

Abstract
The fracture of tibial tuberosity is a rare lesion and still more unusual in adults. We describe a case in an adult who suffered a left knee injury due to a fall from height. No risk factors were identified. The lesion was treated with surgical reduction and internal fixation. The rehabilitation method was successful, resulting in excellent function and rage of motion of the knee. The aim of this study was to present an unusual case of direct trauma of the tibial tuberosity in an adult and the therapy performed.
Background
Fractures of the tibial tuberosity are rare, taking only 3% of the proximal tibial fractures.1 This traumatic lesion is typical of the growth age, when muscles, tendons and ligaments are stronger than the growth plate. The mechanism of the trauma usually is the avulsion of the tubercle for the eccentric contraction of the thigh. The classification systems, treatments, follow-up and complications are all described in the literature for immature bones.
This type of fracture in an adult is an exceptional occurrence.2 The mechanism of trauma was unusual and we had to adapt and design a specific follow-up protocol for the patient. The purpose of this study is to present a rare case of a fracture of the tibial anterior tubercle in an adult and the results of the operative treatment.
Case presentation
A healthy man aged 62 years with direct trauma to the left knee after a fall was admitted to the emergency department of our hospital. He reported pain and inability to walk and extend the knee. The physical examination presented haemarthrosis, swelling and a gap in the insertion of the patellar tendon. At the time of the trauma the patient weighted 82 kg and was 1.70 m height. A radiographic examination showed the fracture of the tibial tuberosity (figure 1).
Figure 1.
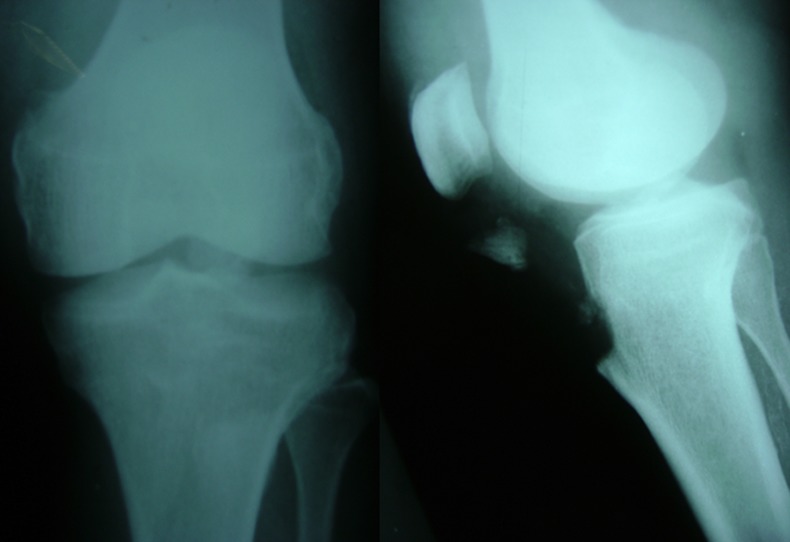
X-rays in anteroposterior and lateral views of the left knee showing the tibial anterior tuberosity fracture.
Investigations
We searched the medical history and blood tests performed with all markers for arthritis and kidney diseases discarding any relationship with any systemic disease or steroid use. Osgood-Schlatter's disease was also ruled out, as well as any previous surgery on this knee.
Treatment
The surgery took place 1 day after admission with the use of a tourniquet and a straight anterior incision (figure 2). We performed an open reduction and internal fixation with a 6.5 mm cannulated screw. The osteosynthesis was tested by careful bending of the joint.
Figure 2.
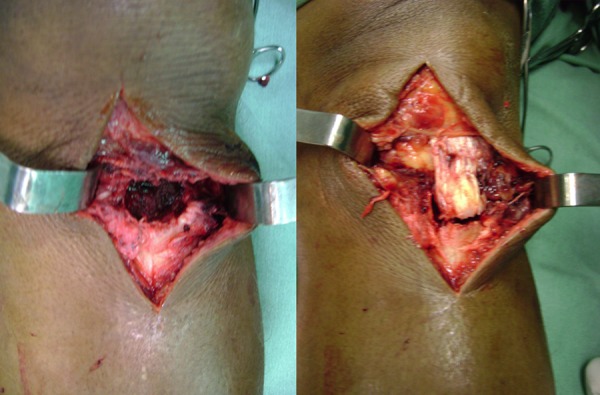
Images of the knee during the surgery, showing the gap in the tibial tubercle by the fracture and the reinsertion position.
Postoperatively, the knee was immobilised with a long brace for 6 weeks it was removed for active rehabilitation exercises to avoid atrophy of the quadriceps. The programme consisted of isometric exercise during the immobilisation and active exercises with progressive increase in range of motion. The full range of motion and overall knee function were obtained in 5 months.
