

INTRODUCTION
Population ageing is one of the most discussed global phenomena in the present century. Countries with a large population like India have a large number of people now aged 60 years or more. The population over the age of 60 years has tripled in last 50 years in India and will relentlessly increase in the near future. According to census 2001, older people were 7.7% of the total population, which increased to 8.14% in census 2011. The projections for population over 60 years in next four censuses are: 133.32 million (2021), 178.59 (2031), 236.01 million (2041) and 300.96 million (2051). The increases in the elderly population are the result of changing fertility and mortality regimes over the last 40-50 years.[1,2]
The elderly process is considered to be an end product of demographic transition or demographic achievement with a decline in both birth and mortality rates and consequent increase in life expectancy at birth and older ages. The expectancy of life at birth during the year 2006-2011 was 65.65 and 67.22 for male and female respectively while projected expectancy of life at birth during the year 2011-2016 will be 67.04 and 68.8 years for males and females respectively. Irrespective of socio-economic status, the non-communicable diseases (NCDs) requiring large quantum of health and social care are extremely common in old age. Disabilities resulting from these NCDs are very frequent, which affects the activities of daily living. The management of these chronic diseases is also very costly, especially for cancer treatment, joint replacements, heart surgery, neurosurgical procedures etc., thereby making it out of pocket for elderly persons. The 60th round of National Sample Survey provides a comprehensive status report on older persons. According to this survey, the prevalence and incidence of diseases as well as hospitalization rates are much higher in older people than the total population. It also reported that about 8% of older Indians were confined to their home or bed. The proportion of such immobile or home bound people rose with age to 27% after the age of 80 years. Women were more frequently affected than males in both rural and urban areas. The survey revealed that a good or fair condition of health was reported by 55-63% of people with a sickness and 77-78% of people without one. In contrast about 13-17% of the survey population without any sickness reported ill-health. It is possible that many older people take ill health in their stride as a part of “usual/normal ageing.” This observation has a lot of significance as self-perceived health status is an important indicator of health service utilization and compliance to treatment interventions.[3]
However, very little effort has been made to develop a model of health and social care in tune with the changing need and time. The developed world has evolved many models for elderly care, e.g., nursing home care, health insurance etc., As no such model for older people exists in India, as well as most other societies with similar socio-economic situation, it may be an opportunity for innovation in the health system development, though it is a major challenge. The requirements for health-care of the elderly are also different for our country. India still has family as the primary care giver to the elderly and scope for training this lot provide support to the program. Presently, the elderly are provided health-care by the general health-care delivery system in the country.
As the elderly population is likely to increase in the future, and there is a definite shift in the disease pattern, i.e. from communicable to non-communicable, it is high time that the health care system gears itself to growing health needs of the elderly in an optimal and comprehensive manner. There is a definite need to emphasize the fact that disease and disability are not part of old age and help must be sought to address the health problems. The concept of Active and Healthy ageing needs to be promoted among the elderly, which includes preventive, promotive, curative and rehabilitative aspects of health.[4]
VISION AND OBJECTIVES OF THE NATIONAL PROGRAM FOR THE HEALTH-CARE FOR THE ELDERLY (NPHCE)
The NPHCE is an articulation of the International and national commitments of the Government as envisaged under the UN Convention on the Rights of Persons with Disabilities, National Policy on Older Persons adopted by the Government of India in 1999 and Section 20 of “The Maintenance and Welfare of Parents and Senior Citizens Act, 2007” dealing with provisions for medical care of Senior Citizen. The Vision of the NPHCE are: (1) To provide accessible, affordable, and high-quality long-term, comprehensive and dedicated care services to an ageing population; (2) Creating a new “architecture” for Ageing; (3) To build a framework to create an enabling environment for “a Society for all Ages;” (4) To promote the concept of Active and Healthy Ageing.
SPECIFIC OBJECTIVES OF NPHCE
To provide an easy access to promotional, preventive, curative and rehabilitative services through community based primary health-care (PHC) approach
To identify health problems in the elderly and provide appropriate health interventions in the community with a strong referral backup support
To build capacity of the medical and paramedical professionals as well as the care-takers within the family for providing health-care to the senior citizen
To provide referral services to the elderly patients through district hospital regional medical institutions
Convergence with National Rural Health Mission (NRHM), Ayush and other line departments like Ministry of Social Justice and Empowerment.
STRATEGIES TO ACHIEVE THE OBJECTIVES OF THE NPHCE
Community based PHC approach including domiciliary visits by trained health-care workers
Dedicated services at PHC/Community Health Center (CHC) level including provision of machinery, equipment, training, additional human resources, Information, Education and Communication (IEC), etc.
