

Abstract
Herlyn-Werner-Wunderlich syndrome (HWWS), characterized by uterus didelphys, obstructed hemivagina, and ipsilateral renal agenesis, is an uncommon combined Mullerian and mesonephric duct anomaly, and its presentation in adulthood is even rarer. We report here a 22-year-old female presenting with primary infertility where magnetic resonance imaging (MRI) suggested the diagnosis of HWWS with endometriosis. In a patient of infertility with endometriosis and unilateral renal agenesis, diagnosis of HWWS should be suspected and MRI is the investigation of choice for such anomalies.
Keywords: Endometriosis, Herlyn-Werner-Wunderlich syndrome, infertility, magnetic resonance imaging, mullerian anomaly
Introduction
Herlyn–Werner–Wunderlich syndrome (HWWS) is often a misdiagnosed entity and high index of suspicion is required in patients with Mullerian and mesonephric duct anomalies. It usually presents at puberty with pelvic pain, but rarely can present in neonates or in adulthood in the form of pyometra, ischiorectal swelling, urinary obstruction, and primary infertility.[1,2,3,4] Since this condition can be treated by vaginal septum excision, and delay in diagnosis may worsen the associated endometriosis,[5] early diagnosis is beneficial. Magnetic resonance imaging (MRI) is the modality of choice for the diagnosis of HWWS and other such anomalies because of better anatomic delineation of pelvic structures and higher sensitivity for blood products.
Case Report
A 22-year-old female, cohabiting with her husband for last 3 years, was evaluated for primary infertility in a private hospital. She attained menarche at the age of 13 years and had a normal menstrual history with no complaints of excessive dysmenorrhoea, dyspareunia, or vaginal discharge. Routine hematological laboratory tests were normal. An abdominal USG and computed tomography (CT) were performed, which revealed absent left kidney, a bicornuate uterus, bilateral cystic adnexal lesions, and left hydrosalpinx. She was taken up for laparotomy and underwent left ovarian cystectomy and adhesiolysis. Histopathology from the left adnexal lesion showed endometriotic cysts and aspirated pelvic fluid showed hemosiderin-laden macrophages. Postoperatively, she was kept on medical management for endometriosis.
She did not resume her menses for 3 months post-surgery and urine pregnancy test was negative, following which she was referred to our institute for further evaluation. MRI examination of the pelvis was performed to assess the current status of endometriosis. MRI revealed two separate uterine cavities, cervices, and vaginas, suggestive of uterus didelphys [Figures 1-3]. The right uterine cavity, cervix, and vagina were normal. The left uterine cavity and cervical canal were dilated and filled with fluid which was hyperintense on both T1W and T2W MRI [Figures 1 and 2] with few T2-hypointense areas [Figure 4] suggesting blood products. Left hemivagina was dilated [Figures 1, 2, and 4] with blood products within, implicating the presence of an obstructing left vaginal septum. Multiloculated left adnexal cystic lesions with blood products were seen suggestive of endometriotic cysts [Figure 5]. In addition, a tubular structure was noted in left adnexal location extending laterally from left uterine cornu with hemorrhagic fluid within, indicative of left hematosalpinx. Right ovary was normal. In addition, there was absent left kidney [Figure 6] with loculated hemorrhagic fluid collections in bilateral paracolic gutters, suggestive of peritoneal endometriosis [Figure 7].
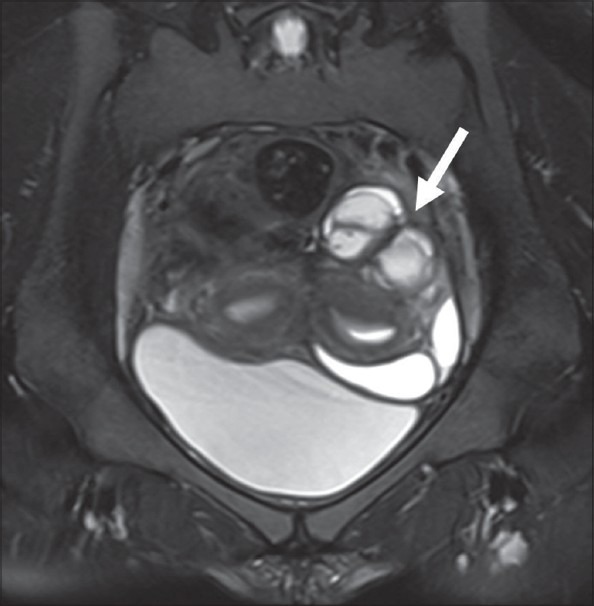
Figure 1.
