

Abstract
Background
The authors evaluated the efficacy and tolerability of 10 percent and 20 percent benzocaine gels compared with those of a vehicle (placebo) gel for the temporary relief of toothache pain. They also assessed the compliance with the label dose administration directions on the part of participants with toothache pain.
Methods
Under double-masked conditions, 576 participants self-applied study gel to an open tooth cavity and surrounding oral tissues. Participants evaluated their pain intensity and pain relief for 120 minutes. The authors determined the amount of gel the participants applied.
Results
The responders’ rates (the primary efficacy parameter), defined as the percentage of participants who had an improvement in pain intensity as exhibited by a pain score reduction of at least one unit on the dental pain scale from baseline for two consecutive assessments any time between the five- and 20-minute points, were 87.3 percent, 80.7 percent and 70.4 percent, respectively, for 20 percent benzocaine gel, 10 percent benzocaine gel and vehicle gel. Both benzocaine gels were significantly (P ≤ .05) better than vehicle gel; the 20 percent benzocaine gel also was significantly (P ≤ .05) better than the 10 percent benzocaine gel. The mean amount of gel applied was 235.6 milligrams, with 88.2 percent of participants applying 400 mg or less.
Conclusions
Both 10 percent and 20 percent benzocaine gels were more efficacious than the vehicle gel, and the 20 percent benzocaine gel was more efficacious than the 10 percent benzocaine gel. All treatments were well tolerated by participants.
Practical Implications
Patients can use 10 percent and 20 percent benzocaine gels to temporarily treat toothache pain safely.
Keywords: Benzocaine, toothache, pain, topical anesthetic, methemoglobinemia, double stopwatch
Topical benzocaine is marketed in 10 percent and 20 percent formulations (regular [10 percent] and maximum [20 percent] strength Orajel [Church & Dwight, Princeton, N.J.] and Anbesol [Pfizer Consumer Healthcare. Madison, N.J.]) for the temporary relief of toothache pain and has been used widely since 1903.1 The U.S. Food and Drug Administration (FDA) assigned this product category I monograph status (generally recognized as safe and effective) as an external anesthetic or analgesic for the temporary relief of pain due to minor irritation or injury of the mouth and gingivae, minor dental procedures, dentures, orthodontic appliances, canker sores, teething, sore mouth and sore throat.2 However, the FDA concluded that the available data were not adequate to establish the effectiveness of benzocaine for the temporary relief of toothache pain and assigned category III status (judged to be safe but efficacy data not confirmative) in the over-the-counter (OTC) monograph for this indication, noting that the FDA would consider reclassifying benzocaine as category I if additional data were received from well-controlled studies.2 We conducted a study with the intention of meeting this requirement.
Investigators in several small vehicle- (placebo-) controlled studies published results supporting the effectiveness of 7.5 to 20.0 percent benzocaine gels in relieving toothache pain.3-5 In these studies, the benzocaine and polyethylene glycol vehicle gels were applied by the investigators3,4 or the study participants5 to both the open tooth cavity and the surrounding soft tissue; significant differences in favor of benzocaine were achieved. In another study, investigators placed a mucoadhesive patch containing 12 milligrams of benzocaine or a vehicle apical to the mucogingival junction of the symptomatic tooth, and a significantly greater percentage (P < .05) of participants in the benzocaine group reported meaningful pain relief (PR) than did participants in the vehicle group by the 30-minute point.6 The results of these studies show that the ability of benzocaine to anesthetize the surrounding soft tissue may contribute to its effectiveness in temporarily relieving toothache pain. Label dose administration directions for one 20 percent benzocaine gel product stated that it should be applied to both the symptomatic open tooth cavity and around the gingivae surrounding the teeth.7 We designed our study to incorporate application to both the tooth and the soft tissue.
Despite benzocaine’s long history of safe use, it has been associated in rare instances with methemoglobinemia, a condition in which the oxygen-carrying capacity of the blood is reduced (ferric state). Although most of the cases of methemoglobinemia in the literature involve benzocaine spray application in a hospital environment for diagnostic procedures such as intubation, endoscopy, bronchoscopy and transesophageal echocardiography,8-44 case reports of methemoglobinemia associated with OTC use of benzocaine have been published.11,45-55 Only two of these cases involved benzocaine self-application for toothache, and both of these cases involved significant overdoses.54,55
In 2011, the FDA issued a safety communication noting the potential for OTC benzocaine products to cause methemoglobinemia on rare occasions.56 Most reports of methemoglobinemia involved children. Thus, although cases of methemoglobinemia involving self-application by adult patients with toothache are rare and typically involve significant overdoses of the drug, it is important to evaluate patients’ compliance with label dose administration directions in patients as young as 12 years (12 years is the youngest age recommended for benzocaine self-application in patients with an acute toothache7).
The FDA has determined that the existing body of evidence supporting the use of topical benzocaine for the temporary relief of toothache pain is lacking.2 For benzocaine to gain category I status for the treatment of toothache pain under the OTC monograph system, additional data are needed. We conducted a study to evaluate the efficacy and tolerability of 10 percent and 20 percent benzocaine gels compared with those of a vehicle gel in participants with toothache pain, as well as to assess the compliance of these participants with the benzocaine gel dose administration directions in a newly proposed product label developed by the manufacturers of Orajel and Anbesol.
METHODS
The institutional review boards at the participating research centers (University of Pennsylvania, Philadelphia; The State University of New York at Buffalo; University of Pittsburgh; Nationwide Children’s Hospital, Columbus, Ohio; The Ohio State University, Columbus; University of Detroit Mercy; New York University, New York City; Tufts University, Boston; and University of Maryland, Baltimore) approved the protocol, informed consent forms and assent forms (for minors), and we listed the trial in ClinicalTrials. gov under the identifier NCT00474175. Male and female patients aged at least 12 years from all ethnic backgrounds were eligible to participate in the study. In the case of minors (those younger than 18 years), both a parental informed consent form and an adolescent assent form had to be read and signed by both the parent or guardian and the child. Study participants had to arrive at the research site with toothache pain of at least a moderate intensity on one permanent tooth with an open tooth cavity to be included in the study.
Participants rated their pain on an ordinal dental pain scale (DPS) on which 0 indicates no pain, 1 indicates slight pain, 2 indicates moderate pain, and 3 indicates severe pain. These results were corroborated by a score of at least 50 millimeters on a 100-mm visual analog scale on which 0 mm indicates no pain and 100 mm indicates the worst possible pain. We excluded patients from the study if they had pain from multiple hard-tissue or soft-tissue sites, had a periodontal abscess, did not have an open tooth cavity, reported having any allergies or contraindications to benzocaine or other local anesthetics, or had taken any short-acting systemic or topical analgesic within 120 minutes before the study visit or any long-acting systemic analgesic agent within 240 minutes before the study visit.
