

Abstract
Purpose: To investigate postoperative pain control and analgesic use after heart surgery. Methods: 20 patients undergone heart surgery, randomly entered the study. Each patient was asked to score his pain intensity on visual analog scale (VAS) at four different occasions. Results: 120 patients aged 59 year-old; including 81 male were enrolled in the study. 69.2% had coronary artery disease and 16.7% had heart-valve problem. Main types of surgeries were coronary artery bypass surgery (70.5%) and valve repairement (23%). Duration of ICU stay was 4.78±2.7 days and duration of intubations was 17.38 ± 36.46 hours. Pre-surgery pain relief was administrated to 42% of the subjects and morphine and promethazine was the main pre-surgery analgesia medication. Post surgery analgesic included morphine (injection), petidine (injection) and NSAIDS (oral or rectal). According to VAS, mean pain level, 1 and 4 hours after extubation, and before and one hour after transferring to wards was 5.05±2.5, 4.09±2.0, 3.52±1.8, 2.36±1.89, respectively. Although the level of pain reported was mostly moderate, 80% were reported satisfaction with their post-surgery pain management. Conclusion: A closer pain management control is needed for patients after heart surgery. Introduction of newer pain management techniques, medications and dosages could reduce the pain and suffering.
Keywords: Postoperative Pain, Visual Analog Pain Scale, Pain Assessment, heart surgery
Introduction
Pain is defined as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms such damage” by the Task Force on Taxonomy of the International Association for the Study of Pain.1 Pain is an integral part of life and as such, attempts to relieve pain must be as old as mankind.2 Post operative pain is one of the consequences of surgeries and the fear of such pain is one of the main concerns of many patients who undergo surgery. This is a well justified fear and post-operative pain has been accepted as foreseeable part of post surgery experience by patients, and even when unrelieved pain is reported, it may not result in corrective measures or many patients may not receive adequate postoperative pain relief because of staff failures to routinely assess pain and prescribed pain relief and physicians are not held accountable for poor analgesia.3 Another factor in inadequate pain relief is the fear of the possibility of development of physical dependence, tolerance, addiction, and side effects which could prevent physicians from prescribing analgesic especially opioid ones. Inadequate pain relief is specially through in children.4
The first description for postoperative opium was by the Glasgow–born London surgeon James Moore (1749–1806) in 1784. He clearly realized opium postoperative benefits when he wrote “Opium … is highly expedient to abate the smarting of the wound after the operation is over, and to induce sleep; but the stronger dose we dare venture to give has little or no effect in mitigating the suffering of the patient during the operation”2. Over the past two centuries, opium and its derivatives have emerged as the most effective analgesics for postoperative pain relief.2 Nowadays, a variety of opioid and non-opioid-based analgesic modalities are available. The World Federation of Societies of Anesthesiologists (WFSA) Analgesic Ladder has been developed to treat acute pain.5
According to this ladder, immediately after an operation, the pain can be expected to be severe and may need controlling with strong parenteral opioids in combination with local anesthetic blocks and peripherally acting drugs. Normally, postoperative pain should decrease with time and the need for drugs to be given by injection should cease. There is then a step down to oral opioids and finally to non-steroidal anti-inflammatory drugs and acetaminophen on its own.6 As the experience of pain varies between patients and opioid effects vary between individuals, so the dosage of opioids need to be assessed for each individual in order to achieve adequate pain control. Analgesics or compounds with less pronounced dependency or tolerance should be used, if possible, and finally, analgesic therapy and the patient’s need for opioid should be evaluated frequently.
Despite of various protocols and medications and methods for post-operation pain relief, many patients still suffer from pain. The aim of the present study was to examine the level of post-cardiac surgery pain control in Iran.
Materials and Methods
Data collection was conducted between December 2007 and July 2008. Our data collected from 120 subjects of Shahid Madani Hospital in Tabriz, East Azerbaijan. This hospital is a cardiac specialist hospital, and serves a population of patients mixed from urban, semi rural and rural areas from East Azerbaijan and neighbor provinces.
Prior to cardiac surgery, patients who were going to undergo cardiac surgery were invited to take part in the study. Patients were informed about the study and the method of pain assessment prior to cardiac surgery. Sufficient time to make an informed discussion or consult with patient’s relatives or physician was given to each participant. After surgery, when patients were transformed to Intensive Care Units (ICU), the level of their pain was asked using a Visual Analog Scale (VAS, 0-10 cm) after 1 (assessment 1) and 4 (assessment 2) hours after extubation, and before (assessment 3) and one hour (assessment 4) after transferring to normal wards. Patients' demographic information, history of illnesses, pre and post surgery analgesics and their doses were extracted from patients' records, and patient satisfaction regarding the pain control was asked from the patients.
