

Abstract
Ictal Pet in presurgical workup of refractory epilepsy is seldom performed and limited due to technical difficulties. In carefully selected patient subset with frequent extratemporal seizures, ictal PET depicts ‘seizure onset zone’ with high spatial resolution even within a widespread pathology. We here depict a four year old with posterior quadrant dysplasia evaluated with ictal PET.
Key Words: Epilepsy, Ictal PET, presurgical workup, refractory
Introduction
Ictal PET studies are limited by several technical difficulties but tend to have high spatial resolution and utility in a selected patient subset. We here report a case with refractory epilepsy evaluated by ictal PET.
Case
A 4-year-girl was evaluated for medically refractory daily seizures of 2 years duration. Seizures started with ocular deviation to left with nystagmoid eye movements, followed by brief posturing of both limbs, kicking movements of the legs and restlessness lasting less than a minute. She was on five antiepileptic medications at evaluation. Examination was normal except for doubtful right hemifield visual deficit.
Magnetic resonance imaging (MRI) showed right posterior quadrant dysplasia [Figure 1]. Video-EEG showed right posterior head region slowing and interictal epileptiform discharges with typical complex partial seizures arising from the right posterior head regions [Figure 2, see video]. Planned ictal positron emission tomography (PET) showed increased ictal metabolism in the right lateral parietal-occipital region [Figure 3]. She underwent right posterior quadrant disconnection to remain seizure free at 2 year follow-up.
Figure 1.
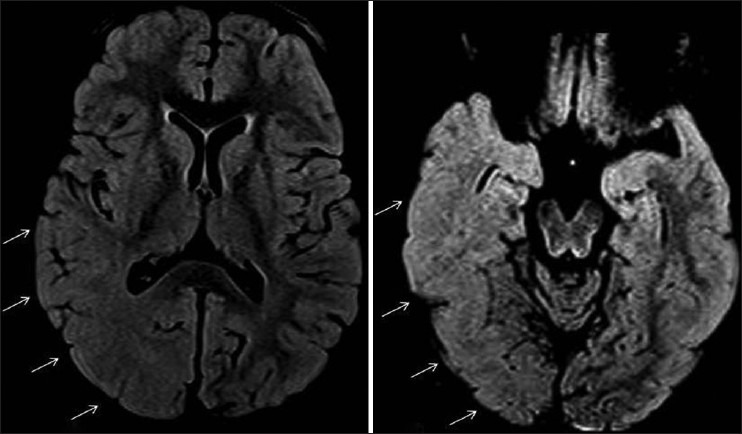
MRI brain (1.5T-FLAIR sequence) showing right parietal-temporal-occiptal dysplasia with poor gray white differentiation (arrows)
Figure 2.
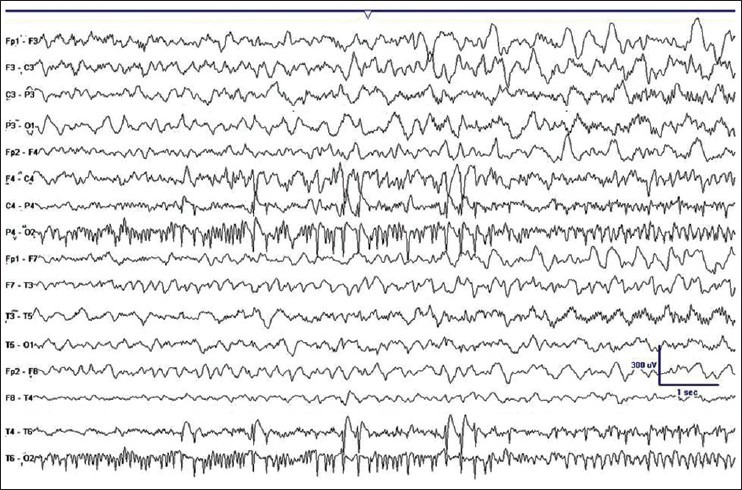
EEG during one of the complex partial seizure during video-EEG (bipolar anterior to posterior montage) showing right-occipital 15 hz rhythm evolving to 5-7 hz theta activity over the right posterior head region at seizure onset
Figure 3.
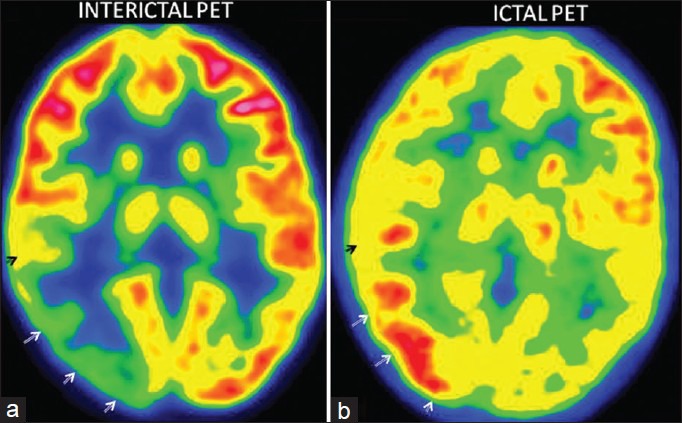
PET imaging showing right temporo-parietal interictal hypometabolism (a) that during seizure demonstrates hypermetabolism (b). Note the mildly increased metabolism in bilateral thalamus and basal ganglia with widespread hypometabolism diffusely in the ictal PET
Discussion
FDG-PET is a standard non-invasive tool in presurgical refractory epilepsy evaluation with high spatial resolution than ictal SPECT.[1] Commonly, interictal PET is performed due to short 110-minute FDG ligand half-life. PET abnormalities are dynamic and variable. Interictal PET may show widespread hypometabolism than the ‘ictal onset zone’. This can be accurately clarified with ictal PET in selective patients with high seizure frequency more so in extratemporal epilepsies.[2] In patients with widespread or large area of MRI abnormality, ictal PET or ictal SPECT help localize ‘seizure onset zone’ within this abnormality that help planning invasive recordings, surgical resection, and prognosticate seizure outcomes after surgery. PET imaging is considered integral of the pediatric refractory epilepsy presurgical workup.[3]
Videos available at www.annalsofian.org
Footnotes
Source of Support: Nil
Conflict of Interest: Nil
References
- 1.Van Paesschen W, Dupont P, Sunaert S, Goffin K, Van Laere K. The use of SPECT and PET in routineclinical practice in epilepsy. Curr Opin Neurol. 2007;20:194–202. doi: 10.1097/WCO.0b013e328042baf6. [DOI] [PubMed] [Google Scholar]
- 2.Meltzer CC, Adelson PD, Brenner RP, Crumrine PK, Van Cott A, Schiff DP, et al. Planned ictal FDG PET imaging for localization of extratemporal epileptic foci. Epilepsia. 2000;41:193–200. doi: 10.1111/j.1528-1157.2000.tb00139.x. [DOI] [PubMed] [Google Scholar]
- 3.Ollenberger GP, Byrne AJ, Berlangieri SU, Rowe CC, Pathmaraj K, Reutens DC, et al. Assessment of the role of FDG PET in the diagnosis and management of children with refractory epilepsy. Eur J Nucl Med Mol Imaging. 2005;32:1311–6. doi: 10.1007/s00259-005-1844-6. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.