

Abstract
Aim and Objectives:
To comparatively evaluate the microleakage and microgap formation along the gingival margin in class II cavities restored with silorane resin composite and methacrylate resin composite with and without flowable resin liner.
Materials and Methods:
Sixty human mandibular premolars were distributed into three groups, each group containing 20 teeth (n = 20). Mesial (subgroup A) and distal (subgroup B) box cavities were prepared with gingival margin above and below cemento enamel junction (CEJ), respectively, in each tooth and restored as follows — Group I — Silorane resin composite with self-etch primer and bond (Filtek P90, 3M ESPE MN, USA). Group II — Methacrylate resin composite (Filtek P60, 3M ESPE MN, USA) and self-etch adhesive (Adper Easy one, 3M ESPE MN, USA). Group III — Methacrylate resin composite with self-etch adhesive and a flowable resin liner (Filtek Z350 XT, 3M ESPE MN, USA). The teeth were thermocycled and immersed in 50% silver nitrate solution before sectioning. The specimens were observed under scanning electron microscope for dye penetration and microgap formation. The data was subjected to statistical analysis using Kruskal-Wallis test and Mann-Whitney U test using SPSS version 18.
Results:
Subgroup A in all the three groups showed significantly less microleakage and microgap formation compared to subgroup B with P < 0.05.
Intergroup comparison of subgroup A did not show statistically significant difference, whereas subgroup B showed statistically significant difference for microleakage between group I and group II (P = 0.003), group III and group II (P = 0.002).
Conclusion:
Silorane resin composite and methacrylate resin with liner showed significantly less microleakage in class II cavities along the gingival margin placed below CEJ compared to methacrylate resin without liner. All the study groups showed less microleakage and microgap formation along the gingival margin placed above CEJ.
Keywords: Flowable resin liner, methacrylate resin, microgap, microleakage, scanning electron microscope, silorane resin
INTRODUCTION
Resin composites have improved greatly since their introduction and are now the materials of choice for most of the restorations. Many commercially available dental composites are based on methacrylate chemistry, and volumetric shrinkage still remains a major drawback, which can result in gap formation at the tooth restoration interface causing microleakage, permitting the passage of bacteria and oral fluids resulting in post-operative sensitivity, pulpal inflammation, and secondary caries.[1,2] Several restorative techniques have been proposed to minimize polymerization shrinkage such as — use of resin liner under the restoration,[3] incremental placement of restorative material,[4] increasing the filler content in the composition, and use of ring opening monomer in recent years.[5]
Packable resin composites are introduced to market as an alternative to amalgam. They are characterized by a high filler load and are indicated for stress bearing posterior restorations with improved handling property.[6] Despite being more favorable, concerns related to their ability to sufficiently wet and adapt to cavity walls especially at the cervical margins apical to cement enamel junction (CEJ) has been raised. Flowable resin composites are used as liners to address this concern.[7]
Flowable resin composites introduced in late 1996 by Bayne have a filler size similar to hybrid resin composites but with a lower filler content. A reduced microleakage was revealed at the cervical margins of class II restorations with the use of them as they act as stress-absorbing layers between the hybrid resin composite and the tooth structure.[3]
Siloranes, a new class of ring opening monomers, were synthesized to overcome the problems related to polymerization shrinkage. This new type of monomer is obtained from the reaction of oxirane and silorane molecules with a volumetric shrinkage determined to be 0.99 volume %. The compensating mechanism for stress in this new system is achieved by opening and extending of the oxirane ring during polymerization to compensate volume reduction.[5,8]
Class II restorations with resin composites can be placed at an acceptable standard if the gingival margin is in sound enamel, but there is much debate regarding marginal integrity that extend apical to CEJ.[7] Hence, the purpose of the study was to evaluate and compare microleakage and microgap formation in class II cavities at the gingival margin placed above and below CEJ, and restored with silorane resin composite and a packable methacrylate resin composite with and without the use of a flowable resin composite liner.
