

Abstract
Background:
To compare the level of knowledge, the attitudes, and practices with regards to tobacco use between Iranian students at a public (PBU) and Islamic Azad (IAU) university.
Methods:
A cross-sectional design was used in this study. As the number of students at the IAU were three times greater than that of the PBU, we selected 150 students from the PBU and 450 students from the IAU using simple random sampling. A 57-item survey instrument was utilized for this study. The collected data were recorded by SPSS version 15 software and then it underwent statistical analysis using descriptive statistics and ANOVA to compare the difference between means of knowledge, attitude and practice scores. Logistic regression analysis was conducted to identify variables that have an independent association with students smoking and to describe possible variations in these relationships. The P value level for statistical significance was set at 0.05.
Results:
From participants, 46.8% were females, 10% of 327 students reported being daily smokers; of these, 84% were from the IAU. Totally, among the 107 smokers, 61 (57%) and 29 (27.1%) were water pipe and cigarettes smokers, respectively. Ninety-three IAU students (21.7%) and 30 PBU students (20.7%) reported smoking during the past 30 days. The mean of the knowledge items between the students of IAU was lower than PBU students. Female gender, smoking in the home, and allowing visitors to smoke in the home were significant predictors of smoking in the past 30 days in PBU, respectively. In IAU, female gender, smoking by friends, and health status were predictors for smoking in the past 30 days.
Conclusions:
Future studies should assess the factors affecting smoking initiation, as well as effective techniques for the prevention of smoking initiation and substance abuse in Iranian adolescents and young adults.
Keywords: Engineering students, smoking, tobacco use, university
INTRODUCTION
Tobacco use is the leading cause of preventable death worldwide. Globally, each year, smoking kills nearly 6 million people and causes hundreds of billions of dollars of economic losses. A disproportionately higher number of individuals who succumb to the adverse effects of tobacco use reside in low and middle-income countries and this disparity is expected to widen further over the next several decades.[1] Tobacco products contain the dried, processed leaves of the tobacco plant Nicotiana rustica or Nicotania tabacum, which is harmful to human health.[2]
Smoking costs over a lifetime for a man and for a woman have been reported as $106,000 and $220,000, respectively. Thus, the cost of cigarettes is an economic burden, not only to society, but also to the individual smoker and his/her family.[3]
Smoking adversely affects all body systems and can severely affect a smoker's health. Smoking causes coronary heart diseases, blood vessel constriction, and the nicotine there in stimulates adrenal epinephrine secretion, which increases blood pressure and heart rate.[4,5] In addition, smoking is a leading cause of respiratory diseases such as emphysema, bronchitis, pneumonia and chronic airway obstruction by damaging the airways and alveoli of the lung.[4,6] There is a direct relationship between the number of years of smoking and lung cancer.[3] Tobacco users are at risk for several other types of cancers such as carcinoma of the upper respiratory tract, cervix, throat, larynx, mouth, pancreas, kidney, bladder and acute myeloid leukemia.[2,3,7]
In developed countries, mean smoking prevalence has been reported as 42% in men and 24% in women, while in less developed nations, an average of 48% of men and 7% of women smoke. In the U.S., smoking prevalence is estimated at 28% and 23% for men and women, respectively.[8] Forty percent of Cubans smoke, as do 37% of Kuwaitis, Chileans, Russians, Belarusians and Bangladeshis while only 6% of Nigerians, 8% of Salvadorans, and 8% of Ghanaians smoke. High smoking rates have been recorded in the former Soviet countries in the Commonwealth of Independent States (CIS) (29%), Central Europe (29%), and the European Union (28%).[9]
According to the 2001 National Household Survey on Drug Abuse, about 66.5 million Americans reported past month use of a tobacco product, of which, 24.9% smoked cigarettes, while 5.4% used cigars, 1.0% smoked pipes, and 3.2% used smokeless tobacco.[2] Data analyzed from the 1999 and 2000 National Youth Tobacco Survey, which was conducted across U.S. middle schools and high schools showed that 48.6% of U.S. adolescents had at least experimented with tobacco and 7.8% were established smokers.[10]
One investigation conducted in Tehran, Iran, showed that the mean prevalence of smoking was 11.9%, of which 20.6% of the male and 2.9% of the female participants were smokers. These percentages increased significantly until age 54. Additionally, married people, and individuals with higher education levels smoked more.[11] Similarly, a subsequent report of adult smoking in Tehran found that 21.3% of males and 3.4% of females were current smokers.[12]
According to a study done on a sample of 1,964 students from public and private universities in Beirut, Lebanon, the overall prevalence of smoking was 40%. Most smoked narghile only (21.1%), while 7.6% smoked only cigarettes and 11.3% were dual users of both cigarettes and narghile.[13] Smoking rates between Iranian university students ranged from 7-52% with much higher usage among male students.[14,15,16,17,18] For example, a study of 950 university students in Kerman, Iran revealed that approximately 40% of male students and 5.8% of the female students were smokers. Male gender, higher income, lower average exam scores, and a close friend's smoking were factors associated with increased likelihood of smoking cigarettes.[18]
The aim of this study was to compare the level of knowledge, the attitudes, and practices with regards to tobacco use between Iranian engineering students at a PBU and an IAU.
