

Abstract
A 57-year-old Caucasian man, otherwise fit and well, presented with a 2-week history of dysphagia, odynophagia. Two weeks prior to the presentation, he had felt a fishbone stuck in his throat which was self-extruded after 3 days. Subsequently he developed a right anterior neck swelling and hoarseness. Transnasal endoscopic examination of larynx revealed an injected and oedematous right hemilarynx with right vocal cord paresis. An ultrasound examination of the neck confirmed a collection in the neck on the right side, and frank pus was aspirated from the neck abscess and he responded well to conservative management. Subsequent examination in follow-up had shown complete recovery of vocal cord movement. The patient did not seek medical attention immediately after getting a 5 cm fishbone extruded from the throat which resulted in significant morbidity. All patients should be alerted to the possibility of delayed complications and they should be encouraged to seek urgent medical attention.
Background
It is a very common presentation in ear nose throat (ENT) emergency clinic with a foreign body sensation after swallowing fish. Oftentimes, the fishbone is lodged in the tonsil or base of tongue and is easily removed.1 Neck abscess is an uncommon condition most commonly caused by odontogenic or upper airway infections spreading through the lymphatic system.2 However, it is very rare to present with vocal cord paresis and neck abscess as a delayed complication following a fishbone being stuck in the throat. Serious complications can be prevented by seeking an urgent specialist (ENT) review.
Case presentation
A 57-year-old Caucasian man, otherwise fit and well, presented with a 2-week history of dysphagia, odynophagia and subsequently developed a neck swelling on the right side and hoarseness. On careful history he could recall that while eating a fish during his dinner, he felt a fishbone stuck in his throat 2 weeks ago. He did not seek any medical help but continued his efforts to dislodge the stuck fishbone by traditional methods of eating bread and took regular paracetamol for throat pain. A 5 cm long fishbone (figure 1) spontanoeusly came out of his throat 3 days later. However, the pain in his throat gradually got worse and he developed dysphagia for solids. Two days prior to presentation to the accident and emergency department he developed right-sided neck swelling associated with a hoarse voice. He never smoked but enjoyed occasional alcohol.
Figure 1.

Fishbone.
On examination he was non-feverish and systemically well. He was found to have a 4 cm right neck swelling (figure 2) associated with the right lobe of thyroid gland and it moved with deglutition. Adjacent cervical lymph nodes in right neck levels III and IV were also palpable but were benign on clinical examination. Transnasal pharyngolaryngoscopy revealed injected and oedematous right hemilarynx involving the laryngeal surface of epiglottis, false cord, right true cord and significantly oedematous arytenoids process with reduced mobility of the right vocal cord.
Figure 2.

Right neck abscess.
Investigations
The soft tissue neck X-ray (figure 3) did not show any retained radio-opaque foreign body. The ultrasound scan (USS) of his neck revealed a 21 mm×18 mm×31 mm well-defined hypoechoic area within the right-sided strap muscles indenting the superior border of the right lobe of the thyroid gland. Overall, the appearances were consistent with a resolving infection or haematoma (figure 4). A fine-needle aspiration yielded 2 mL of frank pus. The cytological examination showed a cellular specimen and consisted of neutrophil polymorphs. The features were in keeping with an acute inflammatory process, an abscess. The microscopy of the aspirated material revealed Pus cells +++ and Gram-positive cocci ++ but no acid and alcohol fast bacilli were observed on tuberculosis (TB) microscopy. On culture, a profuse growth of Streptococcus milleri was established sensitive to clindamycin, doxycycline, erythromycin, penicillin and tetracycline. There was no growth in 12 weeks on a mycobacterial culture.
Figure 3.
