

Abstract
Sternocostoclavicular hyperostosis is a chronic inflammatory disorder affecting the sternoclavicular joint and upper ribs. There is a strong association with seronegative spondyloarthropathy in which bilateral involvement is common. Ultrasonography and Color Doppler findings of this entity have not been described previously, to the best of our knowledge. We describe the findings in a patient of ankylosing spondylitis who was referred for unilateral sternoclavicular joint swelling.
Keywords: Ankylosing spondylitis, color doppler ultrasonography, sternocostoclavicular hyperostosis
Introduction
Sternocostoclavicular hyperostosis (SCCH) is a rare disease.[1] Bony overgrowth involving the medial end of the clavicle and sternum along with periarticular soft-tissue calcification are typical features of this disease. Unilateral involvement is uncommon.[2] The first rib may also be involved in the disease process. This condition is strongly associated with palmoplantar pustulosis and seronegative spondyloarthropathy[2] Computed tomography (CT) scans of sternoclavicular joint (SCJ) are commonly used for the diagnosis of this disorder.
Case Report
A 42-year-old male attended our Rheumatology outpatient clinic with a history of swelling and mild pain of right SCJ for about eight months. There was no history of trauma or fever. The patient had been diagnosed to have ankylosing spondylitis since ten years with predominantly axial involvement. Clinical examination revealed a warm, hard and tender swelling over right SCJ. No skin lesions such as acne or pustulosis palmaris et plantaris were observed. Ankylosing spondylitis disease activity was fairly controlled (Bath ankylosing spondylitis disease activity index: 2.5.[3] Radiograph of sternoclavicular joint did not detect any abnormality. Ultrasonography (USG) and doppler examination revealed calcifications around the joint with periarticular hypervascularity [Figures 1 and 2]. Doppler spectral analysis revealed low-resistance flow [Figure 3]. All the features were compared with normal left SCJ. CT scan showed calcifications around the right sternoclavicular joint and adjacent right first rib [Figure 4]. A diagnosis of right SCCH was made from clinical and imaging features. The patient was treated with non-steroidal anti-inflammatory agent and advised rest, physiotherapy and follow-up.
Figure 1.
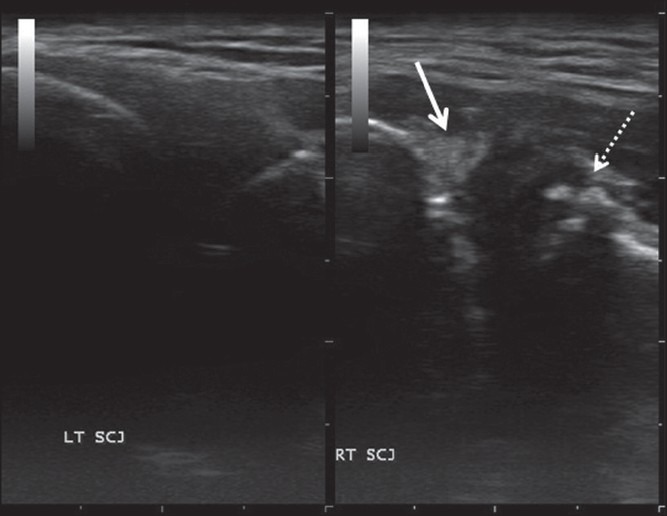
USG of the right sternoclavicular joint (RT SCJ) showing calcification around the medial end of the clavicle (solidarrow) and sternum (dottedarrow). Normal left SCJ (LT SCJ) for comparison
Figure 2.
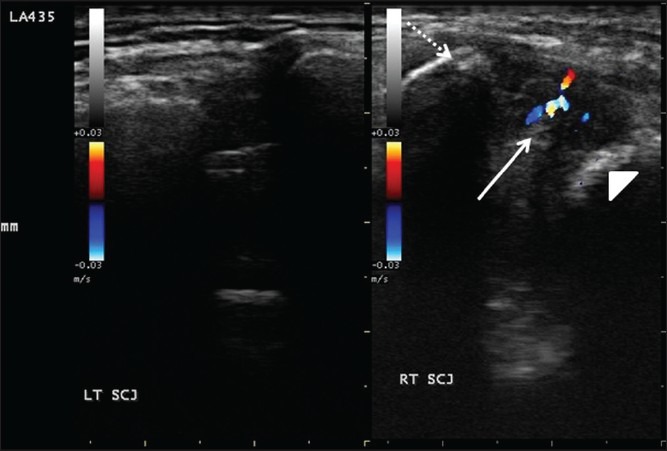
Color flow imaging of the right sternoclavicular joint (RT SCJ) showing periarticular hypervascularity (solidarrow, dottedarrow-medial end of clavicle. arrowhead-sternum). The normal left side (LT SCJ) for comparison
Figure 3.