METHODS
This cross-sectional study was performed during 2011. Considering the engineering student population at the two universities (IAU, 6000 students; PBU, 2000 students). As the number of students at the IAU was three times greater than that of the PBU, we randomly selected 150 students from the public university and 450 students from the IAU using simple random sampling. Then we randomly selected students of different engineering disciplines to participate in the survey.
A 57-item survey instrument originally developed by researchers at the Indiana University School of Dentistry to assess the tobacco knowledge, attitudes and practices among health professions students was utilized for this study. It was modified by the addition of four demographic questions. The survey questionnaire was composed of two sections; the first section included 33 tobacco knowledge and attitude items, while the second section included 28 questions about the demographic characteristics and the smoking history of the participants. The first 16 survey items related to tobacco knowledge; responses for these items were based on a 5-point scale (strongly agree, agree, neither agree nor disagree, disagree and strongly disagree). The correct answer was coded as “1” and others were coded as “zero”. So the maximum knowledge score was 16 and the minimum was 0. The second six questions[17,18,19,20,21,22] represented attitude items; response choices were “low”, “moderate” and “high”. The ideal answer was coded “1” and other responses were coded as “zero”, so the maximum attitude score was 6, while the minimum was 0. The demographic items (questions 35-37) included age, sex, and health status (self-explanatory). Between the remaining questions, because they had the same weighting, seven questions with dichotomous response choices were selected to represent the tobacco practices of respondents. Thus, the maximum practice score was 7 and the minimum was 0.
These survey items were numerically coded. The questionnaire was translated into Persian and then translated into English and retranslated into Persian by another group and the content validity of the questionnaire was confirmed. The reliability coefficient for the knowledge items using Kuder Richardson test for reliability was 0.706 and for attitude and practice items using Cronbach's α internal consistency coefficient were 0.702 and 0.735, respectively. This study was approved by Research deputy of Shiraz University of Medical Sciences.
After obtaining oral informed consent, participant received his/her self-reporting questionnaire while in a classroom. Research team members briefly introduced the survey, explained that the survey responses were voluntary and confidential, answered inquiries and distributed the surveys. Participants completed the questionnaires in approximately 10 min. The data were identified and reported only in aggregate form. Survey data underwent coding followed by recording into an electronic database for analyses. The collected data were recorded by SPSS version 15 software and then it underwent statistical analysis using descriptive statistics and ANOVA to compare the difference between means of knowledge, attitude and practice scores, also logistic regression analysis using a multivariable regression model to the data on tobacco smoking status, separately for PBU and IAU students. In this study, the P value level for statistical significance was set at 0.05.
RESULTS
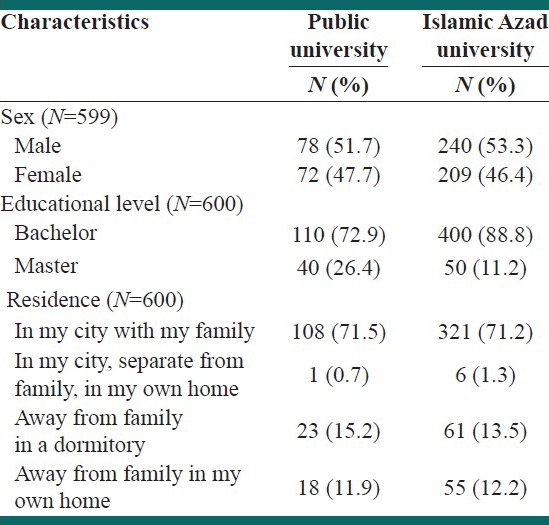
In this study, 600 engineering students were participated and because of the replacement of potential participants who did not choose to complete the survey (by going to the next his/her classmate), response rate was 100%. Of the participants, 46. 8% were females [Table 1]. The mean age of participants was 21 years in the IAU and 23 years in the PBU.