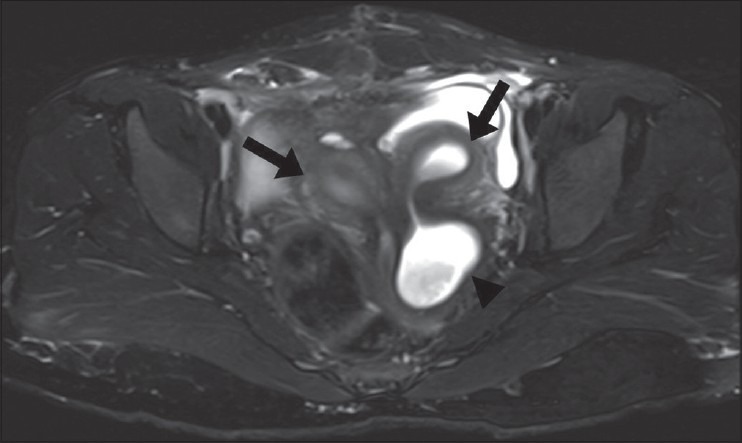
Axial T2W MRI shows two separate uterine cavities (black arrows) with two separate cervices and dilatation of left hemivagina (arrowhead)
Figure 3.
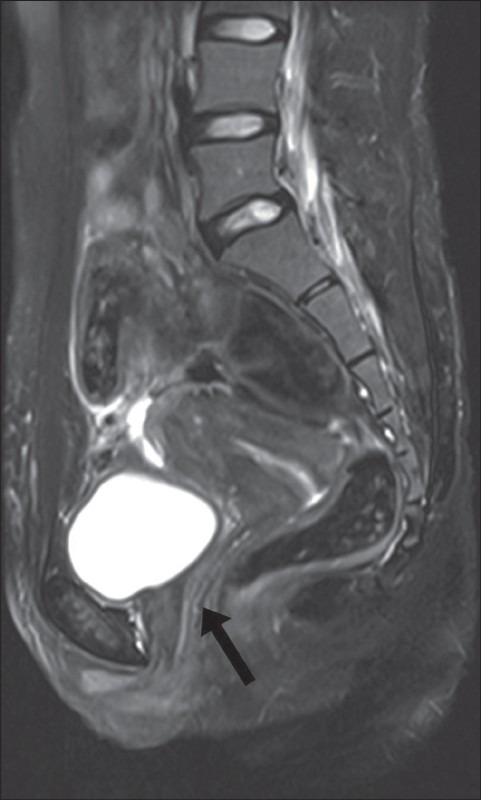
Sagittal T2W MRI shows right uterine cavity with normal cervix and vagina (black arrow)
Figure 2.
Axial fat-suppressed T1W MRI shows hyperintense contents of dilated left hemivagina (arrow) and uterine cavity, suggestive of blood products
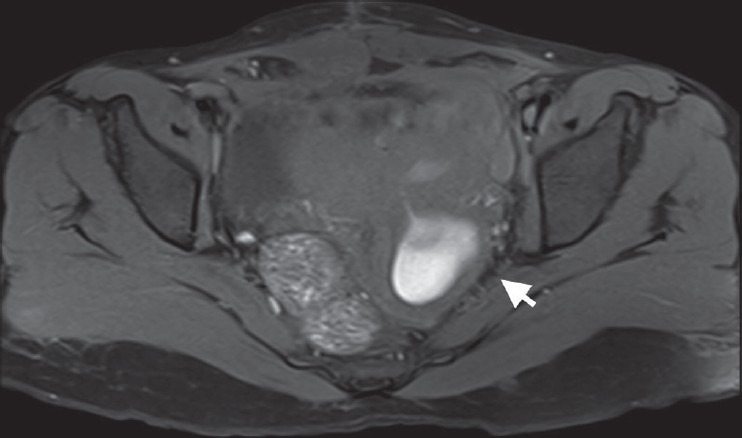
Figure 4.