MATERIALS AND METHODS
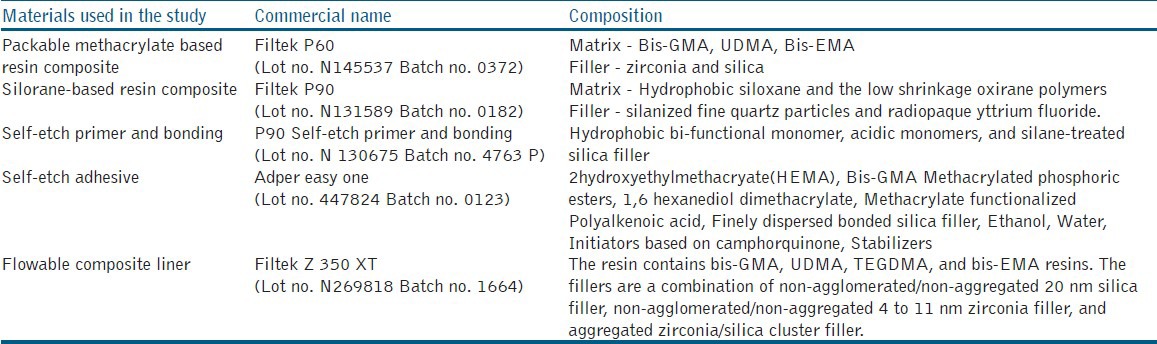
Sixty human maxillary premolar teeth extracted for orthodontic purpose without any structural defects were collected, cleaned with ultrasonic scaler to remove the surface deposits, and stored at room temperature in deionized water with 0.1% thymol. The teeth were used within three months after extraction. The teeth were randomly divided into three groups, each group containing 20 teeth (n = 20) according to the restoration planned. The product profile of the restorative materials used in the study is shown in Table 1.
Table 1.
Product profile of restorative materials used in the study
Cavity preparation
The teeth were mounted in metal jaws with minimum one tooth on either side and with good contact to simulate the clinical situation. Class II box only preparations were done on the mesial (subgroup A) and distal surface (subgroup B) of each tooth with the gingival margin 1 mm above and below cemento enamel junction, respectively. Bucco lingual width of the cavities was 1/3rd of the bucco lingual width of the teeth. The buccal and lingual walls were approximately parallel and connected to gingival seat with rounded line angles. The axial depth was 2 mm. Gingival margins were not beveled but smoothened using gingival marginal trimmer. All the preparations were done using 245 tungsten carbide bur (Dentsply, India) with a high-speed hand piece with copious air water spray. The bur was replaced after every six preparations.
Matrix application
Tofflemire universal metal matrix band and retainer (GDC, India) was adapted to the prepared cavity and stabilized with the help of a wedge.
Restoration
Group I — Filtek P90 self-etch primer and bond (3M ESPE MN USA) was applied to the prepared cavity according to the manufacturer's instructions and light-cured for 10 seconds using LED light-curing unit. Silorane resin composite (Filtek P90, 3M ESPE MN USA) was then placed in the cavity with each increment cured for 20 seconds. Group II — Restoration was done with a packable methacrylate resin composite (Filtek P60, 3M ESPE MN USA) with self-etch adhesive (Adper easy one, 3M ESPE MN USA) as per the manufacturer's instructions. Group III — Self-etch adhesive (Adper easy one, 3M ESPE MN USA) was applied to the prepared cavity, air-dried for 5 seconds, and light-cured for 10 seconds, following which a flowable resin composite (Filtek Z 350 XT, 3M ESPE MN USA) liner was placed to a thickness of 1 mm for the gingival seat. Restoration was done similar to group II.
Finishing and polishing of all the restorations was done using composite finishing kit (EVE composite finishing kit, Germany). Teeth were stored in deionized water for 15 days at room temperature and themocycled for 1500 cycles at 5 and 55 degree centigrade with a dwell time of 30 seconds and a transfer time of 10 seconds.
Preparation of specimens for scanning electron microscope (SEM)
The apices of teeth were sealed with utility wax before painting them with two coats of nail varnish, except 1 mm beyond the margins of the restoration and allowed to air dry. The teeth were immersed in 50% silver nitrate dye for 6 hours and then placed in photographic film developing solution for 4 hours. Then, the specimens were cleaned in running tap water for 2 minutes and sectioned mesiodistally through the center of the restorations with water-cooled diamond disk to obtain two sections. The prepared specimens were mounted on a metal table, gold sputtered for observation under SEM (Cambridge S 200, Germany) at a magnification between 100-500X. The length of dye penetration and microgap at the tooth restoration interface was measured using the grid option.