Table 1.
Demographic characteristics of study participants from engineering programs at two Iranian universities
Among the engineering students, there were 33 (10%) out of 327 students who reported being daily smokers; of these, 84% were from the IAU and 16% from PBU [Table 2]. Totally, among the smokers, 61 (57%) and 29 (27.1%) of 107 were water pipe and cigarettes smokers, respectively [Table 2].
Table 2.
Comparison of tobacco use by engineering students at a public and Islamic Azad Universities
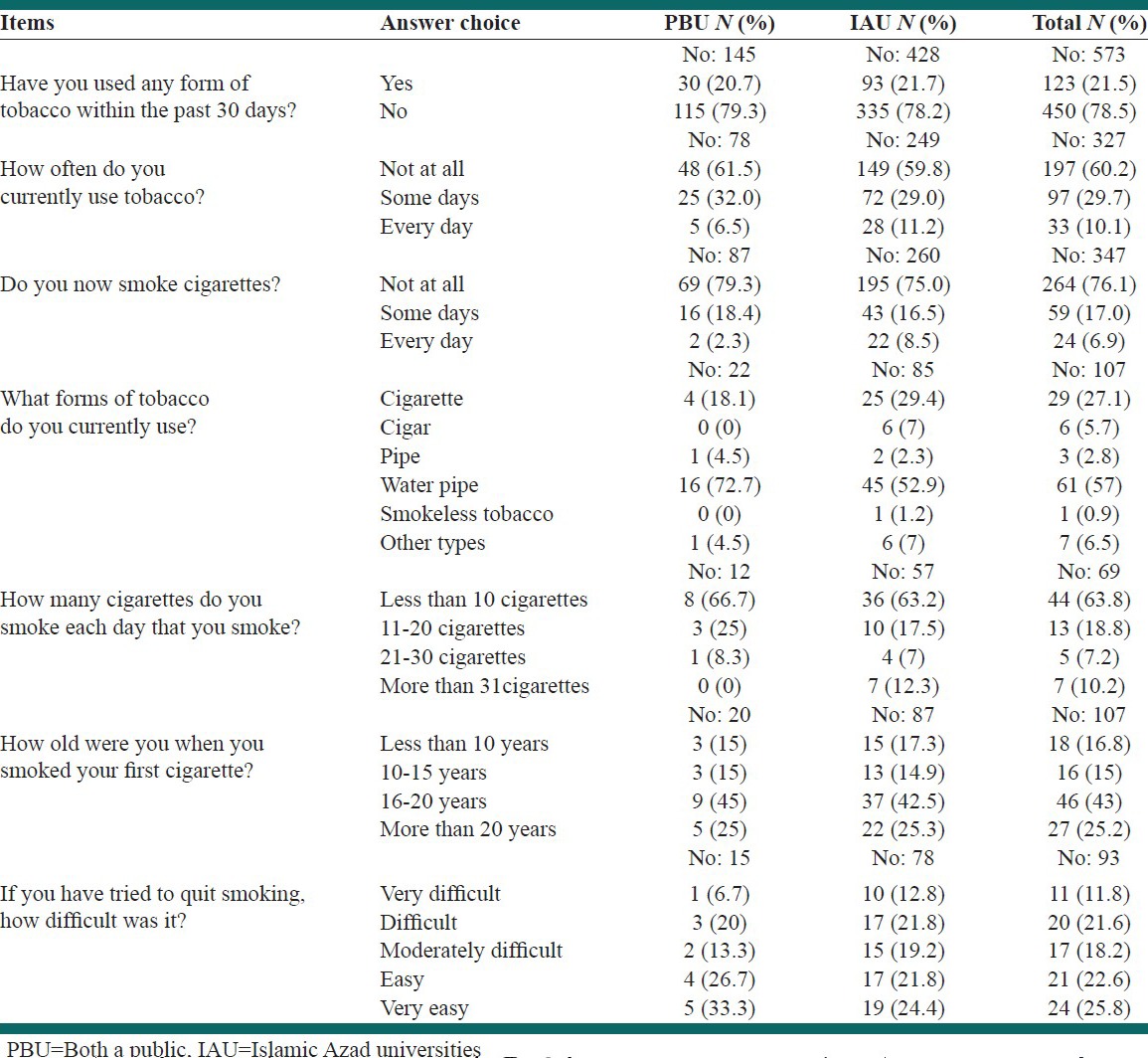
Of students reporting that they smoked at least 100 cigarettes in their lifetime, 10 (6.8%, N = 146) were from PBU and 49 (10.9%, N = 425) from IAU students. Among the cigarette smoking students, 7 IAU students smoked more than 31 cigarettes per day, while no PBU students reported smoking that much. At the other end of the spectrum, 36 (63.2%) out of 57 of IAU students and 8 (66.7%) out of 12 of PBU students reported smoking less than 10 cigarettes per day [Table 2]. Of those reporting water pipe smoking, the primary location for doing so was reported by 5.6% (34) of students as a teahouse, while 4.6% said a friend's residence was the primary location, 3.8% indicated hookah smoking at a relatives’ house, and 11.6% of students said that they smoked hookah primarily at locations other than these.