Sagittal T2W MRI shows left uterine cavity (thin arrow) with dilated hemivagina (thick arrow) showing hypointense signal within a background of hyperintensity (T2 shading), suggestive of blood products within (hematometra)
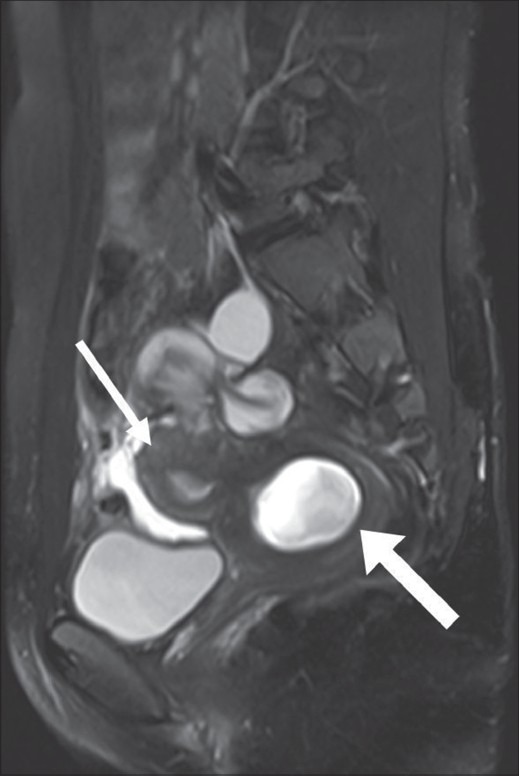
Figure 5.
Coronal T2W MRI shows multiloculated cystic lesion in left adnexa with T2 shading suggestive of blood products with endometriotic cysts
Figure 6.
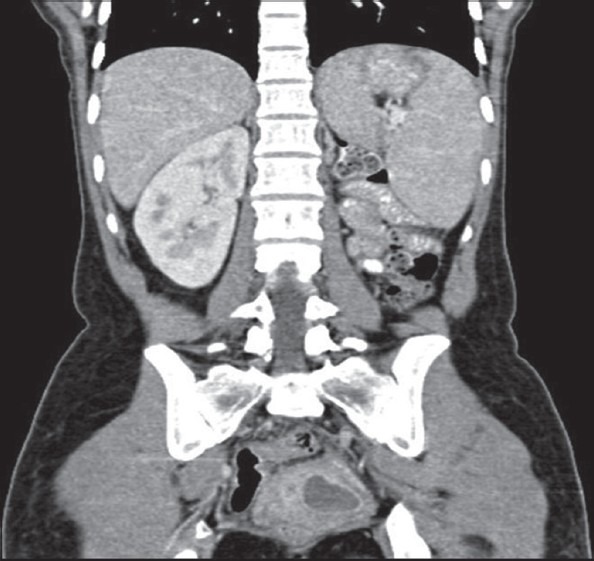
Coronal contrast-enhanced CT image reveals absent left kidney
Figure 7.
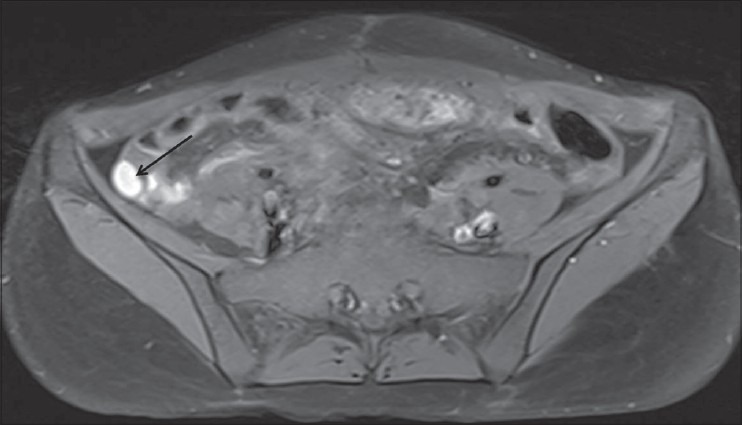
Axial fat-supressed T1W MRI shows multilocular T1 hyperintense fluid collections in right paracolic gutter (arrow) consistent with peritoneal endometriosis
Hence, a diagnosis of uterus didelphys with left hematometra, hematosalpinx, hematocolpos, and left hemivaginal obstruction with adnexal and peritoneal endometriosis was made. Considering that she also had absent left kidney, a final diagnosis of HWWS or obstructed hemivagina ipsilateral renal anomaly (OHVIRA) syndrome was made. Since the patient had already undergone recent laparotomy, no further surgery was immediately performed. She has been kept on short-term conservative management with oral contraceptives to suppress menstruation and laparoscopic vaginal septal excision has been planned after 3 months.