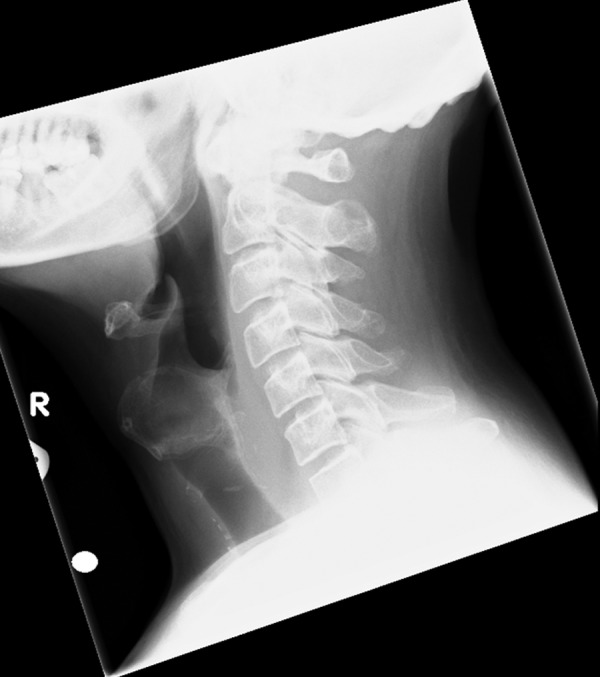
Lateral soft tissue neck X-ray.
Figure 4.
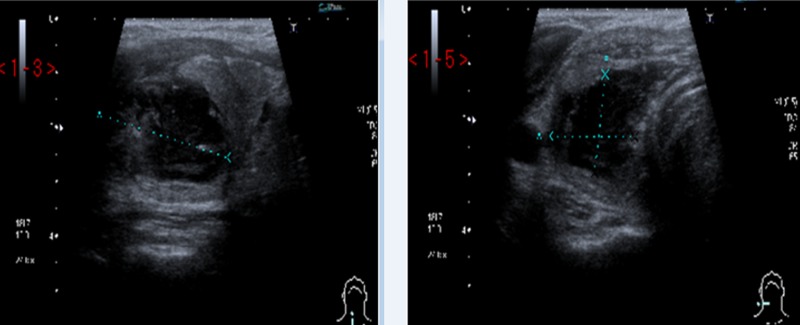
Ultrasound scan of the neck showing 21 mm×18 mm×31 mm well-defined hypoechoic area within the right-sided strap muscles indenting the superior border of the right lobe of the thyroid gland.
Differential diagnosis
Any patient presented with a neck swelling and hoarseness of voice would prompt an ENT surgeon to rule out the Head and Neck cancer. In this case the patient is a non-smoker and the duration of the symptoms before the presentation was short. The acute presentation is more often due to infection. He never had any dental infection, which is the most common cause of neck swelling. Therefore, a detailed history of any recent trauma and a complete otolaryngological examination to rule out the aforementioned causes is required.
Treatment
The patient was managed conservatively with regular oral analgesia and intravenous coamoxiclav. He responded well and was discharged home in 48 h on oral antibiotic medications.
Outcome and follow-up
On subsequent follow-up at otolaryngology out-patient clinic in 1 month, complete recovery of vocal cord movement was noted and the neck swelling completely disappeared.
No long-term complications were noticed.
Discussion
Deep neck space infections are an uncommon clinical entity in postantibiotic era. The common causes of deep neck abscess include odontogenic or upper airway infection. Although rare, a fishbone can easily penetrate the soft tissues of the throat and introduce pathogenic organisms into the deeper tissues of neck.
Commonly, the patients with a fishbone stuck in their throat are referred to the otolaryngology department from accident and emergency or by general practitioners. They can present with a feeling of something stuck in the throat, dysphagia or odynophagia. The tonsils or base of tongue are the commonest areas where a fishbone can get lodged. However, the fishbones may also become lodged in the vallecula, pyriform fossa, epiglottis, cricopharyngeus and oesophagus.1 If the fishbone is not removed from the throat then serious complications can result including a deep neck abscess, mediastinitis, perforated oesophagus and vocal cord paresis.3 Occasionally serious vascular complications may arise, including aortic-oesophageal fistula, innominate oesophageal fistula; subclavian oesophageal fistula and carotid rupture.4 These complications arise from the movement of the fishbone through the soft tissues of the neck. The mechanism for the movement of foreign bodies through the soft tissues of the throat or oesophagus is still unclear; however, it has been suggested that it is the result of peristalsis combined with movements of the neck.5
A patient with a history of foreign body ingestion associated with persistent pharyngalgia and fever would suggest an oesophageal perforation.6 Furthermore radiographic signs such as thickened soft tissue and gas in the retropharyngeal or anterior cervical region would be indicative of a deep neck abscess.7 The CT/MRI scans are definitive investigations to rule out deep neck space infection.