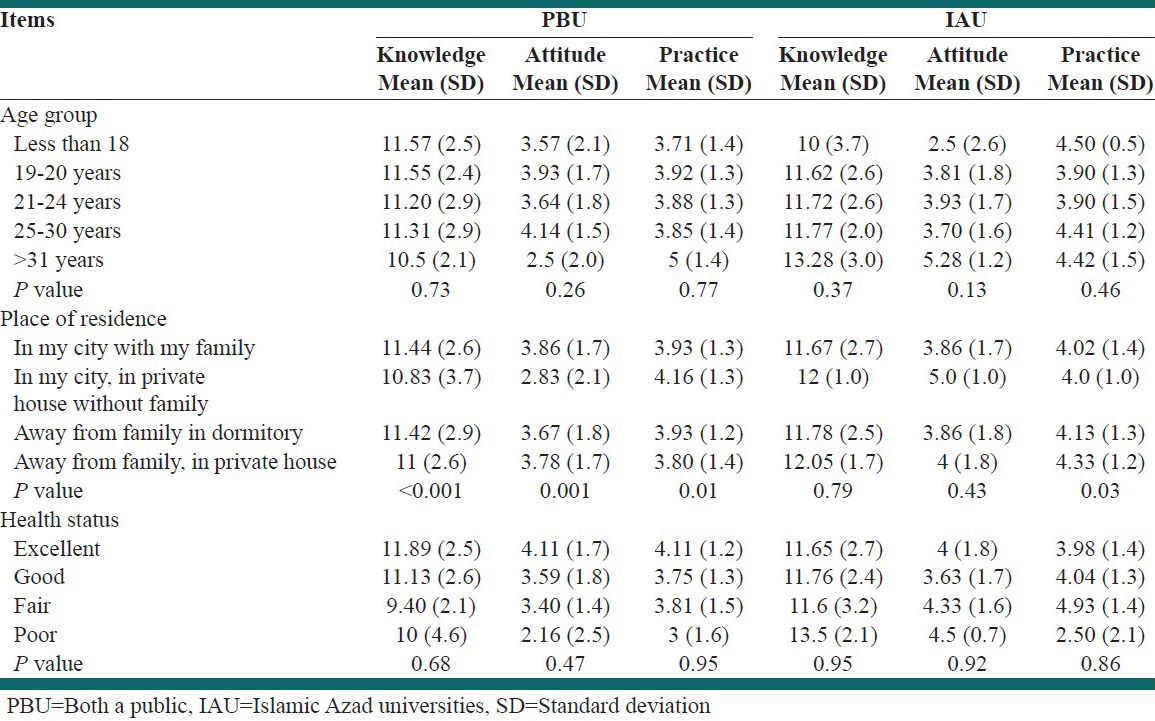
The mean of knowledge, attitude and practices of the students according to the age group, health status and the residence categories is summarized in Table 3. The ANOVA analysis indicated a significant difference regarding the mean of knowledge, attitude and practice according to the residence categories in the IAU students (P < 0.05).
Table 3.
Comparing the mean scores of knowledge, attitude and practice scores between engineering students in both a Public and Islamic Azad Universities
Out of all respondents, ninety-three IAU students (21.7%) and 30 PBU students (20.7%) reported smoking during the past 30 days.