We randomly assigned those who qualified for the study to self-apply a single dose of the polyethylene glycol vehicle gel, 10 percent benzocaine gel or 20 percent benzocaine gel in a ratio of 1:2:2 stratified according to participants’ baseline pain levels (moderate or severe). To assess compliance with dose administration directions, we gave participants the product label showing dose administration directions and a picture of how much gel to apply to their painful tooth and surrounding gingival tissue (Figure 1). We weighed the contents of each coded 7-milliliter study gel tube by using a digital balance immediately before and after participants self-applied the study gel with their fingers. Participants rated their pain intensity and PR levels by using the DPS and a five-level ordinal dental pain relief scale on which 0 indicated no relief, 1 indicated a little relief, 2 indicated some relief, 3 indicated a lot of relief, and 4 indicated complete relief. They rated their pain intensity and PR levels at five-minute intervals from zero to 30 minutes and at 10- minute intervals from 30 to 120 minutes after they applied the study gel.5
Figure 1.
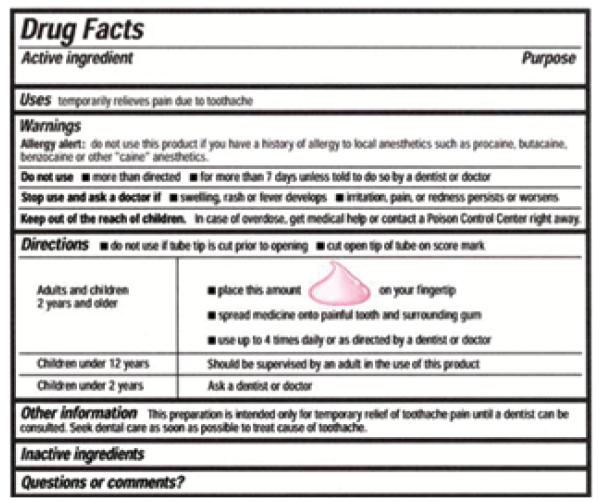
Label showing dose administration directions presented to study participants.
We recorded onset time of first perceptible relief and meaningful relief by asking the participants to press the buttons on two stopwatches when and if they experienced either event. The study coordinator activated both stopwatches at the time participants applied the study gel, and then he or she covered the stopwatch displays so that the participants could not see the elapsed time. We instructed the participants to “stop the first stopwatch when you first begin to feel any pain-relieving effect what-so-ever of the drug” and to “stop this second stopwatch when you have meaningful relief, that is, when the relief from the pain is meaningful to you,” as in previous postsurgical dental pain studies.57-59
Participants completed a five-level ordinal global satisfaction assessment scale used frequently in postsurgical dental pain studies58,59 at the conclusion of the 120-minute evaluation period or at the time they dropped out of the study owing to inadequate PR. (We encouraged participants with inadequate PR to wait at least 10 minutes before dropping out.) We asked participants, “How would you rate this medication for temporary relief of toothache pain?” Their choices were poor, fair, good, very good or excellent, and we assigned numeric values to each categorical response ranging from 0 for poor to 4 for excellent. We offered ibuprofen or acetaminophen to participants who requested a rescue analgesic. We encouraged these participants to remain in the research suite for the full 120 minutes.
We recorded the participants’ blood pressure and heart rates before they applied the study gel and again at 60 and 120 minutes after application. We recorded all adverse events (AEs) when they occurred, as well as the time the participant dropped out of the study during the 120-minute evaluation period if he or she dropped out. At the end of the evaluation period, we asked any participant who used 1 gram or more of the study gel (100 mg and 200 mg of 10 percent and 20 percent benzocaine, respectively) what the possible reason was for overapplying the gel. We referred all study participants for definitive dental care (endodontic therapy or extraction) at the end of the study.
Statistical analyses
The primary efficacy parameter was the percentage of responders, defined as a participant who had an improvement in pain intensity as exhibited by a pain score reduction of at least one unit on the DPS from baseline for two consecutive assessments any time between the five- and 20-minute points. We considered an observed increase of 10 percentage points for each of the benzocaine gels compared with the vehicle gel to be a clinically meaningful difference. We considered the dose response to be established if we observed an increase of five percentage points for the 20 percent benzocaine group compared with the 10 percent benzocaine group.
For power analysis, we assumed a 50 percent response rate in the benzocaine groups and a 30 percent response rate in the vehicle group, and we expected sample sizes of 200 per benzocaine group and 100 in the vehicle group to provide at least 90 percent power. We used two-sided statistical tests for all analyses. We controlled the type I error rate at 5 percent for efficacy analyses by testing 20 percent benzocaine gel against the vehicle gel first, followed by testing 10 percent benzocaine gel against the vehicle if the results of the first test were significant.
We used the Mantel-Haenszel test to analyze participants’ baseline DPS score, sex, race and age distribution. We analyzed the percentages of participants classified as responders in each group by using the Cochran-Mantel-Haenszel (CMH) test, controlling for site and baseline DPS score.
For the secondary efficacy parameters, we used the Kaplan-Meier method to estimate the distribution of the time elapsed before onset of confirmed first perceptible relief (time to pressing the button on the first stopwatch, provided that the participant also indicated meaningful relief by pressing the button on the second stopwatch59) and meaningful relief, duration of effect and time elapsed before dropping out owing to lack of efficacy for each treatment group. We used the Cox proportional hazards regression model, adjusting for site and baseline DPS score, to compare the treatment groups. We calculated pain intensity difference (PID) scores at each time point by subtracting each reported pain intensity score from the pain intensity score reported at baseline. We summed PR and PID scores at each time point to derive PR combined with PID (PRID) scores, and we plotted these scores across time. We also calculated the time-weighted sum of PRID (SPRID) scores at 60 and 120 minutes. We analyzed the PRID and SPRID scores by using an analysis of variance model with treatment, baseline DPS score and site terms in the model. We calculated duration of effect as the time difference between the onset of effect (the first of two consecutive periods in which pain intensity was reduced by at least one unit) and its offset (the first of two time points in which pain intensity returned to baseline levels or higher), and we compared these durations between treatments by using the Cox proportional hazards model. We also used the Cox proportional hazards model to analyze the time to dropping out of the study. We calculated all 95 percent confidence intervals on the basis of the corresponding fitted model. We analyzed the global satisfaction scores among treatments by using the CMH test and modified ridit scores.
We calculated the percentage of participants who applied no more than 400 mg of gel, and we graphed the amount of gel applied per participant in 200-mg intervals as a histogram.
RESULTS
A total of 577 participants enrolled in the study, and 576 self-applied study medication (Figure 2). One participant did not apply study medication and was excluded in the final analyses. Among all participants, 100 were minors (aged 12-17 years). Table 1 (page 520) illustrates the demographic characteristics and baseline pain scores for each treatment group. We found no significant differences among treatment groups.
Figure 2.

Flow diagram of participant study inclusion and exclusion.
