PubMed] [Google Scholar]
- 10.Headache Classification Committee of the International Headache Society. Classification and diagnostic criteria for headache disorders, cranial neuralgias, and facial pain. Cephalalgia. (2nd ed) 2004;24:1–160. [PubMed] [Google Scholar]
- 11.Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL, et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990;33:160–72. doi: 10.1002/art.1780330203. [DOI] [PubMed] [Google Scholar]
- 12.Schoenen J, Bottin D, Hardy F, Gerard P. Cephalic and extracephalic pressure pain thresholds in chronic tension-type headache. Pain. 1991;47:145–9. doi: 10.1016/0304-3959(91)90198-7. [DOI] [PubMed] [Google Scholar]
- 13.Metsahonkala L, Anttila P, Laimi K, Aromaa M, Helenius H, Mikkelsson M, et al. Extracephalic tenderness and pressure pain threshold in children with headache. Eur J Pain. 2006;10:581–5. doi: 10.1016/j.ejpain.2005.08.005. [DOI] [PubMed] [Google Scholar]
- 14.Holick MF. Vitamin D deficiency: What a pain it is. Mayo Clin Proc. 2003;78:1457–9. doi: 10.4065/78.12.1457. [DOI] [PubMed] [Google Scholar]
- 15.Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357:266–81. doi: 10.1056/NEJMra070553. [DOI] [PubMed] [Google Scholar]
- 16.Jenkins DH, Roberts JG, Webster D, Williams EO. Osteomalacia in elderly patients with fracture of the femoral neck. A clinico-pathological study. J Bone Joint Surg Br. 1973;55:575–80. [PubMed] [Google Scholar]
- 17.Bingham CT, Fitzpatrick LA. Noninvasive testing in the diagnosis of osteomalacia. Am J Med. 1993;95:519–23. doi: 10.1016/0002-9343(93)90335-m. [DOI] [PubMed] [Google Scholar]
- 18.McKenna MJ, Freaney R, Casey OM, Towers RP, Muldowney FP. Osteomalacia and osteoporosis: Evaluation of a diagnostic index. J Clin Pathol. 1983;36:245–52. doi: 10.1136/jcp.36.3.245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.McFate T, Scher AI. Chronic pain disorders and headache chronification. Curr Pain Headache Rep. 2009;13:308–13. doi: 10.1007/s11916-009-0049-2. [DOI] [PubMed] [Google Scholar]
- 20.Hagen K, Einarsen C, Zwart JA, Svebak S, Bovim G. The co-occurrence of headache and musculoskeletal symptoms amongst 51 050 adults in Norway. Eur J Neurol. 2002;9:527–33. doi: 10.1046/j.1468-1331.2002.00451.x. [DOI] [PubMed] [Google Scholar]
- 21.Hagen K, Linde M, Steiner TJ, Zwart JA, Stovner LJ. The bidirectional relationship between headache and chronic musculoskeletal complaints: An 11-year follow-up in the Nord-Trøndelag Health Study (HUNT) Eur J Neurol. 2012;19:1447–54. doi: 10.1111/j.1468-1331.2012.03725.x. [DOI] [PubMed] [Google Scholar]
- 22.Fumal A, Schoenen J. Tension-type headache: Current research and clinical management. Lancet Neurol. 2008;7:70–83. doi: 10.1016/S1474-4422(07)70325-3. [DOI] [PubMed] [Google Scholar]
- 23.Turner MK, Hooten WM, Schmidt JE, Kerkvliet JL, Townsend CO, Bruce BK. Prevalence and clinical correlates of vitamin D inadequacy among patients with chronic pain. Pain Med. 2008;9:979–84. doi: 10.1111/j.1526-4637.2008.00415.x. [DOI] [PubMed] [Google Scholar]
- 24.Plotnikoff GA, Quigley JM. Prevalence of severe hypovitaminosis D in patients with persistent, nonspecific musculoskeletal pain. Mayo Clin Proc. 2003;78:1463–70. doi: 10.4065/78.12.1463. [DOI] [PubMed] [Google Scholar]