Only 60 IAU students (20%, N = 299) and 16 PBU students (12.9%, N = 124) indicated an intention to quit smoking. Only 20 IAU students (22.7%, N = 88) and 3 PBU students (15.7%, N = 19) indicated that they intend to quit smoking during the next 6 months. However, 41 IAU students (19%, N = 215) and 7 PBU students (12.5%, N = 56) responded that they have tried to quit smoking during the last 2 years. One (6.7%) out of 15 PBU students and 10 (12.8%) out of 78 IAU students reported that quitting smoking was s very difficult [Table 2].
Table 4 shows the predictors of smoking status based on logistic regression model in the public university. Based upon logistic regression analysis, Table 5 describes the predictors of smoking in engineering students at the IAU in Shiraz.
Table 4.
Logistic regression analysis of smoking usage and predictors among engineering students of a public university
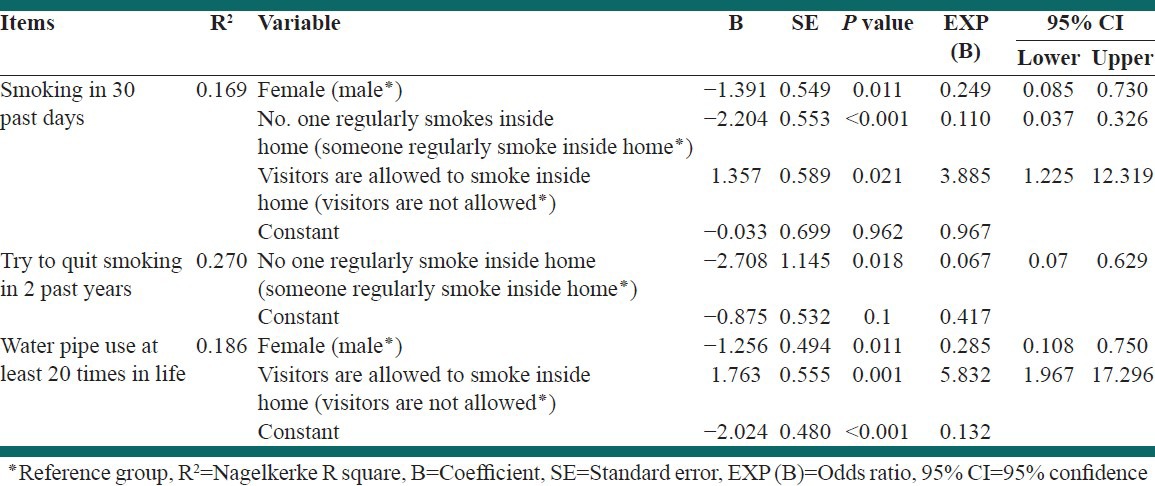
Table 5.
Logistic regression analysis of smoking usage and predictors among engineering students in Azad Islamic university
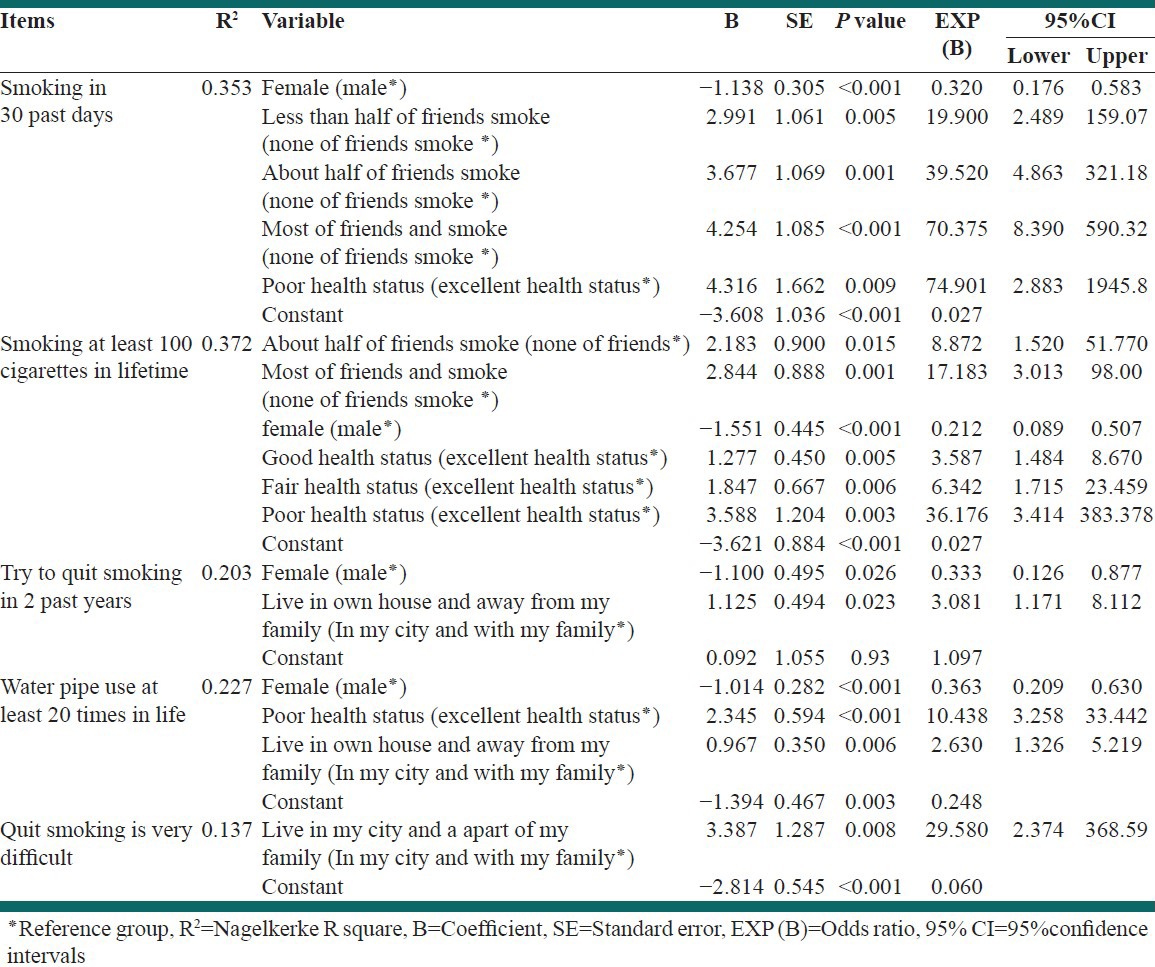
Compared to students who described their health status as “excellent”, smoking in 30 past days was 74 times greater in students describing their health status as “poor”. Compared to students who reported having no smoking friends, smoking at least 100 cigarettes in their lifetime was nearly 8 times greater for students who indicated that half of their friends smoke and 17 times greater for students who reported that most of their friends smoke. Compared with students who reported excellent health status, good, fair, and poor health status were predictors of smoking at least 100 cigarettes in their lifetime with odds 3, 6 and 36 times greater, respectively.
Interestingly, among students who live in their own home away from their family, the odds of attempting to quit smoking during the 2 past years was nearly 3 times greater than for students who live in their hometown and with their family. Reported use of a water pipe at least twenty times was 10 times greater in students with poor health status and 3 times greater in students who lived in their own home away from their family. Reported difficulty in quitting among students who live in their hometown apart from their family was over 29 times greater than among students living with their family.