The data was tabulated and subjected to statistical analysis using Kruskal-Wallis ANOVA and Mann-Whitney U test using SPSS version 18. The significance level was set at P = 0.05
RESULTS
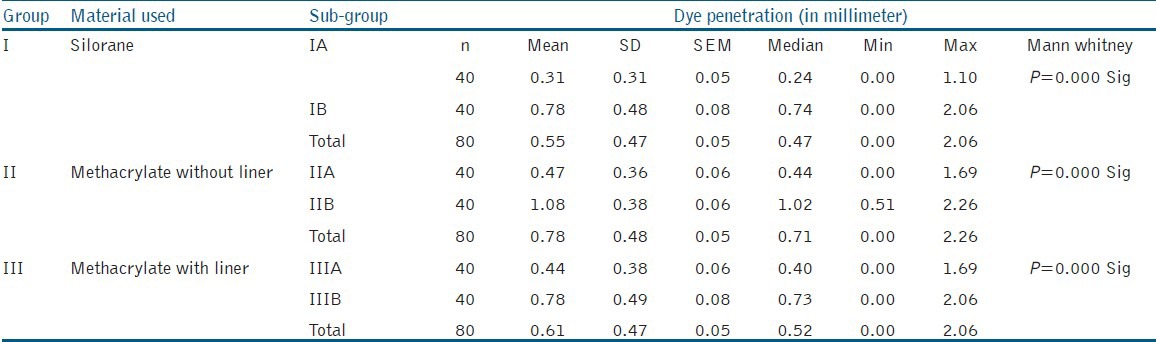
Comparison of subgroup A and B in each group for microleakage showed statistically significant difference with P < 0.001, subgroup A showing less leakage as shown in Table 2.
Table 2.
Comparison of sub groups A and B within each group for microleakage at the gingival margin
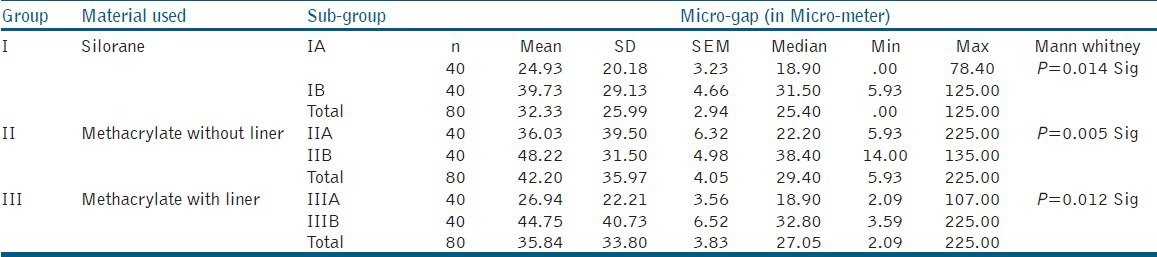
Comparison of subgroup A and B in each group for microgap showed less gap formation for subgroup A with P values 0.014, 0.005, and 0.012 as shown in Table 3.
Table 3.
Comparison of sub groups A and B within each group for microgap at the gingival margin
Intergroup comparison of subgroup A for microleakage did not show statistically significant difference. Intergroup comparison of subgroup B showed statistically significant difference between group I and group II (P < 0.003) and group III and group II (P < 0.002) as shown in Table 4.
Table 4.
Inter group comparison of sub-group B for microleakage at gingival margin placed below CEJ

There was statistically no significant difference between the groups for microgap formation.
DISCUSSION
Restoring class II cavities with resin composites has always been a point of debate in deep cavities where there is no enamel and the cavity margins are formed of dentin, cementum, or both.[9] Bonding to dentin is more difficult to achieve due to the specific properties of dentin such as tubular structure and intrinsic wetness.[10] Hence, in the present study, class II box cavities were prepared to evaluate the effectiveness of the studied materials when the gingival margins are placed above and below cemento enamel junction (CEJ).