In our case, it would appear that the neck abscess was a result of a direct injury caused by ingestion of a foreign object. The ingested fishbone perforated the patient's hypopharynx and possibly the thyroid gland resulting in the formation of a neck and thyroid abscess. The ingested fishbone was 5 cm long and it had traumatised the right-sided hemilarynx. The two possible explanations for impaired mobility of the right-sided vocal cord are significant inflammation caused by direct trauma to the larynx and/or recurrent laryngeal nerve irritation secondary to inflammation and abscess in the neck. The vocal cord paresis has been linked to mechanical obstruction of vocal cord movement and has also been reported on rare occasions to be caused by direct damage to the nerve by the foreign body.8
An important feature in our patient is delayed occurrence of complications, that is, 1 week after the fishbone had spontaneously extruded. It seems prudent to recommend that patients should seek medical attention after choking on a fishbone, regardless whether they are able to remove the fishbone themselves. In our case the fishbone remained stuck in the throat for 3 days and led to significant throat trauma which could have caused compromised airway and septic complications.
Flexible pharyngolaryngoscopy is important in patients presenting with a fishbone stuck in the throat to confirm the presence of a fishbone in the upper aerodigestive tract. In our case a flexible pharyngolaryngoscopy revealed an injected and oedematous right hemilarynx with right vocal cord paresis, which proved useful in explaining the hoarseness our patient was suffering from. Although our patient had a neck abscess but he responded well to aspiration of an abscess from his neck and avoided open incision and drainage under general anaesthetic. No long-term complications were noticed and he made a full recovery.
Conclusion
The patients should be encouraged to seek urgent medical attention after choking on a fishbone. Flexible pharyngolaryngoscopy is the standard of care in such cases to confirm the presence of a fishbone in the upper aerodigestive tract. The patients should be alerted to the possibility of developing a neck abscess even after the fishbone had been removed from their throat. In select cases, the neck and thyroid abscess can be managed with aspiration and antibiotic treatment.
Learning points.
Do not ignore a patient with a foreign body sensation in throat following fishbone ingestion.
Incidence of serious complications should be kept in mind.
Urgent specialist review (otolaryngology) should be sought.
More often they can be managed conservatively.
Footnotes
Contributors: VV, MS and KWA-S was involved in data collection, literature search, preparing and finalising the manuscript. SC was involved in literature search, preparing and finalising the manuscript.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Pang KP, Pang YT. A rare case of a foreign body migration from the upper digestive tract to the subcutaneous neck. Ear Nose Throat J 2002;2013:730–2 [PubMed] [Google Scholar]
- 2.Huang TT, Liu TC, Chen PR, et al. Deep neck infection: analysis of 185 cases. Head Neck 2004;2013:854–60 [DOI] [PubMed] [Google Scholar]
- 3.Lue AJ, Fang WD, Manolidis S. Use of plain radiography and computed tomography to identify fish bone foreign bodies. Otolaryngol Head Neck Surg 2000;2013:435–8 [DOI] [PubMed] [Google Scholar]
- 4.Lam HC, Woo JK, van Hasselt CA. Esophageal perforation and neck abscess from ingested foreign bodies: treatment and outcomes. Ear Nose Throat J 2003;2013:786, 789–94 [PubMed] [Google Scholar]
- 5.Lin ZH, Teng YS, Lin M. Acute thyroid abscess secondary to oesophageal perforation. J Int Med Res 2008;2013:860–4 [DOI] [PubMed] [Google Scholar]
- 6.Remsen K, Lawson W, Biller HF, et al. Unusual presentations of penetrating foreign bodies of the upper aerodigestive tract. Ann Otol Rhinol Laryngol Suppl 1983;2013:32–44 [DOI] [PubMed] [Google Scholar]
- 7.Tang IP, Singh S, Shoba N, et al. Migrating foreign body into the common carotid artery and internal jugular vein—a rare case. Auris Nasus Larynx 2009;2013:380–2 [DOI] [PubMed] [Google Scholar]
- 8.Honda K, Tanaka S, Tamura Y, et al. Vocal cord fixation caused by an impacted fish bone in hypopharynx: report of a rare case. Am J Otolaryngol 2007;2013:257–9 [DOI] [PubMed] [Google Scholar]