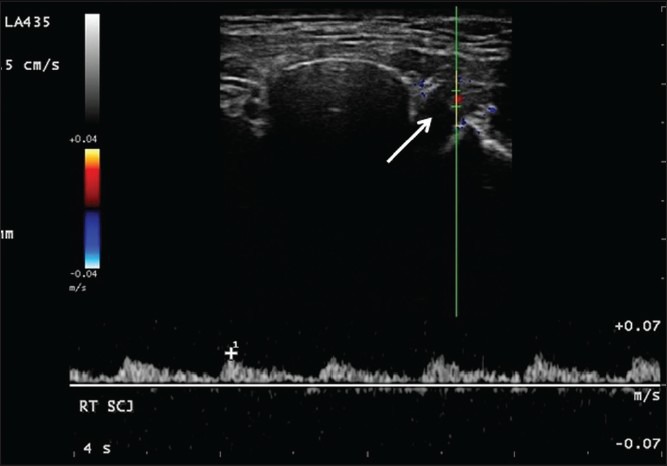
Duplex study of right SCJ vessels (arrow) showing low-velocity flow with prolonged antegrade diastolic phase
Figure 4.
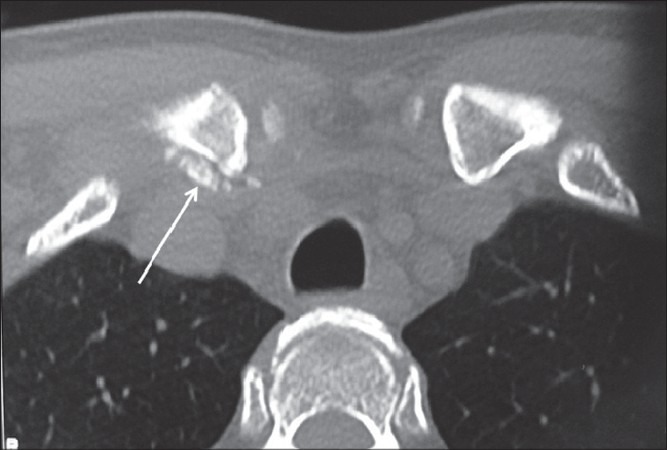
Axial CT scans of the sternoclavicular joints showing soft-tissue calcification around the medial end of the right clavicle (arrow)
Discussion
SCCH is a chronic inflammatory disease which commonly presents with pain, swelling and redness of the affected joint.[4] Between 10-30% cases are associated with pustulosis palmaris et plantaris. Seronegative spondyloarthropathy is another important association.[2] The disease characteristically starts as a non-specific inflammation of the sternoclavicular ligament and also involves periarticular soft tissues. The chronic inflammatory process ultimately leads to bony hyperostosis and localized soft-tissue calcification which may result in fusion of SCJ in longstanding disease.[5] Bilateral involvement is common.[6]
Differential diagnosis of unilateral SCJ arthritis includes infective and inflammatory pathologies like sternal osteomyelitis, septic arthritis, rheumatoid arthritis and osteoarthritis of SCJ.
CT scan detects the characteristic changes of SCCH earlier than conventional radiography and is therefore the preferred modality for diagnosis of SCCH.[7] Findings range from localized disease with mild ossification of costoclavicular ligament to the formation of a bone mass between the clavicle, sternum, and first or upper ribs. Based on these features, Sonozaki et al., categorized the radiological findings into three groups.[8] This was later modified by various other authors to include those without definite ossification or evidence of multiple rib or extrasternal involvement.[5,9] Radiography of the sternoclavicular joint and scintigraphy are other modalities used in the diagnosis of SCCH. Scintigraphy shows increased radiotracer uptake in characteristic regions and is helpful in the diagnosis of SCCH, especially when radiographic changes are subtle.[10,11]
The utility of USG in pathologies affecting superficial joints is now widely accepted. Power Doppler USG of hand joints has good sensitivity and accuracy in detecting active synovitis in rheumatoid arthritis.[12] In rheumatoid arthritis of SCJ, USG shows widening of joint space and osseous irregularity. In addition, synovial vascularity can be assessed by Color Doppler study giving some information on activity of the disease. Infective conditions of SCJ like septic arthritis and osteomyelitis demonstrate joint effusion, irregularity of the bony margins and soft tissue thickening on USG.