Discussion
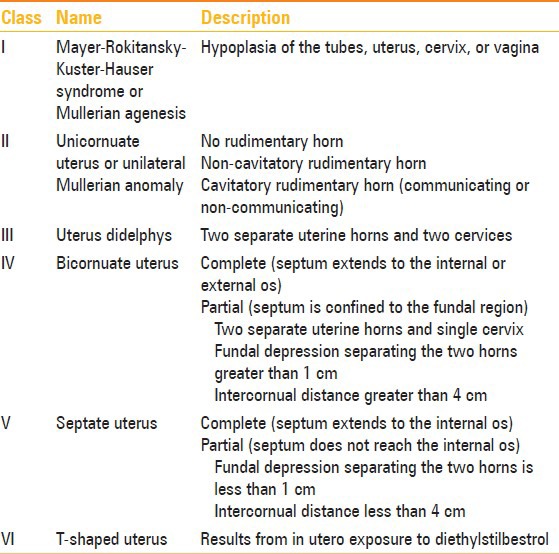
The most frequently used system for classification of Mullerian duct anomalies (MDAs) was proposed by Buttram and Gibbons, which classifies them into six categories[6] [Table 1].
Table 1.
Mullerian duct anomalies classification
HWWS is a combination of Type III Mullerian anomaly with mesonephric duct anomaly with vaginal septum. The classic renal manifestation of OHVIRA syndrome is ipsilateral renal agenesis, but reports of duplicated kidneys, dysplastic kidneys,[7] rectovesical bands,[8] or crossed fused ectopia[9] have also been described. Uterus didelphys with obstructed hemivagina is due to lateral non-fusion of the Mullerian ducts with asymmetric obstruction, and it is almost always associated with renal agenesis ipsilateral to the side of obstruction.[7] An important point to note in patients with HWWS is that renal agenesis is located ipsilateral to the dilated uterine cavity. On the other hand, in case of unicornuate uteri, the renal anomalies are ipsilateral to the rudimentary or absent uterine horn.[10] Embryopathogenesis of HWWS can be temporally located around 8 weeks of gestation, simultaneously affecting both Mullerian and metanephric ducts.[11]
Haddad et al. studied the associations of a blind hemivagina in 42 patients and found that it was associated with renal agenesis in all but one patient. In addition, blind hemivagina with ipsilateral agenesis was generally associated with uterus didelphys; however, rare cases of septate uterus were also found.[12]
Patients of endometriosis must be evaluated for any obstructive Mullerian lesion,[13] and presence of concomitant unilateral renal agenesis should indicate a suspicion for HWWS. Patients of HWWS usually have normal menstruation and may or may not complain of dysmenorrhoea, explaining the delay in diagnosis in adults.[14] Endometriosis is a frequent complication of this syndrome. This is because of obstructed outflow to part of the menstrual blood, which collects in obstructed Mullerian derivatives, leading to hematometra, hematosalpinx, and peritoneal endometriosis.
When suspecting a genitourinary anomaly, an initial screening ultrasound should be followed by MRI rather than CT, since the later involves radiation exposure and many questions remain unanswered because of its limited soft-tissue resolution. Considering the vast differential in uterovaginal anomalies, precise anatomical delineation of the uterus, tubes, cervix, and vagina is essential. Status of these reproductive organs and extent of endometriosis, pelvic inflammation, and adhesions can be well evaluated with MRI.[9] Laparoscopy remains the gold standard diagnostic modality with the additional advantages of therapeutic drainage of hematocolpos/hematometra, vaginal septectomy, and marsupialization.[15,16]
Laparoscopic vaginal septum excision is the treatment of choice for HWWS. A successful pregnancy is achieved eventually in 87% patients, while 23% have the risk of abortions.[14]
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Wu TH, Wu TT, Ng YY, Ng SC, Su PH, Chen JY, et al. Herlyn-Werner-Wunderlich Syndrome consisting of uterine didelphys, obstructed hemivagina and ipsilateral renal agenesis in a newborn. Pediatr Neonatol. 2012;53:68–71. doi: 10.1016/j.pedneo.2011.11.014. [DOI] [PubMed] [Google Scholar]
- 2.Jeong JH, Kim YJ, Chang CH, Choi HI. A case of Herlyn-Werner-Wunderlich syndrome with recurrent hematopyometra. J Womens’ Med. 2009;2:77–9. [Google Scholar]