TABLE 1.
| CHARACTERISTIC | OVERALL STUDY POPULATION (N = 576) |
VEHICLE (n = 115) |
10 PERCENT BENZOCAINE (n = 233) |
20 PERCENT BENZOCAINE (n = 228) |
|---|---|---|---|---|
|
| ||||
| Sex, No. (%) | ||||
| Male | 276 (47.9) | 53 (46.1) | 113 (48.5) | 110 (48.2) |
| Female | 300 (52.1) | 62 (53.9) | 120 (51.5) | 118 (51.8) |
|
| ||||
| Age, Years | ||||
| Mean (SD‡) | 31.1 (12.7) | 31.2 (12.6) | 30.8 (12.7) | 31.3 (12.8) |
| Range | 12-82 | 12-65 | 12-82 | 13-70 |
|
| ||||
| Adolescents, No. (%) | ||||
| 12-14 years | 31 (5.4) | 7(6.1) | 13 (5.6) | 11 (4.8) |
| 15-17 years | 69 (12.0) | 13 (11.3) | 33 (14.2) | 23 (10.1) |
|
| ||||
| Race, No. (%) | ||||
| Black | 365 (63.4) | 78 (67.8) | 145 (62.2) | 142 (62.3) |
| White | 180 (31.3) | 31 (27.0) | 73 (31.3) | 76 (33.3) |
| Asian | 14 (2.4) | 3 (2.6) | 7 (3.0) | 4 (1.8) |
| Other (mixed racial origins) | 10 (1.7) | 2(1.7) | 5(2.1) | 3(1.3) |
| American Indian/Alaskan | 5 (0.9) | 1 (0.9) | 3(1.3) | 1 (0.4) |
| Native | ||||
| Native Hawaiian/ other Pacific Islander |
1 (0.2) | 0 (0) | 0 (0) | 1 (0.4) |
| Not reported | 1 (0.2) | 0(0) | 0(0) | 1 (0.4) |
|
| ||||
| Ethnicity, No. (%) | ||||
| Non-Hispanic or non-Latino | 537 (93.2) | 108 (93.9) | 218 (93.6) | 211 (92.5) |
| Hispanic or Latino | 39 (6.8) | 7(6.1) | 15 (6.4) | 17 (7.5) |
|
| ||||
| Weight, Pounds | ||||
| Mean (SD) | 179.3 (51.2) | 184.8 (54.4) | 179.5 (54.2) | 176.4 (46.1) |
| Range | 66-410 | 104-366 | 83-410 | 66-350 |
|
| ||||
|
Baseline Pain Dental
Pain Scale Score, No. (%) |
||||
| Moderate | 354 (61.5) | 71 (61.7) | 144 (61.8) | 139 (61.0) |
| Severe | 222 (38.5) | 44 (38.3) | 89 (38.2) | 89 (39.0) |
|
| ||||
|
Baseline Pain Visual
Analog Scale Score, Millimeters |
||||
| Mean (SD) | 73.5 (14.3) | 74.1 (13.4) | 73.3 (14.5) | 73.5 (14.7) |
| Range | 49-100 | 51-100 | 49-100 | 50-100 |
Not all percentage totals equal 100 percent owing to rounding.
Treatment groups were comparable with respect to their demographic and baseline characteristics.
SD: Standard deviation.
Table 2 displays the percentage of responders, and Table 3 shows the overall observed differences and 95 percent confidence intervals calculated by using the CMH model, with P values comparing each pair of treatment groups. Both 10 percent and 20 percent benzocaine gels were statistically better than the vehicle gel (P = .038 and P < .001, respectively). We observed a dose-response relationship: the 20 percent benzocaine group had 6.6 percent more responders than did the 10 percent benzocaine group (P = .047).
TABLE 2.
Responders, according to treatment type.
| TREATMENT | RESPONDERS, NO. (%) |
|---|---|
| Vehicle (n = 115) | 81 (70.4) |
| 10 Percent Benzocaine (n = 233) | 188 (80.7) |
| 20 Percent Benzocaine (n = 228) | 199 (87.3) |
TABLE 3.
Differences in participants receiving 10 percent benzocaine, 20 percent benzocaine or vehicle gel.
| TREATMENT | PAIRWISE COMPARISONS | |
|---|---|---|
| Observed Treatment Differences, % (95 Percent CI*) |
P Value† |
|
|
20 Percent Benzocaine
Versus Vehicle |
16.8 (7.2-25.7) | < .001‡ |
|
10 Percent Benzocaine
Versus Vehicle |
10.3 (0.3-19.3) | .038‡ |
|
20 Percent Benzocaine
Versus 10 Percent Benzocaine |
6.6 (0.2-13.3) | .047‡ |
The 95 percent confidence interval (CI) was calculated on the basis of the Cochran-Mantel-Haenszel weighted percentages and corresponding standard errors.
P values are from the Cochran-Mantel-Haenszel test, controlling for site and baseline dental pain scale score.
The first treatment was significantly better than was the second treatment at the .05 level.
Table 4 and Table 5 display a summary of the analyses for the secondary efficacy variables. Both 10 percent and 20 percent benzocaine gels had statistically more rapid median onset times than did the vehicle gel for first perceptible relief and meaningful relief (P < .001), with 20 percent benzocaine gel having a significantly more rapid median onset time than did the 10 percent gel for confirmed first perceptible relief (P =.030). In addition, 20 percent benzocaine gel was statistically better than the vehicle gel for SPRID at 60 minutes (P = .035). Figure 3 illustrates the time-effect curves for PRID for the three treatment groups through 120 minutes. Both benzocaine gels also were significantly (P < .05) more efficacious than the vehicle gel for mean global satisfaction scores. Figure 4 (page 524) illustrates the percentage of participants who rated their global satisfaction as poor, fair, good, very good or excellent for each treatment group. Seventy-nine percent of participants who received the 20 percent benzocaine gel and 80 percent of participants who received the 10 percent benzocaine gel assigned a global satisfaction score of good, very good or excellent compared with 61 percent of participants who received the vehicle gel.
TABLE 4.