Dedicated facilities at the district hospital with 10 bedded wards, additional human resources, machinery and equipment, consumables and drugs, training and IEC
Strengthening of 8 Regional Medical Institutes to provide dedicated tertiary level medical facilities for the elderly, introducing PG courses in geriatric medicine, and in-service training of health personnel at all levels
IEC using mass media, folk media and other communication channels to reach out to the target community
Continuous monitoring and independent evaluation of the Program and research in geriatrics and implementation of NPHCE
Promotion of public private partnerships in geriatric health-care
Mainstreaming Ayush – revitalizing local health traditions and convergence with programs of Ministry of Social Justice and Empowerment in the field of geriatrics
Reorienting medical education to support geriatric issues.
THE FOLLOWING ARE THE EXPECTED OUTCOMES OF NPHCE
Regional geriatric centers (RGC) in eight Regional Medical Institutions by setting up RGCs with a dedicated geriatric out-patient department (OPD) and 30-bedded geriatric ward for management of specific diseases of the elderly, training of health personnel in geriatric health-care and conducting research
Post-graduates in geriatric medicine (16) from the eight regional medical institutions
Video Conferencing Units in the 8 Regional Medical Institutions to be utilized for capacity building and mentoring
District geriatric units with dedicated geriatric OPD and 10-bedded geriatric ward in 80-100 District Hospitals
Geriatric clinics/rehabilitation units set up for domiciliary visits in community/primary health centers in the selected districts
Sub-centers provided with equipment for community outreach services
Training of Human Resources in the Public Health-Care System in geriatric care.
PACKAGE OF SERVICES UNDER NPHCE
In the program, it is envisaged providing promotional, preventive, curative and rehabilitative services in an integrated manner for the Elderly in various Government health facilities. The package of services would depend on the level of health facility and may vary from facility to facility. The range of services will include health promotion, preventive services, diagnosis and management of geriatric medical problems (out- and in-patient), day care services, rehabilitative services and home based care as needed. Districts will be linked to RGCs for providing tertiary level care. The services under the program would be integrated below district level and will be an integral part of existing PHC delivery system and vertical at district and above as more specialized health-care are needed for the elderly.
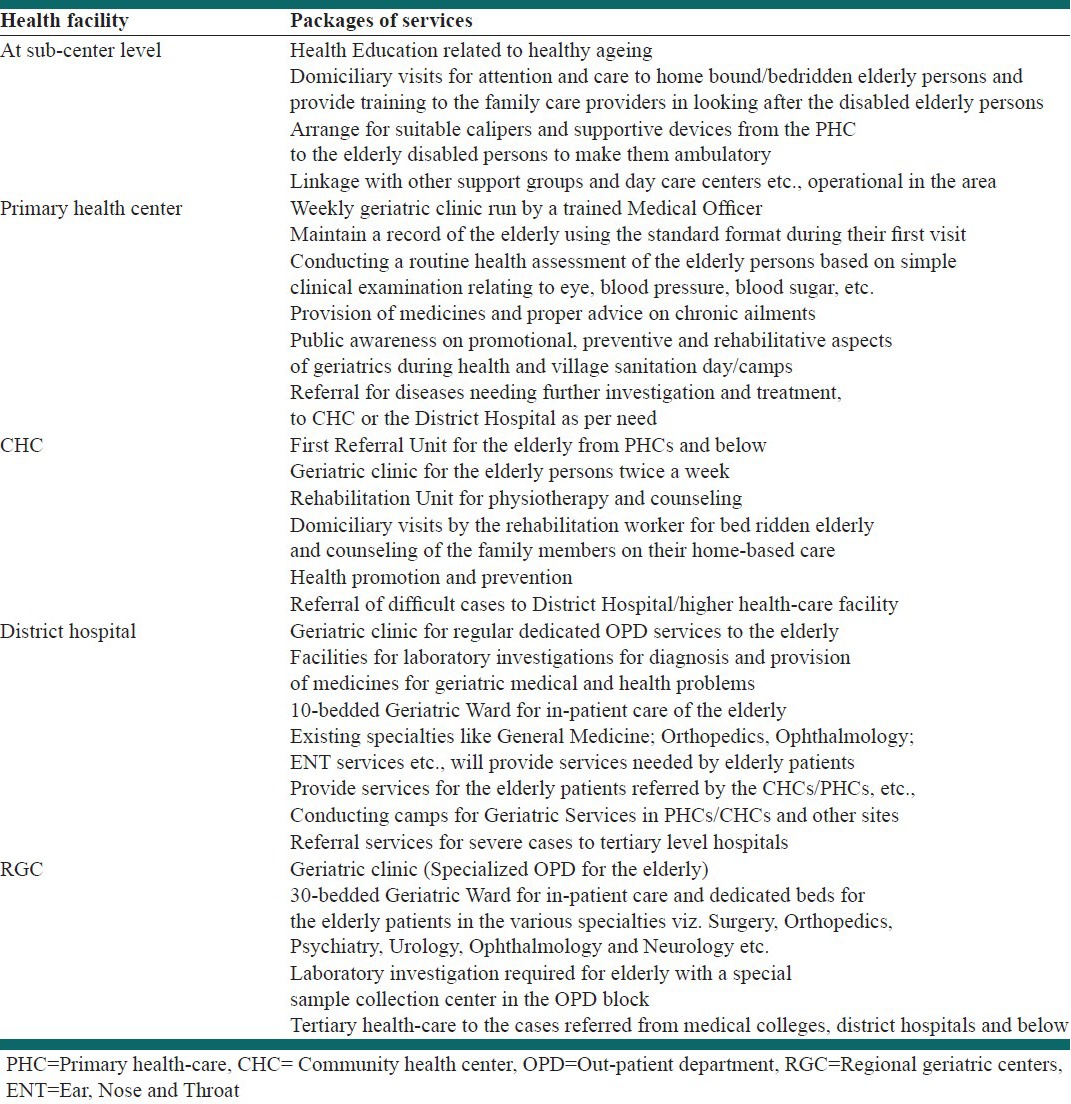
Packages of services to be made available at different levels under NPHCE
In the program, it is envisaged providing promotional, preventive, curative and rehabilitative services in an integrated manner for the elderly in various Government health facilities. The package of services would depend on the level of health facility and may vary from facility to facility. The range of services will include health promotion, preventive services, diagnosis and management of geriatric medical problems (out- and in-patient), day care services, rehabilitative services and home based care as needed. Districts will be linked to RGCs for providing tertiary level care.
The services under the program would be integrated below district level and will be an integral part of existing PHC delivery system and vertical at district and above as more specialized health-care are needed for the elderly.
Institutional framework for the implementation of NPHCE