The patient was evaluated at 7, 15, 30, 45 days and 2 months and so monthly until the sixth month, and quarterly thereafter. Our follow-up with this patient is 2 years and he came back with his usual activities being accompanied with a radiographic control (figure 3). In evaluating knee function we use the modified Lysholm score system.3 We obtained an average of 94 points in the left knee, which is considered an excellent score according to the same evaluation system (figures 4 and 5).
Figure 3.
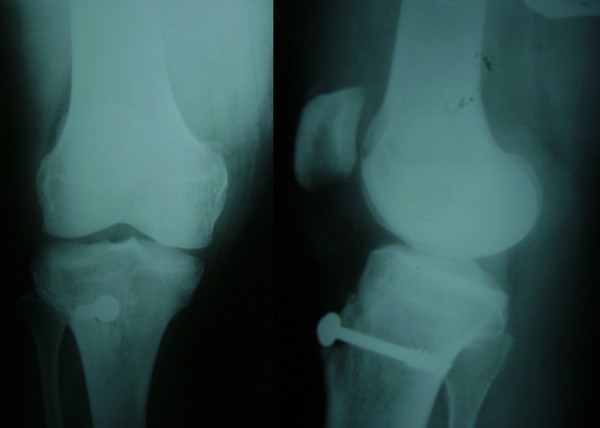
X-rays of the knee in anteroposterior and lateral views after the osteosynthesis.
Figure 4.

Images of the inferior limb demonstrating the functional assessment after the treatment.
Discussion
Regarding gender, the literature shows a predominance of men4 due to more frequent involvement in sports practicing during adolescence. The usual mechanism of avulsion of the tibial tuberosity is a sudden contraction of the quadriceps during knee extension or passive flexion of the knee against rapid contraction of the quadriceps.5 It happens on jumping or stabilising the knee in flexion.6 However, the direct trauma to the knee due to a fall from height could produce the fracture as shown. Kang et al7 described another direct trauma to the knee resulting in a fracture of the tibial tubercle in a 84-year-old man.
There are studies that correlate the avulsion fracture of the tibial tuberosity with Osgood-Schlatter lesion as a predisposing factor,8 9 but this man denied prior symptoms in both knees, as well as surgery. Some studies correlate avulsion of the tibial tuberosity with associated injuries of the knee6 10–12 as meniscal tears, collateral ligaments ruptures, capsule avulsion and intra-articular fractures, but we also could not find any on the clinical examination. The fracture of the tibial tuberosity in adults is usually due to a complication of anterior cruciate ligament reconstruction with autologous patellar tendon graft.13 There are reports of osteogenesis imperfecta as a predisposing factor for this lesion in children.14 Extensor knee mechanism injuries are associated to systemic disorders such as chronic steroid use, chronic renal failure, arthritis and lupus erythematosus.15 In this case we have a man without previous surgery, and without predisposing factors to injury.
Roentgenographic studies of the knee are reasonably accurate in the diagnostic confirmation, besides being a low-cost examination.1 In our opinion, when there is a trauma knee, radiography should always be the first imaging test to be requested, but fractures extended to the joint and fragmented should be evaluated with CT.6 11 When soft tissue-associated injuries are suspected, MRI can also help the diagnostic.16
All existing classifications of fractures of the tibial tuberosity are related to the growth phase and the presence of the physis. Watson-Jones and Ogden described classification systems for immature skeletons.9 For this reason, we did not use any specific classification of fractures of the tibial tuberosity. We used the classification of disruption of the extensor mechanism of the knee. This classification is subdivided into: rupture of the quadriceps tendon, patellar fracture, patellar ligament rupture and fracture of the tibial tuberosity.17
There is controversy between keeping the knee immobilised or not and the postoperative immobilisation period.18 We must remember that this type of injury usually affects children and adolescents. In the immature skeleton, there is a lower risk of joint stiffness when compared with adults. Therefore, we prefer the use of a brace for 6 weeks, with removal of daily exercises to gain range of motion and muscle development, avoiding stiffness.
The prognosis of tibial tubercle fractures is generally good after surgical treatments, but rerupture and stiffness must be careful handle postoperatively in adults. Theoretically genu recurvatum is an expected complication in open physis individuals after tibial tuberosity fractures, but only one case has ever been reported in an 11-year-old boy.19
In our opinion the diagnosis of the injury and early repair are the main goals of the treatment in order to obtain a better functional outcome. This method resulted in an excellent function according to the modified Lysholm score system in 2 years of follow-up.
Learning points.
Direct trauma and the adult age are not commonly related to tibial tubercle fractures, but it can happen.
Careful physical examination is essential for suspecting uncommon lesions.
Recognise-associated knee lesions and search for predisposing factors is important to define the treatment.
Open reduction and internal fixation is the goal for preserving the extensor mechanism of the knee after tibial tuberosity fractures.