Summary of the time elapsed from baseline to the event efficacy parameters for the three treatment groups.
| PARAMETER | TREATMENT | HAZARD RATIO (95 PERCENT CONFIDENCE INTERVAL; P VALUE*) |
||||
|---|---|---|---|---|---|---|
| Vehicle (n = 115) |
10 Percent Benzocaine (n = 233) |
20 Percent Benzocaine (n = 228) |
20 Percent Benzocaine Versus Vehicle |
10 Percent Benzocaine Versus Vehicle |
20 Percent Benzocaine Versus 10 Percent Benzocaine |
|
|
Median Time Elapsed From
Baseline to Meaningful Relief, Minutes |
8.5 | 4.4 | 3.2 | 2.0† (1.6 to 2.7†; < .001‡) |
1.7† (1.3 to 2.3†; < .001‡) |
1.2† (1.0 to 1.4†; .100) |
|
Median Time Elapsed From
Baseline to Confirmed First Perceptible Relief, Minutes |
2.0 | 1.4 | 1.1 | 2.0† (1.6 to 2.6†; < .001‡) |
1.6† (1.3 to 2.1†; < .001‡) |
1.2† (1.0 to 1.5†; .030‡) |
|
Median Duration of Effect,
Minutes |
> 115 | > 115 | > 115 | 0.9† (0.6 to 1.2†; .492) |
0.9† (0.7 to 1.3†; .649) |
1.0† (0.7 to 1.3†; .773) |
|
Median Time Elapsed Before
Dropping Out, Minutes |
> 120 | > 120 | > 120 | 1.2† (0.7 to 2.1†; .484) |
1.1† (0.6 to 2.0†; .653) |
1.1† (0.7 to 1.7†; .752) |
P values for meaningful relief, confirmed first perceptible relief, duration of effect and time elapsed before dropping out were derived from the Cox proportion hazards model with terms for treatment, site and baseline dental pain scale score.
The hazard ratio of the first treatment relative to the second treatment and corresponding 95 percent confidence intervals were based on the Wald statistic.
The first treatment was significantly better than was the second treatment at the P ≤ .05 level.
Table 5.
Summary of SPRID* scores for the three treatment groups.
| PARAMETER | TREATMENT | OBSERVED TREATMENT DIFFERENCE (95 PERCENT CONFIDENCE INTERVAL; P VALUE) |
||||
|---|---|---|---|---|---|---|
| Vehicle (n = 115) |
10 Percent Benzocaine (n = 233) |
20 Percent Benzocaine (n = 228) |
20 Percent Benzocaine Versus Vehicle |
10 Percent Benzocaine Versus Vehicle |
20 Percent Benzocaine Versus 10 Percent Benzocaine |
|
|
SPRID at 60
Minutes, Mean (SD†) |
3.1 (2.3) | 3.4 (2.0) | 3.6 (2.0) | 0.5 (0.0 to 1.0‡; .035§) |
0.3 (−0.1 to 0.8‡; .173) |
0.2 (−0.2 to 0.6‡; .358) |
|
SPRID at
120 Minutes, Mean (SD) |
5.9 (4.8) | 6.4 (4.2) | 6.7 (4.3) | 0.8 (−0.2 to 1.7‡; .135) |
0.5 (−0.5 to 1.5‡; .332) |
0.3 (−0.5 to 1.1‡; .517) |
SPRID: Time-weighted sum of pain relief combined with pain intensity difference. P values for SPRID 60 and SPRID 120 were derived from the analysis of variance (ANOVA) model with treatment, site and baseline dental pain scale (DPS) score.
SD: Standard deviation.
The 95 percent confidence intervals were calculated on the basis of the least squares means from the ANOVA model with treatment, site and baseline DPS score.
The first treatment was significantly better than was the second treatment at the P ≤ .05 level.
Figure 3.
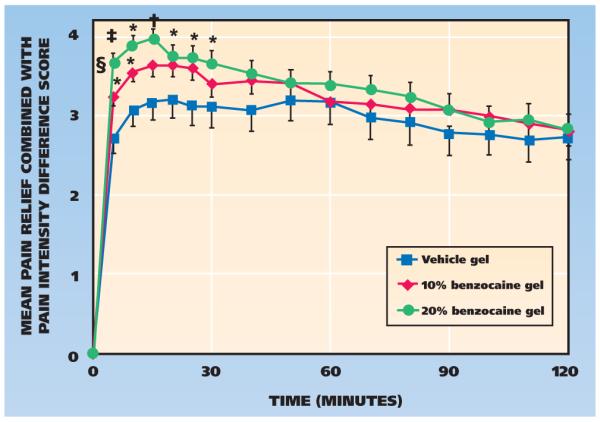
Time-effect curves for pain relief combined with pain intensity difference (PRID) (standard error of the mean) through 120 minutes after self-application. * Significantly better than vehicle gel (P ≤ .05). † Significantly better than vehicle gel (P ≤ .01). ‡ Significantly better than vehicle gel (P ≤ .001). § Significantly better than 10 percent benzocaine gel (P ≤ .05).
Figure 4.

Percentage of participants who rated the global satisfaction of each treatment gel as poor, fair, good, very good or excellent. * Significantly better than vehicle (P ≤ .05). The percentages for 10 percent benzocaine total 99 percent owing to rounding.
Participants applied a mean (standard deviation) of 235.6 (148.7) mg (median, 203; range, 18-1,026 mg) of study gel, with 88.2 percent of participants applying 400 mg or less. Only one participant, a 29-year-old man randomly assigned to the 20 percent benzocaine gel group, applied more than 1,000 mg of study gel. He stated he wanted “instant relief” from his pain, and when he placed more medication on his finger than the picture on the label, he knew he could not put it back, so he applied it all. Figure 5 (page 524) presents the distribution of the amount of study gel applied in 200-mg intervals.
Figure 5.
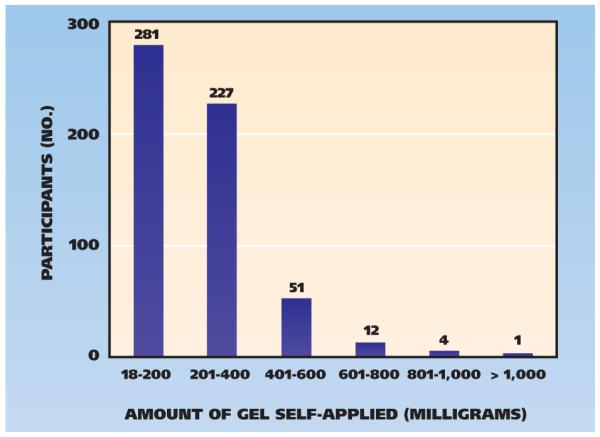
Number of participants self-applying various amounts of study gel in 200-milligram increments.
Participants reported only 16 AEs in this study; four (3.5 percent) of 115 participants in the vehicle gel group, six (2.6 percent) of 233 participants in the 10 percent benzocaine gel group and six (2.6 percent) of 228 participants in the 20 percent benzocaine gel group. We rated all AEs as mild in intensity except for one AE in a participant in the vehicle gel group that was rated as moderate. The most common AEs were transient increases in blood pressure (n = 3) and gastrointestinal complaints (n = 2). We observed no cases of methemoglobinemia. There were no significant differences between treatment groups in the overall incidence of AEs or the incidence of any particular AE.