- 25.Glerup H, Mikkelsen K, Poulsen L, Hass E, Overbeck S, Thomsen J, et al. Commonly recommended daily intake of vitamin D is not sufficient if sunlight exposure is limited. J Intern Med. 2000;247:260–8. doi: 10.1046/j.1365-2796.2000.00595.x. [DOI] [PubMed] [Google Scholar]
- 26.Badsha H, Daher M, Ooi Kong K. Myalgias or non-specific muscle pain in Arab or Indo-Pakistani patients may indicate vitamin D deficiency. Clin Rheumatol. 2009;28:971–3. doi: 10.1007/s10067-009-1146-7. [DOI] [PubMed] [Google Scholar]
- 27.Heidari B, Shirvani JS, Firouzjahi A, Heidari P, Hajian-Tilaki KO. Association between nonspecific skeletal pain and vitamin D deficiency. Int J Rheum Dis. 2010;13:340–6. doi: 10.1111/j.1756-185X.2010.01561.x. [DOI] [PubMed] [Google Scholar]
- 28.Al Faraj S, Al Mutairi K. Vitamin D deficiency and chronic low back pain in Saudi Arabia. Spine (Phila Pa 1976. 2003;28:177–9. doi: 10.1097/00007632-200301150-00015. [DOI] [PubMed] [Google Scholar]
- 29.McBeth J, Pye SR, O’Neill TW, Macfarlane GJ, Tajar A, Bartfai G, et al. Musculoskeletal pain is associated with very low levels of vitamin D in men: Results from the European Male Ageing Study. Ann Rheum Dis. 2010;69:1448–52. doi: 10.1136/ard.2009.116053. [DOI] [PubMed] [Google Scholar]
- 30.Huang W, Shah S, Long Q, Crankshaw AK, Tangpricha V. Improvement of pain, sleep, and quality of life in chronic pain patients with vitamin d supplementation. Clin J Pain. 2013;29:341–7. doi: 10.1097/AJP.0b013e318255655d. [DOI] [PubMed] [Google Scholar]
- 31.Maxwell JD. Seasonal variation in vitamin D. Proc Nutr Soc. 1994;53:533–43. doi: 10.1079/pns19940063. [DOI] [PubMed] [Google Scholar]
- 32.Rapuri PB, Kinyamu HK, Gallagher JC, Haynatzka V. Seasonal changes in calciotropic hormones, bone markers, and bone mineral density in elderly women. J Clin Endocrinol Metab. 2002;87:2024–32. doi: 10.1210/jcem.87.5.8475. [DOI] [PubMed] [Google Scholar]
- 33.Marrelli A, Marini C, Prencipe M. Seasonal and meteorological factors in primary headaches. Headache. 1988;28:111–3. doi: 10.1111/j.1526-4610.1988.hed2802111.x. [DOI] [PubMed] [Google Scholar]
- 34.Soriani S, Fiumana E, Manfredini R, Boari B, Battistella PA, Canetta E, et al. Circadian and seasonal variation of migraine attacks in children. Headache. 2006;46:1571–4. doi: 10.1111/j.1526-4610.2006.00613.x. [DOI] [PubMed] [Google Scholar]
- 35.Takala EP, Viikari-Juntura E, Moneta GB, Saarenmaa K, Kaivanto K. Seasonal variation in neck and shoulder symptoms. Scand J Work Environ Health. 1992;18:257–61. doi: 10.5271/sjweh.1580. [DOI] [PubMed] [Google Scholar]
- 36.Schlesinger N, Schlesinger M. Seasonal variation of rheumatic diseases. Discov Med. 2005;5:64–9. [PubMed] [Google Scholar]
- 37.Masood H, Narang AP, Bhat IA, Shah GN. Persistent limb pain and raised serum alkaline phosphatase the earliest markers of subclinical hypovitaminosis D in Kashmir. Indian J Physiol Pharmacol. 1989;33:259–61. [PubMed] [Google Scholar]
- 38.Parfitt AM. Osteomalacia and related disorders. In: Avioli VL, Krane SM, editors. Metabolic Bone Disease and Clinically Related Disorders. 3rd ed. New York: Academic Press; 1996. pp. 327–86. [Google Scholar]
