

Abstract
IgG4-related systemic disease is an inflammatory disorder that can affect many organs. This case report describes a patient who in 2004 was found to have an inflammatory pseudotumor with IgG4 pathology. Over the next 3 years, visual symptoms responded well to recurrent courses of prednisone. In 2009, the patient developed chest pain and bradycardia with subsequent third-degree heart block, necessitating placement of a pacemaker. A subsequent PET scan showed extensive involvement of multiple organs as described in IgG4 disease as well as involvement of the myocardium and SA node. Pseudotumors involving the heart have been reported but have not been shown to be related to IgG4 disease. Although there was no pathology confirmation of heart involvement, the nature and extent of the organ involvement led us to conclude that it was due to IgG4-related disease. The use of the PET scan may help identify involvement of the myocardium.
Keywords: IgG4, inflammatory pseudotumor

Introduction
IgG4-related systemic disease is an inflammatory disorder that can affect many different organs. Specific criteria for diagnosis include elevated IgG4 serum levels, tissue IgG4 staining, and storiform fibrosis. Storiform fibrosis has a microscopic appearance of fibroblast collagen deposition in an irregularly whorled pattern resembling a straw mat. Consensus of the criteria for diagnosis is in progress. Depending on the individual organ, the histologic picture may differ. Involvement of the heart with pseudotumors has been described in several reports but has not been shown to be related to IgG4.
Case Report
The patient is a 59-year-old Caucasian female with pseudotumor in the eye since 2004. Her past medical history includes hypertension, obesity, dyslipidemia, Hashimoto’s thyroiditis, arthralgias, fatigue, idiopathic anemia, and plantar fasciitis. Family history is relevant for maternal coronary artery bypass grafting. In 2004, the patient consulted an ophthalmologist for eye pain, blurred vision, headaches, and vertigo. A CT scan of the orbits revealed enlarged oculomotor muscles (Figure 1). A biopsy revealed an inflammatory sclerosing pseudotumor (Figure 2). The patient was treated with prednisone 1 mg/kg/day for 3 months with complete resolution of symptoms.
Figure 1.
Comparative CT orbital scans taken in 2006 and after treatment in 2009. The black arrow shows an enlarged right eye muscle belly and inflamed oculomotor tendon insertions.
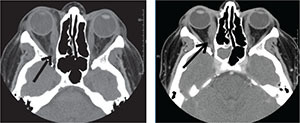
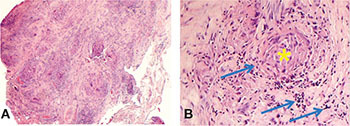
Figure 2.
Microscopic findings at 10x magnification of the left orbital biopsy included (A) fibrous adipose tissue and striated muscle fibers mostly replaced by dense fibrosis (B) with foci of lymphoplasmacytic infiltrate and focal granulomata without necrosis(*). At 50x magnification, it is easier to see the dense infiltrate of plasma cells (arrows) surrounding the granuloma (asterisk). [Pathology review with digital photos taken in 2010] Note: Granulomas form when the immune system attempts to wall off substances that it perceives as foreign but is unable to eliminate. A granuloma is therefore a special type of inflammation that can occur in a wide variety of diseases. The identification of necrosis in granulomas is important because granulomas with necrosis tend to have infectious causes. In the above tissue sample, there is no necrosis.
In 2006, the symptoms recurred. The initial biopsy was then reviewed and was positive for IgG4-related disease (Figure 3). Prednisone was resumed and methotrexate was added to the treatment regimen. On follow-up visits, the patient reported substantial symptom relief with increased doses of prednisone. In 2008, she experienced dyspepsia with substernal discomfort that was relieved by omeprazole; however, a year later the chest discomfort was no longer responsive to omeprazole. A cardiac work-up was done, and a computed tomography with coronary calcium scoring showed zero calcium in the coronary vessels. In May 2010, an esophagogastroduodenoscopy was normal. During this procedure, electrocardiographic monitoring showed a first-degree heart block. Four days later, the patient experienced an acute chest pain episode with dyspnea and was admitted to the hospital. Inpatient cardiac stress testing was normal. An echocardiogram and chest X-ray had revealed moderate cardiomegaly. Subsequently, the patient developed bradycardia with third-degree heart block, and a pacemaker was placed. Six months later, the patient continued complaining of resting chest pain.
