

Abstract
Essex-Lopresti injuries are rare and present a clinical challenge. Incomplete diagnosis and treatment can lead to long-term instability, pain and functional impairment. We report on a clinical case of proximal radioulnar joint (PRUJ) and distal radioulnar joint (DRUJ) dislocation with unusual distal radial displacement and associated radial head shear fracture. The case was managed with closed reduction of the PRUJ and DRUJ followed by open reduction and fixation of the radial head. A high index of suspicion with thorough examination of the elbow, forearm and wrist and comprehensive imaging was important in reaching a complete diagnosis for appropriate treatment. Anatomical reduction of the PRUJ and DRUJ is essential to achieve optimal functional outcomes. Six months following the injury the patient made a satisfactory recovery with full range of movement; however, she continued to have mild to moderate general and moderate work-related disability.
Background
Forearm fractures associated with either a distal radioulnar disruption (DRUJ) or radial head disruption are classically described as Galeazzi and Monteggia fractures respectively. Galeazzi and Monteggia fractures represent 3–6% and 1–2% of forearm fractures, respectively.1 A rarer forearm injury is the Essex-Lopresti injury which consists of a fracture of the radial head, rupture of the interosseous membrane and proximal disruption of the DRUJ.2 We report on the diagnostic and treatment challenge of a simultaneous proximal radioulnar joint (PRUJ) and DRUJ dislocation with associated intra-articular radial head fracture and unusual distal and ulnar displacement of the radial head.
Case presentation
A 26-year-old female student fell awkwardly forward onto her forearm and elbow during an obstacle course. She was unable to recall the exact position of her limb on impact. She reported immediate swelling and pain to her elbow and wrist. She was otherwise fit and healthy with no other medical history. On examination, there was considerable swelling and tenderness of the elbow, forearm and ulnar side of the wrist. There was no skin or neurovascular compromise.
Investigations
Initial lateral radiographs showed a fracture dislocation of the radial head. The radial head was dislocated distally in relation to the capitellum with a comminuted fracture of its posterior aspect (figure 1). There was mild widening of the DRUJ with significant ulnar negative variance (figure 2B).
Figure 1.
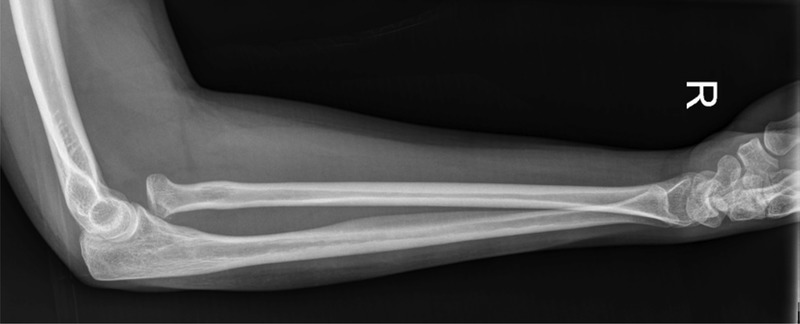
Lateral forearm X-ray.
Figure 2.

Anteroposterior elbow (A) and wrist (B) X-rays.
A CT scan was subsequently undertaken which showed a comminuted fracture of the radial head with displaced fracture fragments. The PRUJ was dislocated with the radial head displaced distally, anteriorly and ulnarly in relation to the articulating surface of the ulnar notch.
The radiographs and CT were in keeping with the DRUJ and PRUJ dislocation suggestive of a complete disruption of the interosseous membrane and radioulnar ligaments with the unusual feature of distal displacement of the radius with negative ulnar variance.
The final position of the ulna and radius was in supination (figures 2A and 3). There was also a small avulsion fracture noted on the posterolateral aspect of the capitellum. There was no evidence of an impaction on the capitellum and no fracture of the ulna and the elbow joint was concentrically enlocated (figure 3).
Figure 3.

CT forearm with reconstructed views.
Treatment
Closed reduction of the DRUJ was achieved by pronating the forearm and manipulating the radius laterally. Fluoroscopy comparison with the contralateral wrist confirmed the PRUJ and DRUJ reduction. A Kocher approach was then used to address the fracture of the radial head. Two smart nails (1.5 mm, Conmed Linvatec) were used to achieve a near anatomic internal fixation. The DRUJ and elbow joint were then assessed for stability. The lateral collateral ligament, which was partially taken off the humerus during the approach, was repaired with a bioabsorbable anchor and the common extensor origin was repaired.
A sling was used for comfort for 2 weeks postoperatively with physiotherapy and range of motion exercises initiated early.
Outcome and follow-up
The patient was followed up clinically, with functional scores and further imaging. At 6 months full wrist and elbow flexion and extension and full pronation and supination were achieved (figures 4A–C). The patient made a good recovery in regard to pain and mobility. She was able to return to her studies, however was unable to participate in contact sports. The disabilities of the arm, shoulder and hand index 6-month postinjury showed a disability/symptom score of 44 and work module score of 56. The sports module score was not applicable at the 6-month follow-up given the postoperative restrictions. Follow-up radiographs of her elbow at 3 months showed union of her radial head fracture and no adverse features (figure 5A). A follow-up MRI at 5-month postinjury demonstrated a reduced DRUJ with no triangular fibrocartilage complex injury (figure 5B).
Figure 4.

(A) Wrist flexion and extension, (B) elbow flexion and extension, and (C) forearm supination and pronation.
Figure 5.