DISCUSSION
The results of our study demonstrated that for the primary efficacy endpoint of percentage of responders, both 10 percent and 20 percent benzocaine gels were significantly more efficacious than was the vehicle gel and the 20 percent benzocaine gel was significantly more efficacious than was the 10 percent benzocaine gel in the relief of toothache pain. To our knowledge, our study is the first with results demonstrating a dose response between the 10 percent and 20 percent benzocaine treatments. The dose-response relationship supports the availability of both regular strength (10 percent) and maximum strength (20 percent) formulations. The clinical importance of an increase of five percentage points in PR is supported by the results of a 2004 systematic review of the outcome difference between regular and extra-strength acetaminophen.60 In that meta-analysis, the results showed a difference of five percentage points in the number of participants reaching the response threshold when investigators compared maximum strength and regular strength acetaminophen. Thus, a difference of five percentage points has been accepted as being a clinically significant difference. In our study, participants we randomly assigned to the 20 percent benzocaine gel group had a significantly quicker onset of confirmed first perceptible relief than did participants we randomly assigned to the 10 percent benzocaine gel group. Both 10 percent and 20 percent benzocaine gels also were statistically better than vehicle gel with regard to a number of secondary endpoints (Table 4, Table 5, Figure 3 and Figure 4).
There was a high percentage of positive responders in the vehicle group. A placebo response rate as high as 30 percent is not uncommon in studies of analgesics for a variety of reasons, including participant expectation. In topical application, there also may be a vehicle effect resulting from protection of the lesion from the environment. In addition, the vehicle composition might have an effect. Polyethylene glycol is used as the solvent in benzocaine solutions because the local anesthetic is poorly soluble in water.61,62 In our study, the concentrations of polyethylene glycol in the 20 percent benzocaine, 10 percent benzocaine and vehicle gels were 77 percent, 87 percent and 97 percent, respectively. Results from laboratory experiments indicated that 40 percent polyethylene glycol completely abolishes compound action potentials with significant diminution of C-fiber nerve activity beginning at a concentration of 30 percent.63 Thus, the vehicle used commercially to keep benzocaine in solution is likely to be active and may not be a “true placebo” per se. Investigators reported analgesic response rates of 47 percent and 60 percent for polyethylene glycol gel and liquid, respectively, in study participants with toothaches.5,64
In our study, participants’ compliance with label dose administration directions was good, with 88.2 percent applying 400 mg or less of study gel. The product label we gave participants in this study was evaluated first in a small 30-participant pilot study.5 The picture depicting how much gel to apply is not on label directions for benzocaine gels, and we believe this graphic contributed to the favorable label dose administration direction compliance rates in our study and should be considered in future label directions for benzocaine gels. To our knowledge, our study is the first evaluation of compliance with label dose administration directions in a large cohort of participants, including adolescents as young as 12 years, who had moderate to severe toothache pain.
The fact that we did not evaluate the application of multiple doses of the study gels across a day was one of the limitations of our study. We have no data regarding whether participants who were assigned randomly to the benzocaine gel groups would have used the gel more than four times per day (the maximum dosage stated on the labels of benzocaine toothache products). Because our goal was to enroll participants in the study and have them receive definitive treatment for their symptomatic tooth the same day, conducting a multiple-dose study was not feasible or ethical.
Although reports of methemoglobinemia associated with benzocaine administration are a growing concern to the FDA,56 methemoglobinemia rarely occurs with the OTC use of benzocaine products for the temporary relief of toothache pain.54,55 Drug-induced methemoglobinemia most often is an adverse event that occurs after an overdose of a strong oxidizing drug such as nitroglycerin, benzocaine, prilocaine, phenelzine (a monoamine oxidase inhibitor) or ciprofloxacin. When people have excessive levels of these drugs in their blood, the reduced form of hemoglobin (ferrous state) is converted into oxidized methemoglobin (ferric state), which has poor oxygen-carrying capacity.5,13,65,66 Even the participant in our study who administered the greatest amount of gel (1,026 mg), which would translate to a 10 percent benzocaine dose of 103 mg and a 20 percent benzocaine dose of 205 mg, still would be sevenfold and 3.5-fold, respectively, below the reported methemoglobinemia threshold dose of 15 mg per kilogram in a person weighing as little as 50 kg.15,49 The second highest amount of gel administered by any participant in our study was 870 mg, and only five participants (0.8 percent) administered 800 mg or more of gel.
CONCLUSION
Both 10 percent and 20 percent benzocaine gels were effective in the temporary relief of toothache pain and were well tolerated. Most participants were able to correctly self-apply doses of benzocaine that were at least 10-fold below the reported threshold that could lead to methemoglobinemia. All study gels were well tolerated.
Acknowledgments
This study was supported by a grant from Pfizer Consumer Healthcare (Madison, N.J.) and Church & Dwight (Princeton, N.J.) to Drs. Hersh, Ciancio, Moore, Casamassimo, Jeffers, Corby, Papas and Gordon.
The authors would like to acknowledge the following people for their significant efforts in the successful conduct of this study: Joel Waksman, PhD (Brightech International, Somerset, N.J.); Annahita Ghassemi, PhD; William Hooper, PhD; Linda Vorwerk, BS (Church & Dwight, Princeton, N.J.); William Cooley, PhD (Cooley Consulting, Wyoming, Ohio); Paul Desjardins, DMD, PhD (Desjardins Associates, Maplewood, N.J.); William Thompson, PhD (Georgia Regents University, Augusta); Monika Epler, MA (New York University, New York City); Lisa Baird, BS, MS; Elizabeth DePadova, BS; Xiaoli Hu, MS; Sudam Pathirana, PhD; Emanuel Troullos, DMD, MPH (Pfizer Consumer Healthcare, Madison, N.J.); Michele Bessinger, BS; Sandra Law, RDH (State University of New York at Buffalo); Stephen Cooper, DMD, PhD (Stephen A Cooper, DMD, PhD, Palm Beach Gardens, Fla.); Michele Meeker, RDH, MS (University of Maryland, Baltimore); Stacey Secreto (University of Pennsylvania, Philadelphia); Jayme Zovko, RDH, BS (University of Pittsburgh).
ABBREVIATION KEY
- AE
Adverse event
- DPS
Dental pain scale
- FDA
Food and Drug Administration
- OTC
Over the counter
- PID
Pain intensity difference
- PR
Pain relief
- PRID
Pain relief combined with pain intensity difference
- SPRID
Time-weighted sum of pain relief combined with pain intensity difference
Footnotes
Disclosure. Ms. Leyva is an employee of Pfizer Consumer Healthcare and owns stock in Pfizer. None of the other authors reported any disclosures.
Contributor Information
Dr. Elliot V. Hersh, Division of Pharmacology and Therapeutics, Department of Oral Surgery and Pharmacology, School of Dental Medicine, University of Pennsylvania, 240 S. 40th St., Philadelphia, Pa. 19104-6030.
Dr. Sebastian G. Ciancio, Department of Periodontics and Endodontics, and is the director, Center for Dental Studies, School of Dental Medicine, The State University of New York at Buffalo.
Dr. Arthur S. Kuperstein, Department of Oral Medicine, School of Dental Medicine, University of Pennsylvania, Philadelphia.