- 39.Yorifuji J, Yorifuji T, Tachibana K, Nagai S, Kawai M, Momoi T, et al. Craniotabes in normal newborns: The earliest sign of subclinical vitamin D deficiency. J Clin Endocrinol Metab. 2008;93:1784–8. doi: 10.1210/jc.2007-2254. [DOI] [PubMed] [Google Scholar]
- 40.Al-Jundi SH, Dabous IM, Al-Jamal GA. Craniofacial morphology in patients with hypophosphataemic vitamin-D-resistant rickets: A cephalometric study. J Oral Rehabil. 2009;36:483–90. doi: 10.1111/j.1365-2842.2009.01963.x. [DOI] [PubMed] [Google Scholar]
- 41.Fernández-de-las-Peñas C, Cuadrado ML, Arendt-Nielsen L, Simons DG, Pareja JA. Myofascial trigger points and sensitization: An updated pain model for tension-type headache. Cephalalgia. 2007;27:383–93. doi: 10.1111/j.1468-2982.2007.01295.x. [DOI] [PubMed] [Google Scholar]
- 42.Pfeifer M, Begerow B, Minne HW. Vitamin D and muscle function. Osteoporos Int. 2002;13:187–94. doi: 10.1007/s001980200012. [DOI] [PubMed] [Google Scholar]
- 43.Tague SE, Smith PG. Vitamin D receptor and enzyme expression in dorsal root ganglia of adult female rats: Modulation by ovarian hormones. J Chem Neuroanat. 2011;41:1–12. doi: 10.1016/j.jchemneu.2010.10.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Tague SE, Clarke GL, Winter MK, McCarson KE, Wright DE, Smith PG. Vitamin D deficiency promotes skeletal muscle hypersensitivity and sensory hyperinnervation. J Neurosci. 2011;31:13728–38. doi: 10.1523/JNEUROSCI.3637-11.2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Altura BM, Altura BT. Tension headaches and muscle tension: Is there a role for magnesium? Med Hypotheses. 2001;57:705–13. doi: 10.1054/mehy.2001.1439. [DOI] [PubMed] [Google Scholar]
- 46.Baeke F, Gysemans C, Korf H, Mathieu C. Vitamin D insufficiency: Implications for the immune system. Pediatr Nephrol. 2010;25:1597–606. doi: 10.1007/s00467-010-1452-y. [DOI] [PubMed] [Google Scholar]
- 47.Reilly PA. The differential diagnosis of generalized pain. Baillieres Best Pract Res Clin Rheumatol. 1999;13:391–401. doi: 10.1053/berh.1999.0028. [DOI] [PubMed] [Google Scholar]
- 48.Fitzcharles MA, Boulos P. Inaccuracy in the diagnosis of fibromyalgia syndrome: Analysis of referrals. Rheumatology (Oxford) 2003;42:263–7. doi: 10.1093/rheumatology/keg075. [DOI] [PubMed] [Google Scholar]
- 49.Reginato AJ, Falasca GF, Pappu R, McKnight B, Agha A. Musculoskeletal manifestations of osteomalacia: Report of 26 cases and literature review. Semin Arthritis Rheum. 1999;28:287–304. doi: 10.1016/s0049-0172(99)80013-4. [DOI] [PubMed] [Google Scholar]
- 50.de Torrenté de la Jara G, Pécoud A, Favrat B. Female asylum seekers with musculoskeletal pain: The importance of diagnosis and treatment of hypovitaminosis D. BMC Fam Pract. 2006;7:4. doi: 10.1186/1471-2296-7-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Nellen JF, Smulders YM, Jos Frissen PH, Slaats EH, Silberbusch J. Hypovitaminosis D in immigrant women: Slow to be diagnosed. BMJ. 1996;312:570–2. doi: 10.1136/bmj.312.7030.570. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Basha B, Rao DS, Han ZH, Parfitt AM. Osteomalacia due to vitamin D depletion: A neglected consequence of intestinal malabsorption. Am J Med. 2000;108:296–300. doi: 10.1016/s0002-9343(99)00460-x. [DOI] [PubMed] [Google Scholar]