DISCUSSION
Several investigations were conducted in different countries regarding the smoking behaviors and attitude among students in different fields of study. In the current study, we found that the prevalence of current tobacco consumption was approximately 21.5% and that tobacco use was more prevalent in men. These rates were lower than those of the Kolkata, India study.[19] Additionally, a study which was conducted with public and private university students in Beirut, Lebanon, revealed that the overall prevalence of smoking was 40%,[14] and research from Eskişehir, Turkey found the prevalence of smoking was 42.5%.[20]
In 1993, a Kuwaiti study was conducted concerning the age of smoking initiation among randomly selected male university students. The results showed that almost one tenth of the students initiated cigarette smoking between ages 16 and 17 with the rate of initiation increasing rapidly thereafter and reaching 30% by age 20 and nearly 50% by age 24. In that study, the most important environmental risk factor positively associated with smoking initiation was sibling smoking. Compared to the medical and engineering students, students in other fields of study had a higher risk of smoking initiation;[21] this differs from the current study in which the peak age of smoking initiation was between 16 and 20 years. This may be because at this age the curiosity, opposition of parents, presentation and transmission of sexual and physical maturation from childhood to youth is greater, so smoking is greater. In contrast to the Dar-Odeh et al. study,[22] the highest prevalence of tobacco use in the current study was associated with water pipe (hookah) use. This was not surprising due to its ease of access and availability in nearly every teahouse. As there are few if any educational programs on the risks of tobacco use and available cessation methods in university engineering programs, as found in the current study, there is a tendency for this group of students to have higher levels of tobacco use.