Dr. Eric T. Stoopler, Department of Oral Medicine, School of Dental Medicine, University of Pennsylvania, Philadelphia.
Dr. Paul A. Moore, Department of Dental Anesthesiology, School of Dental Medicine, University of Pittsburgh.
Dr. Sean G. Boynes, Department of Dental Anesthesiology, School of Dental Medicine, University of Pittsburgh, when this article was written. He now is the director of dental medicine at CareSouth Carolina, Society Hill, S.C.
Dr. Steven C. Levine, Department of Diagnostic Sciences, School of Dental Medicine, University of Pittsburgh.
Dr. Paul Casamassimo, Nationwide Children’s Hospital, Columbus, Ohio.
Ms. Rina Leyva, Pfizer Consumer Healthcare, Madison, N.J.
Dr. Tanya Mathew, Department of Pediatric Dentistry, School of Dentistry, The Ohio State University, Columbus.
Dr. Othman Shibly, Department of Periodontics and Endodontics, School of Dental Medicine, The State University of New York at Buffalo.
Dr. Paul Creighton, Department of Pediatric and Community Dentistry, School of Dental Medicine, The State University of New York at Buffalo.
Dr. Gary E. Jeffers, Department of Oral and Maxillofacial Surgery, School of Dentistry, University of Detroit Mercy.
Dr. Patricia M.A. Corby, Department of Periodontics, and the associate director, Bluestone Center for Clinical Research, College of Dentistry, New York University, New York City.
Dr. Stanley N. Turetzky, Department of Oral and Maxillofacial Pathology, Radiology and Medicine, College of Dentistry, New York University, New York City.
Dr. Athena Papas, School of Dental Medicine, Tufts University, Boston.
Dr. Jillian Wallen, Department of Growth and Development, University of Nebraska Medical Center, Omaha, Neb.
Dr. Cynthia Idzik-Starr, Department of Oral and Maxillofacial Surgery, School of Dentistry, University of Maryland, Baltimore.
Dr. Sharon M. Gordon, Department of Oral-Maxillofacial Surgery, School of Dentistry, University of Maryland, Baltimore.
References
- 1.Some uses of anesthesin. Merck’s Arch. 1903;5(1):27. [Google Scholar]
- 2.U.S. Food and Drug Administration Oral Health Care Drug Products for Over-the-Counter Human Use: Amendment to Tentative Final Monograph to Include OTC Relief of Oral Discomfort Drug Products—Notice of Proposed Rulemaking. Fed Regist. 1991;56(185):48302–48347. [Google Scholar]
- 3.Gangarosa LP, Sr, Ciarlone AE, Neaverth EJ, Johnston CA, Snowden JD, Thompson WO. Use of verbal descriptors, thermal scores and electrical pulp testing as predictors of tooth pain before and after application of benzocaine gels into cavities of teeth with pulpitis. Anesth Prog. 1989;36(6):272–275. [PMC free article] [PubMed] [Google Scholar]
- 4.Sveen OB, Yaekel M, Adair SM. Efficacy of using benzocaine for temporary relief of toothache. Oral Surg Oral Med Oral Pathol. 1982;53(6):574–576. doi: 10.1016/0030-4220(82)90342-5. [DOI] [PubMed] [Google Scholar]
- 5.Hersh EV, Stoopler ET, Secreto SA, DeRossi SS. A study of benzocaine gel dosing for toothache. J Clin Dent. 2005;16(4):103–108. [PubMed] [Google Scholar]
- 6.Hersh EV, DeRossi SS, Ciarrocca KN, Secreto SA, Ghassemi A. Efficacy and tolerability of an intraoral benzocaine patch in the relief of spontaneous toothache pain. J Clin Dent. 2003;14(1):1–6. [PubMed] [Google Scholar]
- 7. [Accessed June 29, 2012];Orajel Maximum Strength Toothache Pain Relief Gel: view product label. www.orajel.com/adult-oral-care/toothache/Products/orajel-maximum-strength-toothache-pain-relief-gel.aspx.
- 8.Aepfelbacher FC, Breen P, Manning WJ. Methemoglobinemia and topical pharyngeal anesthesia. N Engl J Med. 2003;348(1):85–86. doi: 10.1056/NEJM200301023480122. [DOI] [PubMed] [Google Scholar]
- 9.Nguyen ST, Cabrales RE, Bashour CA, et al. Benzocaine-induced methemoglobinemia. Anesth Analg. 2000;90(2):369–371. doi: 10.1097/00000539-200002000-00024. [DOI] [PubMed] [Google Scholar]
- 10.Ellis FD, Seiler JG, 3rd, Palmore MM., Jr Methemoglobinemia: a complication after fiberoptic orotracheal intubation with benzocaine spray—a case report. J Bone Joint Surg Am. 1995;77(6):937–939. [PubMed] [Google Scholar]
- 11.Carlson G, Negri E, McGrew A, Plaisier B. Two cases of methemoglobinemia from the use of topical anesthetics. J Emerg Nurs. 2003;29(2):106–108. doi: 10.1067/men.2003.57. [DOI] [PubMed] [Google Scholar]
- 12.Udeh C, Bittikofer J, Sum-Ping ST. Severe methemoglobinemia on reexposure to benzocaine. J Clin Anesth. 2001;13(2):128–130. doi: 10.1016/s0952-8180(01)00222-7. [DOI] [PubMed] [Google Scholar]
- 13.Gupta PM, Lala DS, Arsura EL. Benzocaine-induced methemoglobinemia. South Med J. 2000;93(1):83–86. [PubMed] [Google Scholar]
- 14.Spielman FJ, Anderson JA, Terry WC. Benzocaine-induced methemoglobinemia during general anesthesia. J Oral Maxillofac Surg. 1984;42(11):740–743. doi: 10.1016/0278-2391(84)90424-5. [DOI] [PubMed] [Google Scholar]
- 15.Rodriguez LF, Smolik LM, Zbehlik AJ. Benzocaine-induced methemoglobinemia: report of a severe reaction and review of the literature. Ann Pharmacother. 1994;28(5):643–649. doi: 10.1177/106002809402800515. [DOI] [PubMed] [Google Scholar]
- 16.Bernstein BM. Cyanosis following use of anesthesin: case report. Rev Gastroenterol. 1950;17(2):123. [PubMed] [Google Scholar]
- 17.Douglas WW, Fairbanks VF. Methemoglobinemia induced by a topical anesthetic spray (cetacaine) Chest. 1977;71(5):587–591. doi: 10.1378/chest.71.5.587. [DOI] [PubMed] [Google Scholar]
- 18.Collins JF. Methemoglobinemia as a complication of 20% benzocaine spray for endoscopy. Gastroenterology. 1990;98(1):211–213. doi: 10.1016/0016-5085(90)91312-t. [DOI] [PubMed] [Google Scholar]