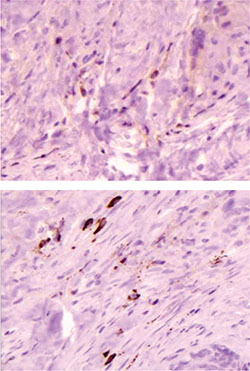
Figure 3.
IgG & IgG4 were used to evaluate the nature of the plasma cells. Results were reported as percentage of IgG4/IgG cells counted in 5 high-power fields. The overall results are IgG4/IgG = 77% (range 50-83%). Note: An IgG4/IgG ratio of >50% is one of several diagnostic criteria of IgG4-related disease.
Because of the history of IgG4 orbital disease, a pseudotumor of the heart was considered. A subsequent positron emission tomography (PET) revealed multi-organ involvement (right mandible, left carotid, paratracheal and para-aortic lymph nodes).1,2 Remarkable findings were fludeoxyglucose nuclear isotope uptake around the oculomotor muscle bellies and marked cardiac uptake with involvement of the sinoatrial node and left ventricle (Figure 4). The patient was treated with prednisone 60 mg/day, and cyclosporine was added later as steroids doses were reduced.
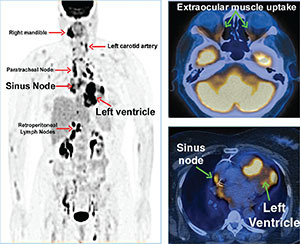
Figure 4.
This image shows positron emission tomography CT scan with nuclear isotope uptake around oculomotor muscle bellies, and marked paratracheal and cardiac uptake with involvement of the sinoatrial node and left ventricle.
Discussion
Approximately 40 case reports of cardiac pseudotumors have been recorded in the medical literature.3 Depending on the pathologic findings, some of these tumors were diagnosed as “plasma cell granulomas” and others were identified as “myofibroblastic tumors.” In addition to heart-related symptoms, many of these patients also complained of systemic symptoms of inflammatory disease including fever, general malaise, weight loss, and arthralgias. Common laboratory findings included thrombocytosis, thrombocytopenia, leukocytosis, hypergammaglobulinemia, and anemia.4 Although inflammatory cardiac pseudotumors have classically been treated with open heart surgery, some of these pseudotumors have decreased in size in response to treatment with high-dose steroids.3, 5-9 To date, IgG4 related pseudotumors have not been described in the heart. The classical histopathologic findings of IgG4 disease include fibrosis, especially storiform fibrosis, rich lymphoplasmacytic infiltrates, venulitis or obliterative phlebitis, and IgG4/IgG ratio >50%. However, in the histopathologic findings, minor variability has been observed between the different target organ sites that can be affected by IgG4 disease.10
The heart is not a known IgG4 target organ.11 In fact, it would be a novel site. So in addition to the histopathology, it is important to look for other tell-tale clinical characteristics of IgG4-related disease, including: (1) a propensity for disease extension; (2) elevated serum IgG4 concentrations; (3) systemic inflammatory symptoms; and (4) a powerful initial response to glucocorticoids.10 The present case report displayed many of the characteristics for IgG4 disease, but since the heart is a novel site, the authors agree that this represents a probable case.
The patient continues on low-dose corticosteroids and cyclosporine. Although steroids produce a beneficial immune response to IgG4 pseudotumors, they do not induce disease remission. This patient has undergone 8 years of treatment with prednisone. Additional therapy with mycophenolate mofetil, azathioprine, methotrexate, or cyclophosphamide was not effective. The current combination of cyclosporine with prednisone has been tolerated and has kept the patient clinically stable. Rituximab has also been contemplated as an alternative treatment option for IgG4 disease and is being investigated in controlled clinical trials.12
Funding Statement
Funding/Support: Dr. Sessoms receives research funding from the Houston Methodist Hospital Foundation.