Postoperative (A) elbow anteroposterior and lateral X-rays and (B) T2-weighted MRI of wrist and triangular fibrocartilage complex.
Discussion
Forearm injuries are commonly the result of a fall on an outstretched hand with a longitudinal force transmitted through the wrist in combination with a rotational force. A Galeazzi injury is typically a result of a fall on an outstretched hand with extreme forearm pronation and a Monteggia fracture is also thought to be due to excessive forced pronation.1 3 4 An Essex-Lopresti fracture is a complex injury in which a longitudinal force is transmitted via the wrist to the radial head and if there is sufficient force, a continuum of injuries occurs.5 The fractured radial head dislocates, after which the interosseous membrane ruptures, the DRUJ dislocates and the radius migrates proximally.2 During an axial load the rotational position of the forearm appears to influence the type of injury, with pronation a common cause.6 The mechanism of injury in our case appears to have been different to those described above and is likely due to an impact onto a supinated forearm with simultaneous posterior to anterior impact on the radial head, subsequently resulting in radial head dislocation, rupture of the interosseous membrane and DRUJ distraction. The radial head was ‘oversupinated’ with medial and distal displacement out of the ulnar notch. This is best appreciated on CT (figure 3). The avulsion fractures of the radial head are most likely to have occurred during medial and distal shear forces. Impact of the radial head with the capitellum humeri as in the usual Essex-Lopresti fracture dislocation is unlikely. The points of interest in this case are the unique mechanism of injury with the relation of the radius and the ulna distraction and the challenge of appropriate diagnosis and treatment.
Often in Essex-Lopresti type injuries, attention is focused on the more obvious injury at the head of the radius and as a consequence the distal radioulnar displacement is overlooked at initial examination.7 If distal radioulnar instability is not adequately appreciated and managed then chronic wrist symptoms, such as pain and instability, can develop.6 8 9 Distal arm pain should not simply be dismissed as referred pain.10 As such, a detailed examination and radiographs of the elbow, forearm and wrist should be conducted when Essex-Lopresti injuries are suspected.6 If plain radiographs are inadequate or there is diagnostic uncertainty, further imaging with MRI and CT are important.5
One of the primary goals of management in this type of injury is the preservation of PRUJ and DRUJ reduction. This is essential as impairment of reduction can result in loss of forearm rotation, grip strength and function.11 In addition to this, maintenance of appropriate length relationships of the radius and the ulna are essential for load bearing and sharing.10 Stability of both the PRUJ and DRUJ should be directly verified under fluoroscopy and further addressed if indicated.12
Learning points.
Accurate diagnosis of simultaneous proximal radioulnar joint (PRUJ) and distal radioulnar joint (DRUJ) injury remains challenging.
Missed diagnosis can lead to persistent wrist pain and instability.
A thorough examination should raise clinical suspicion.
Inconclusive radiographs should be followed by CT scan and/or MRI.
Anatomic reduction of both the PRUJ and DRUJ is essential in regaining function.
Footnotes
Contributors: All the authors contributed in the manuscript writing and figure design, composition, supervision and editing.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Clare DJ, Corley FG, MA W. Ipsilateral combination Monteggia and Galeazzi injuries in an adult patient: a case report. J Orthop Trauma 2002;2013:130–4 [DOI] [PubMed] [Google Scholar]
- 2.Jungbluth P, Frangen TM, Arens S, et al. The undiagnosed Essex-Lopresti injury. J Bone Joint Surg Br 2006;2013:1629–33 [DOI] [PubMed] [Google Scholar]
- 3.Ramisetty NM, Revell M, Porter KM. Galeazzi fractures in adults. Trauma 2004;2013:23–8 [Google Scholar]
- 4.Ramisetty NM, Revell M, Porter KM, et al. Monteggia fractures in adults. Trauma 2004;2013:13–21 [Google Scholar]
- 5.Cheung EV, Yao J. Monteggia fracture-dislocation associated with proximal and distal radioulnar joint instability. J Bone Joint Surg Am 2009;2013:950–4 [DOI] [PubMed] [Google Scholar]
- 6.Rodriguez-Martin J, Pretell-Mazzini J, Vidal-Bujanda C. Usual pattern of Essex-Lopresti injury with negative plain radiographs of the wrist: a case report and literature review. Hand Surg 2010;2013:41–5 [DOI] [PubMed] [Google Scholar]
- 7.Malik AK, Pettit P, Compson J. Distal radioulnar joint dislocation in association with elbow injuries. Injury 2004;2013:324–9 [DOI] [PubMed] [Google Scholar]
- 8.Edwards GS, Jupiter JB. Radial head fractures with acute distal radioulnar dislocation. Essex-Lopresti revisited. Clin Orthop Relat Res 1988;2013:61–9 [PubMed] [Google Scholar]
- 9.Hey HW, Chong AKS, Peng LP. Atypical Essex-Lopresti injury of the forearm: a case report. J Orthop Surg (Hong Kong) 2011;2013:373–5 [DOI] [PubMed] [Google Scholar]
- 10.Sabo MT, Watts AC. Longitudinal instability of the forearm: anatomy, biomechanics, and treatment considerations. Shoulder Elbow 2012;2013:119–26 [Google Scholar]
- 11.LaStayo PC, Lee MJ. The forearm complex: anatomy, biomechanics and clinical considerations. J Hand Ther 2006;2013:137–45 [DOI] [PubMed] [Google Scholar]
- 12.Giannicola G, Sacchetti FM, Greco A, et al. Management of complex elbow instability. Musculoskelet Surg 2010;2013(Suppl 1):S25–36 [DOI] [PubMed] [Google Scholar]