- 3.Asha B, Manila K. An unusual presentation of uterus didelphys with obstructed hemivagina with ipsilateral renal agenesis. Fertil Streril. 2008;849:e9–10. doi: 10.1016/j.fertnstert.2007.08.003. [DOI] [PubMed] [Google Scholar]
- 4.Mandava A, Prabhakar RR, Smitha S. OHVIRA Syndrome (obstructed hemivagina and ipsilateral renal anomaly) with Uterus Didelphys, an Unusual Presentation. J Pediatr Adolesc Gynecol. 2012;25:e23–5. doi: 10.1016/j.jpag.2011.11.004. [DOI] [PubMed] [Google Scholar]
- 5.Adair L, II, Georgiades M, Osborne R, Ng T. Uterus didelphys with unilateral distal vaginal agenesis and ipsilateral renal agenesis: Common presentation of an unusual variation. J Radiol Case Rep. 2011;5:1–8. doi: 10.3941/jrcr.v5i1.572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Buttram VC, Jr, Gibbons WE. Mullerian anomalies: A proposed classification (an analysis of 144 cases) Fertil Steril. 1979;32:40–6. doi: 10.1016/s0015-0282(16)44114-2. [DOI] [PubMed] [Google Scholar]
- 7.Prada Arias M, Muguerza Vellibre R, Montero Sánchez M, Vázquez Castelo JL, Arias González M, Rodríguez Costa A. Uterus didelphys with obstructed hemivagina and multicystic dysplastic kidney. Eur J Pediatr Surg. 2005;15:441–5. doi: 10.1055/s-2005-872926. [DOI] [PubMed] [Google Scholar]
- 8.Heinonen PK. Clinical implications of the didelphic uterus: Long-term follow-up of 49 cases. Eur J Obstet Gynecol Reprod Biol. 2000;91:183–90. doi: 10.1016/s0301-2115(99)00259-6. [DOI] [PubMed] [Google Scholar]
- 9.Tanaka YO, Kurosaki Y, Kobayashi T, Eguchi N, Mori K, Satoh Y, et al. Uterus didelphys associated with obstructed hemivagina and ipsilateral renal agenesis: MR findings in seven cases. Abdom Imaging. 1998;23:437–41. doi: 10.1007/s002619900375. [DOI] [PubMed] [Google Scholar]
- 10.Brody JM, Koelliker SL, Frishman GN. Unicornuate uterus: Imaging appearance, associated anomalies, and clinical implications. AJR Am J Roentgenol. 1998;171:1341–7. doi: 10.2214/ajr.171.5.9798876. [DOI] [PubMed] [Google Scholar]
- 11.Singh M, Geareart JP, Rock JA. Double urethra, double bladder, left renal agenesis, persistent hymen, double vagina and uterus didelphys. Adolesc Pediatr Gynecol. 1993;6:99. [Google Scholar]
- 12.Haddad B, Barranger E, Paniel BJ. Blind hemivagina: Long-term follow-up and reproductive performance in 42 cases. Hum Reprod. 1999;14:1962–4. doi: 10.1093/humrep/14.8.1962. [DOI] [PubMed] [Google Scholar]
- 13.Del Vescovo R, Battisti S, Di Paola V, Piccolo CL, Cazzato RL, Sansoni I, et al. Herlyn-werner-wunderlich syndrome: MRI findings, radiological guide (two cases and literature review), and differential diagnosis. BMC Med Imaging. 2012;12:4. doi: 10.1186/1471-2342-12-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Candiani GB, Fedele L, Candiani M. Double uterus, blind hemivagina, and ipsilateral renal agenesis: 36 cases and long term follow-up. Obstet Gynecol. 1997;90:26–32. doi: 10.1016/S0029-7844(97)83836-7. [DOI] [PubMed] [Google Scholar]
- 15.Gholoum S, Puligandla PS, Hui T, Su W, Quiros E, Laberge JM. Management and outcome of patients with combined vaginal septum, bifid uterus and ipsilateral renal agenesis (Herlin-Werner-Wunderlich syndrome. J Pediatr Surg. 2006;41:987–92. doi: 10.1016/j.jpedsurg.2006.01.021. [DOI] [PubMed] [Google Scholar]
- 16.Park NH, Park HJ, Park CS, Park SI. Herlyn-Werner-Wunderlich Syndrome with unilateral hemivaginal obstruction, ipsilateral renal agenesis and contralateral renal thin GBM disease: A case report with radiological follow up. J Korean Soc Radiol. 2010;62:383–8. [Google Scholar]