The teeth were mounted in metal jaws with minimum one tooth on either side and in good contact to simulate the clinical situation, which also helps in stabilizing the band, enhancing the packing of material into the prepared cavity. No. 245 tungstun carbide bur was used for the preparation of cavities in a high speed handpiece with copious air water spray, as diamond abrasives create a thicker smear layer, which may affect the resin impregnation and thus the bond strength as observed in previous studies.[11] A tofflemeir metal matrix band was used during restoration as they can be better contoured than a clear polyester matrix and offers resistance to condensation of restorative material, which is especially important when a packable resin composite is used. No significant problems are experienced in placing and curing composite material when using a metal matrix as long as small incremental additions are used.[12]
The cavities were restored using oblique incremental technique, which helps to minimize the curing shrinkage by lowering the configuration factor (C-factor). The C factor is the ratio between the bonded and the free surfaces of the cavity. High C factor values can cause adhesion breakdown between the restoration and cavity wall.[10,13] C factor for dental restorations typically ranges from 0.1 to 5, with higher values indicating a greater likelihood of high interfacial stress.[12] C factor in class II restorations is 2, and the restorations are susceptible to adhesive breakdown during curing. Oblique incremental technique with increment of 1-1.5 mm thickness produce lowest C factor.[9] The rationale of this concept is that the margin integrity would be improved regardless of the light-curing method or rate because the occlusal most layer would never be tied simultaneously to both facial and lingual enamel margins. Small increments with greater free surfaces in lieu of bonded ones would compensate for polymerization stress rendering a better integration the resin composite and tooth structure. This result in a better-sealed restoration and limit the contraction forces between opposing walls, reducing stress build up and gap formation.[14]
The use of flowable resin liners at a thickness of 0.5 to 1 mm under packable resin composites may be favorable because of their ability to sufficiently wet and adapt to cavity walls.[3] Hence, in the present study, flowable resin liner is used at a thickness of 1 mm in one of the test groups.
The thermal changes in the mouth are important factors from the point of microleakage and durability of the restoration due to disparity in contraction and expansion between the tooth and the restoration. Therefore, the specimens were thermocycled at 5 and 55 degree centigrade for 1500 cycles to mimic the oral environment. Silver nitrate dye was used to assess the microleakage in the present study, and the specimens were observed under SEM as it provides high magnification and the grid option helps in measuring microleakage and microgap.[15]
The present study was intended to compare silorane resin composite (Group I), methacrylate resin composite (Group II), and methacrylate resin composite with flowable resin liner (Group III) in class II cavities for microleakage and microgap formation along the gingival margin, placed above CEJ (subgroup A) and below CEJ (subgroup B). Subgroup A performed better than subgroup B in all the groups. However, none of the specimens was free of microleakage or microgap formation. This observation is similar to the observations in many previous studies, which demonstrate that the gingival margins placed below CEJ are potentially a greater source of marginal leakage in class II resin composite restorations compared to the margins placed above CEJ.[3,4,6,7,8,10,14,16,17,18] The reason for this is attributed to the complex nature of the substrate (cementum/dentin). Cementum in the cervical area is acellular inserted by sharpeys fibers. The overall degree of mineralization is about 45-60%. High organic content reduces the resin infiltration resulting in poor bonding.[19] Difficulty in bonding to dentin is due to the complex histological structure and variable composition. Dentin is also 45% inorganic, and dentinal hydroxyapatite is randomly arranged in an organic matrix that primarily consists of type I collagen. Dentin is intimately connected with the pulp, and numerous fluid filled channels or tubules traverse through dentin from pulp to dentino enamel junction. This fluid may interfere with adhesion, as hydrophobic resins do not adhere to hydrophilic substrate even if resin tags are formed in the dentin tubule.[20]
Intergroup comparison of subgroup A did not show statistically significant difference, whereas there was difference between the groups in subgroup B. Group IB and group IIIB showed less leakage compared to group IIB. In group IB, silorane resin composite was used, a new class of resin composite, which is proved to have less polymerization shrinkage (0.99% by vol.) compared to methacrylate resin composites (2-5% by vol.). The silorane resin monomer is described as an arrangement of siloranes and oxiranes combining the properties of both, such as biocompatibility, hydrophobicity, high reactivity, and low shrinkage. The silorane system uses ring-opening polymerization compared to free radical polymerization of dimethacrylate monomers.[21] Therefore, a significantly lower polymerization shrinkage and lower stress development occurs, which may be reason for superior marginal integrity.
