

Abstract
We report a case of successful treatment of chronic hepatitis C infection with telaprevir-based triple therapy in a patient with hemophilia A complicated by factor VIII inhibitor. A twenty-two years old male with hereditary hemophilia A and high-titer factor VIII inhibitor was taking maintenance doses of recombinant factor VIII. He visited our clinic for treatment of his chronic hepatitis C with the newly instituted protease inhibitor based therapy. He was diagnosed with hepatitis C genotype 1a at one year of age. He was initiated on telaprevir, ribavirin and peg-interferon for treatment of hepatitis C and qualified for response-guided therapy. He completed treatment at 24 wk with minimal adverse effects. Notably, after 4 wk of hepatitis C treatment, his factor VIII inhibitor screen was negative and the dose for recombinant factor VIII decreased by half of the initial dosing before he was treated for hepatitis C. We suspect that suppressing hepatitis C may help decrease factor VIII inhibitor level and the need for recombinant factor VIII.
Keywords: Hepatitis C virus, Hemophilia, Factor VIII, Telaprevir, Factor VIII inhibitor, Protease inhibitor
Core tip: This is a case of a patient who has Hemophilia A with factor VIII inhibitor and chronic hepatitis C. After successfully treating the patient’s hepatitis C with protease-inhibitor based triple therapy and achieving response-guided therapy with negative hepatitis C virus RNA after week 4, the patient’s need for recombinant factor VIII decreased significantly.
INTRODUCTION
Chronic hepatitis C virus (HCV) infection has been a heavy burden to patients with hemophilia[1]. Patients with hemophilia A frequently receive transfusion of factor VIII as part of their management which can lead to development of antibodies that can neutralize factor VIII[2]. HCV infection by itself and its treatment with interferon can lead to the development of auto-antibodies including acquired factor VIII inhibitor[3,4]. Therefore, treating HCV in hemophiliacs with factor VIII inhibitor remains challenging.
CASE REPORT
A 22-year-old male with a history significant for hereditary hemophilia A complicated by refractory high-titer factor VIII inhibitors and hepatitis C genotype 1a infection diagnosed at the age of 1 year was referred to our clinic regarding hepatitis C treatment. The patient has been treated with recombinant human factor VIII 6000 IU Bid to maintain his factor level at around 20%. He was also receiving rituximab (to help decrease his factor VIII autoantibodies) every 4-6 mo for 3 years. Liver biopsy was not performed prior to starting HCV treatment due to concerns about bleeding and the patient was HCV treatment naive. Patient was started on hepatitis C telaprevir-based triple therapy (telaprevir 750 mg tid, weight based ribavirin, and peg-interferon alpha-2a) with good virologic response (HCV RNA was undetectable at treatment weeks 4, 12 and 24). He qualified for response-guided therapy and completed his treatment at 24 wk. He tolerated therapy relatively well without the need to dose reduce his ribavirin or peg-interferon alpha-2a. Interestingly, within a few days after starting telaprevir therapy his factor VIII level started to increase significantly and after four wk of hepatitis C treatment, his factor VIII inhibitor screen was negative and his need for recombinant factor VIII decreased by 50% as shown in Figure 1. His HCV RNA remained negative at 24 wk after he completed telaprevir-based therapy and the patient achieved a sustained virologic response.
Figure 1.
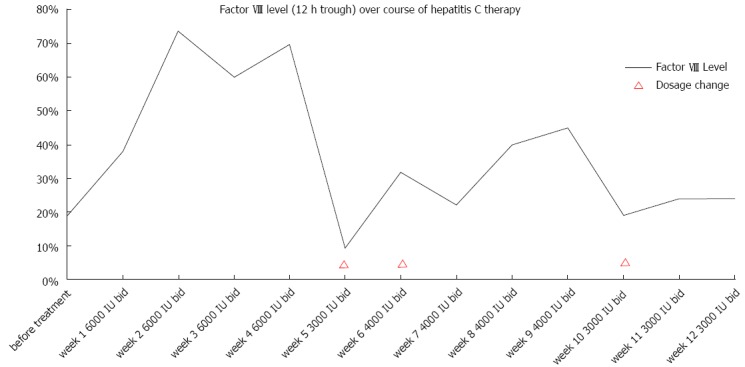
A graph demonstrating factor VIII levels and dosage while on telaprevir-based triple therapy.
DISCUSSION
To our knowledge, this is the first case report on using telaprevir-based triple therapy in a hemophilia patient with factor VIII inhibitor. Acquiring factor VIII inhibitor after HCV infection has been described in previous literature[5]. In our patient, we speculate that the HCV infection itself was inducing production of a factor VIII inhibitor. Consequently, the production of factor VIII inhibitor was suppressed once the virus was cleared with appropriate therapy. This case demonstrates that HCV therapy was safe and that suppressing HCV may help decrease factor VIII inhibitor level and the need for recombinant factor VIII. We hope that our report will encourage other practicing clinicians to treat this challenging patient population.
Footnotes
P- Reviewers Chen KB, Tan XR S- Editor Gou SX L- Editor A E- Editor Ma S
References
- 1.Alavian SM, Tabatabaei SV, Keshvari M, Behnava B, Miri SM, Elizee PK, Lankarani KB. Peginterferon alpha-2a and ribavirin treatment of patients with haemophilia and hepatitis C virus infection: a single-centre study of 367 cases. Liver Int. 2010;30:1173–1180. doi: 10.1111/j.1478-3231.2010.02296.x. [DOI] [PubMed] [Google Scholar]
- 2.Allain JP, Frommel D. Antibodies to factor VIII. V. Patterns of immune response to factor VIII in hemophilia A. Blood. 1976;47:973–982. [PubMed] [Google Scholar]
- 3.Stricker RB, Barlogie B, Kiprov DD. Acquired factor VIII inhibitor associated with chronic interferon-alpha therapy. J Rheumatol. 1994;21:350–352. [PubMed] [Google Scholar]
- 4.Sugishita K, Nagase H, Takahashi T, Takenaka K, Shiratori Y, Omata M. Acquired factor VIII inhibitor in a non-hemophilic patient with chronic hepatitis C viral infection. Intern Med. 1999;38:283–286. doi: 10.2169/internalmedicine.38.283. [DOI] [PubMed] [Google Scholar]
- 5.Dentale N, Fulgaro C, Guerra L, Fasulo G, Mazzetti M, Fabbri C. Acquisition of factor VIII inhibitor after acute hepatitis C virus infection. Blood. 1997;90:3233–3234. [PubMed] [Google Scholar]