Financial Management Groups (FMG) of Program Management support units at the state and district level, which are established under NRHM, will be responsible of maintenance of accounts, release of funds, expenditure reports, utilization certificates and audit arrangements. The funds will be released to States/UTs through the State Health Society (SHS) to carry out the activities at different levels as envisaged in the operational guidelines. Funds release from SHS to District Health Society (DHS) would inter alia include funds for CHCs, PHCs and sub-centers to cover the entire District.
Funds from this program will be released to the SHS by the Government of India. SHS will retain funds for state level activity and release grant-in-aid to the DHSs. NPHCE would operate through NCD cells under the program constituted at State and District levels and also maintain separate bank accounts at each level. Funds from Health Society will be transferred to the Bank accounts of the NCD cell after requisite approvals at the appropriate stage. This system will ensure both convergence as well as independence in achieving program goals through specific interventions. It is envisaged to merge the program at State and District into the SHS and DHS respectively in order to ensure sustaining the current momentum and continued focus [Table 1].
Table 1.
Package of services under NPHCE for elderly age group
Although, the NPHCE addresses most of the health problems in an institutional health-care system, but it completely neglects the home based care of an elderly person in families. It would have been better to focus on awareness among families and make them prepare for possible eventualities rather than treating when it happened. Other than having a national vision, the policy should have a decentralized vision that can make the policy demand driven rather than an autocratic state driven system. As in the case of most of the national programs or policies, it also fails to focus on regional issues that are different in different regions. The policy can be a failure in addressing how to generate an incentive for families to treat and care for their elderly, which is so necessary in a poor country like India.[5]
The NPHCE is a good and new initiative to take care of a fast ageing population. It requires more attention in the implementation and coordination so that the program would not only be on paper like many other programs of the country.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Ministry of health and family welfare. New Delhi: Director General of Health Services, MOHFW, Government of India; 2011. National Program for Health Care of the Elderly (NPHCE): Operational Guidelines 2011. [Google Scholar]
- 2.Central Statistics Office. New Delhi: Central Statistics Office Ministry of Statistics and Programme Implementation, Government of India; 2011. Situation Analysis of the Elderly in India. [Google Scholar]
- 3.Central Statistics Office. New Delhi: National Sample Survey Organization, Ministry of Statistics and Programme Implementation, Government of India; 2006. Morbidity, Health Care and the Condition of the Aged. NSSO (64th round) Jan-June 2004. [Google Scholar]
- 4.National Programme for the Health Care of the Elderly (NPHCE): An approach towards active and healthy ageing. Directorate General of Health Services, Ministry of Health and Family Welfare, Government of India. 2011. [Last accessed on 2012 Oct 17]. Available from: http://www.health.bih.nic.in/Docs/Guidelines-NPHCE.pdf .
- 5.National Programme for Health Care of the Elderly. India current affairs 2011. A leading resource of online information of India. [Last accessed on 2012 Oct 20]. Available from: http://www.indiacurrentaffairs.org/