Group IIB and group IIIB were restored using the same bonding agent and restorative resin. The superior performance of group IIIB may be due to the use of a flowable liner, which reduces the shrinkage stress and improves the marginal adaptation. This observation is in accordance with previous studies who demonstrated significantly less microleakage with the use of a flowable resin liner under condensable methacrylate resin composites.[2,5,8,9,10,22] The advantage is related to the low modulus of elasticity of flowable resins, which absorb stress when the restorative resin shrinks over them and transmit the contraction force to the adjacent tooth structure. But, some researchers have questioned the use of a flowable resin under the restorative resin at the gingival margins. In their studies,[9,23] they have not found improved marginal sealing and felt that the absence of enamel at the gingival cavosurface margin of the proximal box results in low bond strength. The difference in coefficient of thermal expansion and the elastic modulus between the resin and the tooth structure may result in stress and the interfacial gap leading to microleakage. According to some authors, the higher resin content of flowable liner results in greater polymerization shrinkage and more marginal leakage.[24] The possibility of this effect may be due to the increased thickness of flowable resins used, which would lead to greater volumetric contraction as explained by Juan Carlos et al.
However, the samples evaluated in this investigation were prepared on bench top with adequate visualization, moisture control, and ideal access, which may not be the situation in a clinical case. Additional in vivo studies evaluating the long-term clinical performance are needed for a better insight into the efficacy of the restorative materials in class II cavity preparations.
CONCLUSIONS
Within the limitations and the parameters considered in the present study, it can be concluded that
None of the restorative materials tested in the study totally prevented microleakage and microgap formation along the gingival seat in class II cavities.
Silorane resin composite and methacrylate resin composite with flowable resin liner demonstrated better performance compared to methacrylate packable resin without liner, when the gingival margin is placed below CEJ.
All the study groups showed significantly less microleakage and microgap formation when the gingival margin is placed above CEJ.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Watts DC, Hindi A. Intrinsic soft start polymerization shrinkage — kinetic in an acrylic based resin composite. Dent Mater. 1999;15:39–45. doi: 10.1016/s0109-5641(99)00012-3. [DOI] [PubMed] [Google Scholar]
- 2.Going RE. Microleakage around dental restorations: A summarizing review. J Am Dent Assoc. 1972;84:1349–57. doi: 10.14219/jada.archive.1972.0226. [DOI] [PubMed] [Google Scholar]
- 3.Sadeghi M, Lynch CD. The effect of flowable materials on the microleakage of class II composite restorations that extend apical to cemento enamel junction. Oper Dent. 2009;34:306–11. doi: 10.2341/08-91. [DOI] [PubMed] [Google Scholar]
- 4.Ymazaki PC, Bedran-Russo AK, Pereira PN, Swift EJ. Microleakage evaluation of new low shrinkage composite restorative material. Oper Dent. 2006;31:670–6. doi: 10.2341/05-129. [DOI] [PubMed] [Google Scholar]
- 5.Weinmann W, Thalackar C, Guggenberger E. Siloranes in dental composites. Dent Mater. 2005;21:68–74. doi: 10.1016/j.dental.2004.10.007. [DOI] [PubMed] [Google Scholar]
- 6.Attar N, Turgut MD, Gungor HC. The effect of flowabe resin composites as gingival increments on the microleakage of posterior resin composites. Oper Dent. 2004;29:162–7. [PubMed] [Google Scholar]
- 7.Tredvin CJ, Stokes A, Moles DR. Influence of flowable liner and margin location on microleakage of conventional and packable class II resin composites. Oper Dent. 2005;30:32–8. [PubMed] [Google Scholar]