There is a paucity of data regarding the role of USG in the assessment of SCJ pathology; neither is there any case report with USG description of SCCH.
USG is less expensive than CT and widely available. The capability to perform dynamic real-time imaging is a unique advantage of USG. CT scan is very useful for detection of articular and peri-articular changes seen in SCCH. Abnormalities of the bony cortex, articular surface irregularities and soft-tissue calcifications are readily detected by CT scan but it is relatively expensive.
In our case, the characteristic USG features enabled us to suggest SCCH as a diagnostic probability. Further, the application of color flow imaging helped us to study the ongoing inflammatory process within the affected joint and thereby detection of SCCH at an earlier stage. This is very important from the prognostic viewpoint as early intervention may prevent SCJ fusion.
Conclusion
USG and Color Doppler evaluation is useful in the diagnosis of SCCH as well as determining the disease activity. This cost-effective modality must be generously used in imaging of sternoclavicular joint pathologies.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Van der Kloot WA, Chotkan SA, Kaptein AA, Hamdy NA. Diagnostic delay in sternocostoclavicular hyperostosis: Impact on various aspects of quality of life. Arthritis Care Res (Hoboken) 2010;62:251–7. doi: 10.1002/acr.20075. [DOI] [PubMed] [Google Scholar]
- 2.Hiramuro-Shoji F, Wirth MA, Rockwood CA., Jr Atraumatic conditions of the sternoclavicular joint. J Shoulder Elbow Surg. 2003;12:79–88. doi: 10.1067/mse.2003.128566. [DOI] [PubMed] [Google Scholar]
- 3.Sieper J. Management of ankylosing spondylitis. In: Hochberg MC, Silman AJ, Smolen JS, Weinblatt ME, Weisman MH, editors. Rheumatology. Philadelphia: Elsevier; 2011. pp. 1157–77. [Google Scholar]
- 4.Carroll MB. Sternocostoclavicular hyperostosis: A review. Ther Adv Musculoskelet Dis. 2011;3:101–10. doi: 10.1177/1759720X11398333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Fritz P, Baldauf G, Wilke HJ, Reitter I. Sternocostoclavicular hyperostosis: Its progression and radiological features. A study of 12 cases. Ann Rheum Dis. 1992;51:658–64. doi: 10.1136/ard.51.5.658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sartoris DJ, Schreiman JS, Kerr R, Resnik CS, Resnick D. Sternocostoclavicular hyperostosis: A review and report of 11 cases. Radiology. 1986;158:125–8. doi: 10.1148/radiology.158.1.3940368. [DOI] [PubMed] [Google Scholar]
- 7.Edwin E, Spencer, Michael A, Charles A, Rockwood . Disorders of the sternoclavicular joint: Pathophysiology, Diagnosis, and Management. In: Iannotti JP, Williams GR, editors. Disorders of the shoulder: Diagnosis and Management. Philadelphia: Lippincott Williams and Wilkins; 2007. pp. 1007–53. [Google Scholar]
- 8.Sonozaki H, Azuma A, Okai K, Nakamura K, Fukuoka S, Tateishi A, et al. Clinical features of 22 cases with inter-sterno-costo-clavicular ossification: A new rheumatic syndrome. Arch Orthop Trauma Surg. 1979;95:13–22. doi: 10.1007/BF00379164. [DOI] [PubMed] [Google Scholar]
- 9.Chigira M, Shimizu T. Computed tomographic appearances of sternocostoclavicular hyperostosis. Skeletal Radiol. 1989;18:347–52. doi: 10.1007/BF00361423. [DOI] [PubMed] [Google Scholar]
- 10.Kim BY, Karak P, Bybel B, Freedman GS, Neumann DR. Sternocostoclavicular hyperostosis: Scintigraphic evaluation. Clin Nucl Med. 2001;26:452–4. doi: 10.1097/00003072-200105000-00017. [DOI] [PubMed] [Google Scholar]
- 11.Nungu S, Olerud C, Rehnberg L. Sternocostoclavicular hyperostosis. Presentation and long-term follow-up of three cases. Ups J Med Sci. 1992;97:177–82. doi: 10.3109/03009739209179294. [DOI] [PubMed] [Google Scholar]
- 12.Fukuba E, Yoshizako T, Kitagaki H, Murakawa Y, Kondo M, Uchida N. Power Doppler ultrasonography for assessment of rheumatoid synovitis: Comparison with dynamic magnetic resonance imaging. Clin Imaging. 2013;37:134–7. doi: 10.1016/j.clinimag.2012.02.008. [DOI] [PubMed] [Google Scholar]