Knowledge score was almost a little higher than 50%, but attitude and behavior scores were almost 50%, which shows that despite a higher awareness of social programs in the media and other areas discussing the disadvantages of smoking, it did not affect the practices and attitude of students. The mean of the knowledge scores between the students was approximately equal in the female and male students in both universities. The attitude score was higher for males of the PBU than of the IAU, while that of females was higher for females of the PBU than females of the IAU. The approximately equal knowledge mean and attitude scores between the students of the two universities indicates that the governmental and social laws may be the most effective way of enhancing smoking knowledge and shaping attitudes among the Iranian student population.
Most respondents believed that quitting is very easy to do. Perhaps this is because for many Iranian student smokers, smoking is more of a habit rather than a true addiction. This may also be due in part to the Islamic culture and laws that discourage smoking because of its harmful effects on the body.
Compared with male students at both universities, female students were less likely to report smoking or use of a water pipe. Among students of IAU, smoking by friends and poor health status were predictors for current smoking or smoking at least 100 cigarettes in their lifetime; this finding was similar to other studies of this issue.[23,24] However, in PBU, smoking by students in the past 30 days, or use of a water pipe at least twenty times was greater in students who allow visitors to smoke in their home. In IAU, the predictors of use of water pipe use were poor health status and living in one's own home away from family.
This study has several limitations; the design of this study was cross-sectional, so it limited the demonstration of risk factors for smoking. In addition, other factors likely affected respondents’ smoking such as: Parental education, parental tobacco use, and psychological and socioeconomic factors, none of which were assessed in the survey. Another limitation is that, this study was conducted with university students so the results may not be generalizable to all youth in the community. Because data was obtained by self-report, there is a likelihood of under-reporting and social desirability bias.
CONCLUSIONS
As a result of this study, some recommendations may be suggested for policy makers and future research. For example, future studies should assess the factors affecting smoking initiation, as well as effective techniques for the prevention of smoking initiation and substance abuse in Iranian adolescents and young adults and on college campuses.
ACKNOWLEDGMENT
The present article was extracted from the thesis written by Moussa Youssef and was financially supported by Shiraz University of Medical Sciences grants No. 3253.
Footnotes
Source of Support: Shiraz University of Medical Sciences grants No. 3523
Conflict of Interest: None declared.
REFERENCES
- 1.WHO report on the global Tobacco epidemic. 2011. [Last accessed on 2012 Aug 20]. p. 7. Available from: http://www.whqlibdoc.who.int/publications/2011/9789240687813_eng.pdf .
- 2.Center for Substance Abuse Research [homepage on the Internet] Drug Information, Tobacco. [Last accessed on 2012 Aug 20]. Available from: http://www.cesar.umd.edu/cesar/drugs/tobacco.asp .
- 3.Wallace RB. 15th ed. chapter 54. New York: McGraw-Hill; 2008. Maxy-Rosenau-Last-Public health and Preventive Medicine; p. 953. [Google Scholar]
- 4.Centers for Disease Control and Prevention, Smoking and Tobacco Use, Health Effects of Cigarette Smoking. 2011. [Last accessed on 2012 Aug 20]. Available from: http://www.cdc.gov/tobacco/data_statistics/fact_sheets/health_effects/effects_cig_smoking/
- 5.The National Institute on Drug Abuse (NIDA), NIDA InfoFacts: Cigarettes and Other Tobacco Products. [Last accessed on 2012 Aug 20]. updated 2010 October. Available from: http://www.drugabuse.gov/Infofacts/Tobacco.html .
- 6.Effects of smoking. [Last accessed on 2012 Aug 20]. Available from: http://www.Stopsmokingonlinetoday.com/quit/effects-of-smoking/
- 7.Types of Tobacco Products. [Last accessed on 2012 Aug 20]. Available from: http://www.ct.gov/dph/lib/dph/hems/tobacco/tobacco_products.pdf .