- 19.Anderson ST, Hajduczek J, Barker SJ. Benzocaine-induced methemoglobinemia in an adult: accuracy of pulse oximetry with methemoglobinemia. Anesth Analg. 1988;67(11):1099–1101. [PubMed] [Google Scholar]
- 20.Linares LA, Peretz TY, Chin J. Methemoglobinemia induced by topical anesthetic (benzocaine) Radiother Oncol. 1990;18(3):267–269. doi: 10.1016/0167-8140(90)90062-2. [DOI] [PubMed] [Google Scholar]
- 21.Vessely MB, Zitsch RP., 3rd Topical anesthetic-induced methemoglobinemia: a case report and review of the literature. Otolaryngol Head Neck Surg. 1993;108(6):763–767. doi: 10.1177/019459989310800623. [DOI] [PubMed] [Google Scholar]
- 22.Guay J. Methemoglobinemia related to local anesthetics: a summary of 242 episodes. Anesth Analg. 2009;108(3):837–845. doi: 10.1213/ane.0b013e318187c4b1. [DOI] [PubMed] [Google Scholar]
- 23.Mogos M, Thangathurai D, Roffey P, Tay C. Cetacaine-induced complication during transesophageal echocardiography placement (published online ahead of print Aug. 31, 2009) J Cardiothorac Vasc Anesth. 2010;24(4):736. doi: 10.1053/j.jvca.2009.06.018. doi:10.1053/j.jvca.2009.06.018. [DOI] [PubMed] [Google Scholar]
- 24.Jiminez MA, Polena S, Coplan NL, Patel K, Gintautas J. Methemoglobinemia and transesophageal echo. Proc West Pharmacol Soc. 2007;50:134–135. [PubMed] [Google Scholar]
- 25.Lambert AM, Eggleston KL, Smalligan RD, Byrd RP, Jr, Roy TM. Cyanosis following transesophageal echocardiogram. W V Med J. 2008;104(3):10–15. [PubMed] [Google Scholar]
- 26.Young B. Intraoperative detection of methemoglobinemia in a patient given benzocaine spray to relieve discomfort from a nasogastric tube: a case report. AANA J. 2008;76(2):99–102. [PubMed] [Google Scholar]
- 27.Gul W, Chandra M, Sarodia B, Qazi A. Methemoglobinemia: hypotension and oxygen desaturation after transesophageal echocardiography. J Ark Med Soc. 2008;104(8):182–183. [PubMed] [Google Scholar]
- 28.Kwok S, Fischer JL, Rogers JD. Benzocaine and lidocaine induced methemoglobinemia after bronchoscopy: a case report. J Med Case Rep. 2008;2:16. doi: 10.1186/1752-1947-2-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kane GC, Hoehn SM, Behrenbeck TR, Mulvagh SL. Benzocaine-induced methemoglobinemia based on the Mayo Clinic experience from 28 478 transesophageal echocardiograms: incidence, outcomes, and predisposing factors. Arch Intern Med. 2007;167(18):1977–1982. doi: 10.1001/archinte.167.18.1977. [DOI] [PubMed] [Google Scholar]
- 30.Lin SK, Wu JL, Lee YL, Tsao SL. Methemoglobinemia induced by exposure to topical benzocaine for an awake nasal intubation: a case report. Acta Anaesthesiol Taiwan. 2007;45(2):111–116. [PubMed] [Google Scholar]
- 31.Throm MJ, Stevens MD, Hansen C. Benzocaine-induced methemoglobinemia in two patients: interdisciplinary collaboration, management, and near misses. Pharmacotherapy. 2007;27(8):1206–1214. doi: 10.1592/phco.27.8.1206. [DOI] [PubMed] [Google Scholar]
- 32.Abu-Laban RB, Zed PJ, Purssell RA, Evans KG. Severe methemoglobinemia from topical anesthetic spray: case report, discussion and qualitative systematic review. CJEM. 2001;3(1):51–56. doi: 10.1017/s1481803500005182. [DOI] [PubMed] [Google Scholar]
- 33.Saha SA, Kordouni MR, Siddiqui M, Arora RR. Methemoglobinemia-induced cardio-respiratory failure secondary to topical anesthesia. Am J Ther. 2006;13(6):545–549. doi: 10.1097/01.mjt.0000208876.69103.c7. [DOI] [PubMed] [Google Scholar]
- 34.Jaffery Z, Ananthasubramaniam K. A rare side effect of transesophageal echocardiography: methemoglobinemia from topical benzocaine anesthesia. Eur J Echocardiogr. 2008;9(2):289–290. doi: 10.1016/j.euje.2006.09.003. [DOI] [PubMed] [Google Scholar]
- 35.Basra SK, Vives MJ, Reilly MC, Reiter MF, Kushins LG. Methemoglobinemia after fiberoptic intubation in a patient with an unstable cervical fracture: a case report. J Spinal Disord Tech. 2006;19(4):302–304. doi: 10.1097/01.bsd.0000204503.07096.bf. [DOI] [PubMed] [Google Scholar]
- 36.BheemReddy S, Messineo F, Roychoudhury D. Methemoglobinemia following transesophageal echocardiography: a case report and review. Echocardiography. 2006;23(4):319–321. doi: 10.1111/j.1540-8175.2006.00159.x. [DOI] [PubMed] [Google Scholar]
- 37.Hegedus F, Herb K. Benzocaine-induced methemoglobinemia. Anesth Prog. 2005;52(4):136–139. doi: 10.2344/0003-3006(2005)52[136:BM]2.0.CO;2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Dahshan A, Donovan GK. Severe methemoglobinemia complicating topical benzocaine use during endoscopy in a toddler: a case report and review of the literature. Pediatrics. 2006;117(4):e806–e809. doi: 10.1542/peds.2005-1952. [DOI] [PubMed] [Google Scholar]
- 39.Jacka MJ, Kruger M, Glick N. Methemoglobinemia after transesophageal echocardiography: a life-threatening complication. J Clin Anesth. 2006;18(1):52–54. doi: 10.1016/j.jclinane.2005.04.008. [DOI] [PubMed] [Google Scholar]
- 40.Birchem SK. Benzocaine-induced methemoglobinemia during transesophageal echocardiography. J Am Osteopath Assoc. 2005;105(8):381–384. [PubMed] [Google Scholar]
- 41.Srikanth MS, Kahlstrom R, Oh KH, Fox SR, Fox ER, Fox KM. Topical benzocaine (Hurricaine) induced methemoglobinemia during endoscopic procedures in gastric bypass patients. Obes Surg. 2005;15(4):584–590. doi: 10.1381/0960892053723376. [DOI] [PubMed] [Google Scholar]