When treating adults, the stiffness after surgery must be taken care of, but also, in order to prevent postoperative ruptures, a full range of motion should not be allowed too early.
Acknowledgments
The authors are thankful for the staff of the Miguel Couto Municipal Hospital, especially for the members of the Professor Nova Monteiro Orthopedics and Traumatology Service, where this work was performed.
Footnotes
Contributors: RPA examined the patient and performed the surgery. ASC followed-up, the case and collected the images. GCSA organised the bibliographic review and discussion. VSG reviewed the work and text. All the authors took part in the text writing.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.McKoy BE, Stanitski CL. Acute tibial tubercle avulsion fractures. Orthop Clin North Am 2003;34:397–403 [DOI] [PubMed] [Google Scholar]
- 2.Vella D, Peretti G, Fra F. One case of fracture of the tibial tuberosity in the adult. Chir Organi Mov 1992;77:299–301 [PubMed] [Google Scholar]
- 3.Tegner Y, Lysholm J. Rating systems in the evaluation of knee ligament injuries. Clin Orthop Relat Res 1985(198):43–9 [PubMed] [Google Scholar]
- 4.Júnior LHdC, Benevides WA, Nogueira FCS, et al. Fraturas da tuberosidade tibial anterior em adolescentes: relato de casos e revisäo da literatura. Rev Bras Ortop 1995;30:87–90 [Google Scholar]
- 5.Mosier SM, Stanitski CL. Acute tibial tubercle avulsion fractures. J Pediatr Orthoped 2004;24:181–4 [DOI] [PubMed] [Google Scholar]
- 6.Howarth WR, Gottschalk HP, Hosalkar HS. Tibial tubercle fractures in children with intra-articular involvement: surgical tips for technical ease. J Child Orthop 2011;5:465–70 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kang S, Chung PH, Kim YS, et al. Bifocal disruption of the knee extensor mechanism: a case report and literature review. Arch Orthop Trauma Surg 2013;133:517–21 [DOI] [PubMed] [Google Scholar]
- 8.Arredondo-Gomez E, Lopez Hernandez JD, Chavez Martinez F. [Fracture due to bilateral avulsion of the tuberosity of the shin bone (tibia). A case report]. Acta Ortop Mex 2007;21:154–8 [PubMed] [Google Scholar]
- 9.Roy SP, Nag K. Simultaneous bilateral tibial tuberosity avulsion fractures in adolescence: case report and review of 60 years of literature. Injury 2013;44:1953–5 [DOI] [PubMed] [Google Scholar]
- 10.McKoy BE, Stanitski CL, Hartsock LA. Bilateral tibial tubercle avulsion fractures with unilateral recurrence. Orthopedics 2006;29:731–3 [DOI] [PubMed] [Google Scholar]
- 11.Yoo JH, Kim KI, Yoon KH. A case of anterior cruciate ligament tear accompanied by avulsion fractures of tibial tuberosity and Gerdy's tubercle. Knee 2011;18:505–8 [DOI] [PubMed] [Google Scholar]
- 12.Jalgaonkar AA, Dachepalli S, Al-Wattar Z, et al. Atypical tibial tuberosity fracture in an adolescent. Orthopedics 2011;34:215. [DOI] [PubMed] [Google Scholar]
- 13.Júnior LHdC, Martins LH. Fratura da tuberosidade tibial anterior após reconstrução do ligamento cruzado anterior com terço central do tendão patelar: relato de caso. Rev Bras Ortop 2002;37:151–2 [Google Scholar]
- 14.Tamborlane JW, Lin DY, Denton JR. Osteogenesis imperfecta presenting as simultaneous bilateral tibial tubercle avulsion fractures in a child: a case report. J Pediatr Orthop 2004;24:620–2 [DOI] [PubMed] [Google Scholar]
- 15.Lu HD, Cai DZ, Wang K, et al. Simultaneous bilateral patellar tendon rupture without predisposing systemic disease or steroid use: a case report. Chin J Traumatol 2012;15:54–8 [PubMed] [Google Scholar]
- 16.Yee PK, Poon KC, Chiu SY. Simultaneous bilateral patellar tendon avulsion in an adolescent. Hong Kong Med 2012;18:530–2 [PubMed] [Google Scholar]
- 17.Newberg A, Wales L. Radiographic diagnosis of quadriceps tendon rupture. Radiology 1977;125:367–71 [DOI] [PubMed] [Google Scholar]
- 18.Ergun M, Taskiran E, Ozgurbuz C. Simultaneous bilateral tibial tubercle avulsion fracture in a basketball player. Knee Surg Sports Traumatol Arthrosc 2003;11:163–6 [DOI] [PubMed] [Google Scholar]
- 19.Nathan ST, Parikh SN. Genu recurvatum after tibial tuberosity fracture. Case Rep Orthop 2013;2013:952978. [DOI] [PMC free article] [PubMed] [Google Scholar]