- 8.Boaro LC, Gonçalves F, Guimarães TC, Ferracane JL, Versluis A, Braga RR. Polymerization stress, shrinkage and elastic modulus of current low shrinkage restorative composites. Dent Mater. 2010;26:1144–50. doi: 10.1016/j.dental.2010.08.003. [DOI] [PubMed] [Google Scholar]
- 9.Radhika M, Sajjan GS, Kumaraswamy BN, Mittal N. Effect of different placement techniques on marginal microleakage of deep class II cavities restored with two composite resin formulations. J Conserv Dent. 2010;13:9–15. doi: 10.4103/0972-0707.62633. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bagis YH, Baltacioglu IH, Kahyaogullari S. Comparing microleakage and layering methods of silorane based resin composite in wide class II MOD cavities. Oper Dent. 2009;34:578–85. doi: 10.2341/08-073-LR. [DOI] [PubMed] [Google Scholar]
- 11.Von Fraunhofer JA, Smith TA, Marshall KR. The effect of multiple use of disposable diamond burs on restoration leakage. J Am Dent Assoc. 2005;13:53–7. doi: 10.14219/jada.archive.2005.0026. [DOI] [PubMed] [Google Scholar]
- 12.Hegde J, Sravanti Y. An in vitro comparison of adhesive techniques and rotary instrumentation on shear bond strength of nano composite with simulated pulpal pressure. J Conserv Dent. 2011;14:228–32. doi: 10.4103/0972-0707.85794. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Braga RR, Ballester RY, Ferracane JL. Factors involved in the development of polymerization shrinkage stress in resin composites: A systematic review. Dent Mater. 2005;21:962–70. doi: 10.1016/j.dental.2005.04.018. [DOI] [PubMed] [Google Scholar]
- 14.Chuang SF, Jin YT, Chang CH, Garcia-Godoy F. Effect of lining material on microleakage and internal voids of class II resin based composite restorations. Am J Dent. 2003;16:84–90. [PubMed] [Google Scholar]
- 15.Gonzalez NA, Kasim NH, Aziz RD. Microleakage testing. Ann Dent. 1997;4:31–7. [Google Scholar]
- 16.Kusgoz A, Ulcer M, Yesilyurt C, Yoldas OH, Ozil M, Tanrier M. Silorane based composite: Depth of cure, surface hardness, degree of conversion and cervical microleakage in class II cavities. J Esthet Restor Dent. 2011;23:324–35. doi: 10.1111/j.1708-8240.2011.00411.x. [DOI] [PubMed] [Google Scholar]
- 17.Gao BT, Lin H, Han JM, Zheng G. Polymerization characteristics, flexural modulus and microleakage evaluation of silorane based and methacrylate based composites. Am J Dent. 2011;24:97–102. [PubMed] [Google Scholar]
- 18.Idriss S, Abduljabbar T, Habib C, Omar R. Factors associated with microleakage in class II resin composite restorations. Oper Dent. 2007;32:60–6. doi: 10.2341/06-16. [DOI] [PubMed] [Google Scholar]
- 19.Santini A, Miletic V. Comparison of the hybrid layer formed by silorane adhesive, one step self etch and etch and rinse system using confocal micro raman spectroscopy and SEM. J Dent. 2008;36:683–91. doi: 10.1016/j.jdent.2008.04.016. [DOI] [PubMed] [Google Scholar]
- 20.Swift EJ, Jr, Perdigão J, Heymann HO. Bonding to enamel and dentin: A brief history and state of the art. Quintessence Int. 1995;26:95–110. [PubMed] [Google Scholar]
- 21.Duarte S, Jr, Botta AC, Phark JH, Sadan A. Selected mechanical and physical properties, and clinical application of a new low shrinkage composite restoration. Quintessence Int. 2009;40:631–8. [PubMed] [Google Scholar]
- 22.Chuang SF, Jin YT, Liu JK, Chang CH, Shieh DB. Influence of flowable composite lining thickness on class II composite restorations. Oper Dent. 2004;29:301–8. [PubMed] [Google Scholar]
- 23.Peutzfeldt A, Asmussen E. Composite restorations: Influence of flowable and self curing resin composite lining on microleakage in vitro. Oper Dent. 2002;27:569–76. [PubMed] [Google Scholar]
- 24.Ziskind D, Adell I, Teperovich E, Peretz B. The effect of an intermediate layer of flowable composite resin on microleakage in packable composite restorations. Int J Paediatr Dent. 2005;15:349–54. doi: 10.1111/j.1365-263X.2005.00663.x. [DOI] [PubMed] [Google Scholar]