- 42.LeClaire AC, Mullett TW, Jahania MS, Flynn JD. Methemoglobinemia secondary to topical benzocaine use in a lung transplant patient (published online ahead of print Jan. 11, 2005) Ann Pharmacother. 2005;39(2):373–376. doi: 10.1345/aph.1E315. doi:10.1345/aph.1E315. [DOI] [PubMed] [Google Scholar]
- 43.Ash-Bernal R, Wise R, Wright SM. Acquired methemoglobinemia: a retrospective series of 138 cases at 2 teaching hospitals. Medicine (Baltimore) 2004;83(5):265–273. doi: 10.1097/01.md.0000141096.00377.3f. [DOI] [PubMed] [Google Scholar]
- 44.Bayard M, Farrow J, Tudiver F. Acute methemoglobinemia after endoscopy. J Am Board Fam Pract. 2004;17(3):227–229. doi: 10.3122/jabfm.17.3.227. [DOI] [PubMed] [Google Scholar]
- 45.Tush GM, Kuhn RJ. Methemoglobinemia induced by an over-the-counter medication. Ann Pharmacother. 1996;30(11):1251–1254. doi: 10.1177/106002809603001109. [DOI] [PubMed] [Google Scholar]
- 46.Adachi T, Fukumoto M, Uetsuki N, Yasui O, Hayashi M. Suspected severe methemoglobinemia caused by topical application of an ointment containing benzocaine around the enterostomy. Anesth Analg. 1999;88(5):1190–1191. doi: 10.1097/00000539-199905000-00051. [DOI] [PubMed] [Google Scholar]
- 47.Klein SL, Nustad RA, Feinberg SE, Fonseca RJ. Acute toxic methemoglobinemia caused by a topical anesthetic. Pediatr Dent. 1983;5(2):107–108. [PubMed] [Google Scholar]
- 48.Townes PL, Geertsma MA, White MR. Benzocaine-induced methemoglobinemia. Am J Dis Child. 1977;131(6):697–698. doi: 10.1001/archpedi.1977.02120190091021. [DOI] [PubMed] [Google Scholar]
- 49.Potter JL, Hillman JV. Benzocaine-induced methemoglobinemia. JACEP. 1979;8(1):26–27. doi: 10.1016/s0361-1124(79)80446-3. [DOI] [PubMed] [Google Scholar]
- 50.Chung NY, Batra R, Itzkevitch M, Boruchov D, Baldauf M. Severe methemoglobinemia linked to gel-type topical benzocaine use: a case report (published online ahead of print Dec. 20, 2008) J Emerg Med. 2010;38(5):601–606. doi: 10.1016/j.jemermed.2008.06.025. doi:10.1016/j.jemermed.2008.06.025. [DOI] [PubMed] [Google Scholar]
- 51.Bong CL, Hilliard J, Seefelder C. Severe methemoglobinemia from topical benzocaine 7.5% (Baby Orajel) use for teething pain in a toddler (published online ahead of print Oct. 3, 2008) Clin Pediatr (Phila) 2009;48(2):209–211. doi: 10.1177/0009922808324491. doi:10.1177/0009922808324491. [DOI] [PubMed] [Google Scholar]
- 52.Darracq MA, Daubert GP. A cyanotic toddler. Pediatr Emerg Care. 2007;23(3):195–199. doi: 10.1097/PEC.0b013e3180330a2c. [DOI] [PubMed] [Google Scholar]
- 53.Balicer RD, Kitai E. Methemoglobinemia caused by topical teething preparation: a case report. ScientificWorldJournal. 2004;4:517–520. doi: 10.1100/tsw.2004.109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Gilman CS, Veser FH, Randall D. Methemoglobinemia from a topical oral anesthetic. Acad Emerg Med. 1997;4(10):1011–1013. [PubMed] [Google Scholar]
- 55.Orr TM, Orr DL., 2nd Methemoglobinemia secondary to over-the-counter Anbesol (published online ahead of print Oct. 16, 2010) Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;111(2):e7–e11. doi: 10.1016/j.tripleo.2010.06.011. doi:10.1016/j.tripleo.2010.06.011. [DOI] [PubMed] [Google Scholar]
- 56.FDA Drug Safety Communication [Accessed June 30, 2012];Reports of a rare, but serious and potentially fatal adverse effect with the use of over-the-counter (OTC) benzocaine gels and liquids applied to the gums or mouth. www.fda.gov/drugs/drugsafety/ucm250024.htm.
- 57.Desjardins PJ, Mehlisch DR, Chang DJ, et al. The time to onset and overall analgesic efficacy of rofecoxib 50 mg: a meta-analysis of 13 randomized clinical trials. Clin J Pain. 2005;21(3):241–250. doi: 10.1097/00002508-200505000-00007. [DOI] [PubMed] [Google Scholar]
- 58.Zuniga JR, Noveck RJ, Schmidt WK, Boesing SE, Hersh EV. Onset of action of diclofenac potassium liquid-filled capsules in dental surgery patients (published online ahead of print July 19, 2011) Curr Med Res Opin. 2011;27(9):1733–1739. doi: 10.1185/03007995.2011.600300. doi:10.1185/03007995.2011.600300. [DOI] [PubMed] [Google Scholar]
- 59.Hersh EV, Levin LM, Cooper SA, et al. Ibuprofen liquigel for oral surgery pain. Clin Ther. 2000;22(11):1306–1318. doi: 10.1016/s0149-2918(00)83027-1. [DOI] [PubMed] [Google Scholar]
- 60.Barden J, Edwards J, Moore A, McQuay H. Single dose oral paracetamol (acetaminophen) for postoperative pain. Cochrane Database Syst Rev. 2004;1:CD004602. doi: 10.1002/14651858.CD004602. [DOI] [PubMed] [Google Scholar]
- 61.Yagiela J. ADA/PDR Guide to Dental Therapeutics. 5th ed Physicians’ Desk Reference; Montvale, N.J.: 2009. Injectable and topical local anesthetics; pp. 1–25. [Google Scholar]
- 62.Hersh EV, Condouris GA. Local anesthetics: a review of their pharmacology and clinical use. Compendium. 1987;8(5):374, 376, 378–381. [PubMed] [Google Scholar]
- 63.Benzon HT, Gissen AJ, Strichartz GR, Avram MJ, Covino BG. The effect of polyethylene glycol on mammalian nerve impulses. Anesth Analg. 1987;66(6):553–559. [PubMed] [Google Scholar]
- 64.Hersh EV, Cooper SA, Segal H, Greene J. Analgesic onset time as a measure of topical anesthetic efficacy in spontaneous toothache pain: a pilot study. J Clin Dent. 1993;4(2):52–54. [PubMed] [Google Scholar]
- 65.Hall DL, Moses MK, Weaver JM, Yanich JP, Voyles JW, Reed DN. Dental anesthesia management of methemoglobinemia-susceptible patients: a case report and review of literature. Anesth Prog. 2004;51(1):24–27. [PMC free article] [PubMed] [Google Scholar]
- 66.Wilburn-Goo D, Lloyd LM. When patients become cyanotic: acquired methemoglobinemia. JADA. 1999;130(6):826–831. doi: 10.14219/jada.archive.1999.0306. [DOI] [PubMed] [Google Scholar]