Footnotes
Conflict of Interest Disclosure: The authors have completed and submitted the Methodist DeBakey Cardiovascular Journal Conflict of Interest Statement and none were reported.
References
- 1.Moon JC, Sheppard MN, Lloyd G, Patel NR, Pennell DJ, Mohiaddin RH. Cardiac pseudotumor: tissue characterization by cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2003 Jul;5(3):497–500.. doi: 10.1081/jcmr-120022265. [DOI] [PubMed] [Google Scholar]
- 2.Narla LD, Newman B, Spottswood SS, Narla S, Kolli R. Inflammatory pseudotumor. Radiographics. 2003 May-Jun;23(3):719–29.. doi: 10.1148/rg.233025073. [DOI] [PubMed] [Google Scholar]
- 3.Miller DV, Tazelaar HD. Cardiovascular pseudoneoplasms. Arch Pathol Lab Med. 2010 Mar;134(3):362–8.. doi: 10.5858/134.3.362. [DOI] [PubMed] [Google Scholar]
- 4.Li L, Cerilli LA, Wick MR. Inflammatory pseudotumor (myofibroblastic tumor) of the heart. Ann Diagn Pathol. 2002 Apr;6(2):116–21.. doi: 10.1053/adpa.2002.32380. [DOI] [PubMed] [Google Scholar]
- 5.Ferbend P, Abramson LP, Backer CL, Mavroudis C, Webb CL, Doll JA, et al. Cardiac plasma cell granulomas: response to oral steroid treatment. Pediatr Cardiol. 2004 Jul-Aug;25(4):406–10.. doi: 10.1007/s00246-003-0269-x. [DOI] [PubMed] [Google Scholar]
- 6.Pearson PJ, Smithson WA, Driscoll DJ, Banks PM, Ehman RL. Inoperable plasma cell granuloma of the heart: spontaneous decrease in size during an 11-month period. Mayo Clin Proc. 1988 Oct;63(10):1022–5.. doi: 10.1016/s0025-6196(12)64918-0. [DOI] [PubMed] [Google Scholar]
- 7.Pucci A, Valori A, Muscio M, Garofalo L, Ferroni F, Abbruzzese PA. Asymptomatic inflammatory myofibroblastic tumor of the heart: immunohistochemical profile differential diagnosis, and review of the literature. Cardiovasc Pathol. 2009 May-Jun;18(3):187–90.. doi: 10.1016/j.carpath.2008.03.002. [DOI] [PubMed] [Google Scholar]
- 8.Su JW, Caleb MG, Tan RS, Low AF, Lim CH. Cardiac inflammatory myofibroblastic tumor as a rare cause of aortic regurgitation: a case report. J Thorac Cardiovasc Surg. 2006 Jul;132(1):150–1.. doi: 10.1016/j.jtcvs.2006.03.011. [DOI] [PubMed] [Google Scholar]
- 9.Tomiyama M, Nakatani S, Ishibashi-Ueda H, Yutani C, Yamagishi M. Inflammatory pseudotumor of the heart. Ann Intern Med. 2007 Sep 4;147(5):351–2.. doi: 10.7326/0003-4819-147-5-200709040-00023. [DOI] [PubMed] [Google Scholar]
- 10.Deshpande V, Zen Y, Chan JK, Yi EE, Sato Y, Yoshino T, et al. Consensus statement on the pathology of IgG4-related disease. International Symposium on IgG4-Related Disease; 2011 Oct 4-7; Massachusetts General Hospital, Boston, MA. [Google Scholar]
- 11.Khosroshahi A, Stone JH. A clinical overview of IgG4-related systemic disease. Curr Opin Rheumatol. 2011 Jan;23(1): 57–66.. doi: 10.1097/BOR.0b013e3283418057. [DOI] [PubMed] [Google Scholar]
- 12.Khosroshahi A, Carruthers MN, Deshpande V, Unizony S, Bloch DB, Stone JH. Rituximab for the treatment of IgG4-related disease: lessons from 10 consecutive patients. Medicine (Baltimore). 2012 Jan;91(1):57–66.. doi: 10.1097/MD.0b013e3182431ef6. [DOI] [PubMed] [Google Scholar]