- 8.Saha SP, Bhalla DK, Whayne TF, Gairola CG. Cigarette smoke and adverse health effects: An overview of research trends and future needs. Int J Angiol. 2007;16:77–83. doi: 10.1055/s-0031-1278254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Naurath N, Jones JM. Smoking Rates around the World-How Do Americans Compare? [Last accessed on 2007 Aug 17]. Available from: http://www.gallup.com/poll/28432/smoking-rates-around-world-how-americans-compare.aspx .
- 10.Mowery PD, Farrelly MC, Haviland ML, Gable JM, Wells HE. Progression to established smoking among US youths. Am J Public Health. 2004;94:331–7. doi: 10.2105/ajph.94.2.331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Fotouhi A, Khabazkhoob M, Hashemi H, Mohammad K. The prevalence of cigarette smoking in residents of Tehran. Arch Iran Med. 2009;12:358–64. [PubMed] [Google Scholar]
- 12.Ramezankhani A, SarbandiZaboli F, Zarghi A, Masjedi MR, Heidari GR. Smoking habits of adolescent students in Tehran. Tanaffos. 2010;9:33–42. [Google Scholar]
- 13.Tamim H, Terro A, Kassem H, Ghazi A, Khamis TA, Hay MM, et al. Tobacco use by university students [abstract], Lebanon. Addiction. 2003;98:933–9. doi: 10.1046/j.1360-0443.2003.00413.x. [DOI] [PubMed] [Google Scholar]
- 14.Majidpour A, Hamidzadeh Arbaby Y, Abbasgholizadeh N, Salehy S. Prevalence and Causes of Tendency to Cigarette Smoking among Students in Ardabil University of Medical Sciences. J Ardabil Univ Med Sci Health Servi. 2005;5:266–70. [Google Scholar]
- 15.Ansari R, Khosravy A, Mokhtary M. Prevalence and causes of tendency to cigarette smoking among medical student. J Semnan Univ Med Sci. 2007;9:21–6. [Google Scholar]
- 16.Ghanizadeh A. Shiraz University students’ attitude towards drugs: An exploratory study. East Mediterr Health J. 2001;7:452–60. [PubMed] [Google Scholar]
- 17.Divsalar K, Nakhaei N. Prevalence and correlates of Cigarette Smoking among Students of Two Universities in Kerman, Iran. J Babol Univ Med Sci (JBUMS) 2008;10:78–83. [Google Scholar]
- 18.Nakhaee N, Divsalar K, Jadidi N. Religious involvement and cigarette smoking among Iranian university students [abstract] Int J Psychiatry Med. 2009;39:189–98. doi: 10.2190/PM.39.2.g. [DOI] [PubMed] [Google Scholar]
- 19.Chatterjee T, Haldar D, Mallik S, Sarkar GN, Das S, Lahiri SK. A study on habits of tobacco use among medical and non-medical students of Kolkata. Lung India. 2011;28:5–10. doi: 10.4103/0970-2113.76293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Metintaş S, Sariboyaci MA, Nuhoğlu S, Metintaş M, Kalyoncu C, Etiz S, et al. Smoking patterns of university students in Eskişehir, Turkey. Public Health. 1998;112:261–4. doi: 10.1038/sj.ph.1900470. [DOI] [PubMed] [Google Scholar]
- 21.Sugathan TN, Moody PM, Bustan MA, Elgerges NS. Age patterns of smoking initiation among Kuwait university male students. Soc Sci Med. 1998;47:1855–8. doi: 10.1016/s0277-9536(98)00204-4. [DOI] [PubMed] [Google Scholar]
- 22.Dar-Odeh NS, Bakri FG, Al-Omiri MK, Al-Mashni HM, Eimar HA, Khraisat AS, et al. Narghile (water pipe) smoking among university students in Jordan: Prevalence, pattern and beliefs. Harm Reduct J. 2010;24(7):10. doi: 10.1186/1477-7517-7-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Torres AR, Ruiz T, Müller SS, Lima MC. Quality of life, physical and mental health of physicians: A self-evaluation by graduates from the Botucatu Medical School-UNESP. Rev Bras Epidemiol. 2011;14:264–75. doi: 10.1590/s1415-790x2011000200008. [DOI] [PubMed] [Google Scholar]
- 24.Rozi S, Butt ZA, Akhtar S. Correlates of cigarette smoking among male college students in Karachi, Pakistan. BMC Public Health. 2007;7:312. doi: 10.1186/1471-2458-7-312. [DOI] [PMC free article] [PubMed] [Google Scholar]