Permission for the study was obtained from the Regional Medical Research Ethic Committee, Tabriz University of Medical Sciences, with code number of 8521 and all patients included in the study signed informed consent. Data were analyzed using the SPSS software 13.5. Paired Student’s t-tests were performed to examine the differences between variables and Pearson's correlation coefficient was used for examining the possible relationship between various factors. All tests were conducted at the P<0.05 level of significance.
Results
One hundred and twenty randomly chosen patients who undergone heart surgery in Tabriz entered the study and completed questioner. The subjects aged 16 to 82 years old, and with median age of 59 (± 14.0) years including 81 male and 39 female patients. 27% of patients had no educational background and 12% had university education. Most of the subjects were from East Azerbaijan (57%) while others were from neighbor provinces such as West Azerbaijan (30%), Ardebil (15%) and Kurdistan (7%).
Main type of surgery was Coronary artery bypass surgery (CABS; 70.5%) and valve repairement (23%). 28.3% had illnesses other than their current heart problem with diabetes as the highest one (67.7%) (Table 1). 42% of the patients reported taking analgesic as the pain relief of their concurrent disease which included acetaminophen codeine (57.8%), acetaminophen (19.1%), ibuprofen (11.9%) and opium (2.4%). 28.6% reported taking these analgesia medication as required (PRN) and 7.1% reported taking analgesic only once a day. 29 subjects reported taking anti-anxiety medication prior to their hospital admission which included oxazepam (16 subjects), diazepam (10 subjects) and lorazepam, alperazom, clonazepam, trifloprazine, cholordiaspoxide. Duration of ICU stay was 4.78 ± 2.7 (mean ± SD) days ranging 2 to 16 days and duration of intubation was 17.38 ± 36.46 hours ranging 4 to 306 hours. Three patients passed away before extubation or moving to the wards. There was no correlation between duration of intubation and ICU stay (R2= 0.321).
Table 1. Characteristics of patients’ illnesses.
| Patients Heart illnesses (Number, %) |
Coronary artery (83,69.2%) |
Valve problem (20, 16.7%) |
Other (17,14.2%) |
| Surgery type (Number, %) |
CABG (75,62.5%) |
Valve repairment (15, 12.5%) |
Other (30,25.0%) |
| Co-morbid disease (Number, %) |
Yes (34,28.3%) |
No (86, 71.7%) |
_ |
Pre-surgery pain relief was mainly morphine (injection) and promethazine (injection or oral). Some patients received diazepam (32.4%), oxazepam (4.9%), midazolam (12.4%) petidine (2.5%), methadone (1.7%) or fentanyle (0.8%). Post surgery analgesic included morphine and/or petidine which accounted for 93.3% of the subjects. Smaller percentages received morphine (IV) with NSAIDS (oral or rectal) or NSAIDs alone.
According to VAS, the mean pain level after 1 and 4 hours after extubation, and before and one hour after transferring to wards was 5.05 (± 2.5), 4.09 (± 2.0), 3.52 (± 1.8), 2.36 (± 1.89), respectively (Figure 1). The used pain control medication for a pain score of 1 to 3 was acetaminophen and other NSAIDs, administrated orally or rectally. When the pain score was 4 to 6, the main medication was oral acetaminophen-codeine, and when pain scores increased to 7 or higher, the medication was intravenous or intramuscular morphine, petidine or methadone. At pain score of 1 to 6, analgesia medication was given at certain intervals according to the medication dose instruction and when it was required, while after pain score of 7, injection of strong opiates was given only when it was needed. Eighty percent of the patients reported satisfaction with their post-surgery pain management, while 3.3% reported unsatisfaction with the pain management.
Figure 1.
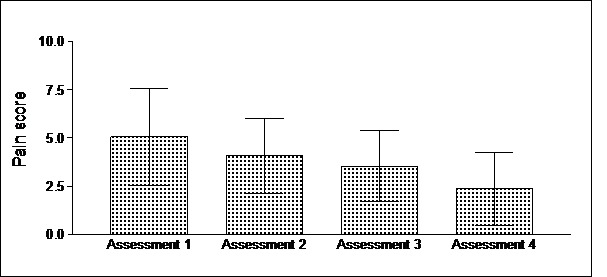
Pain assessment after 1h (assessment 1) and 4h (assessment 2) after extubation, and before (assessment 3) and one hour (assessment 4) after transferring to wards.
Discussion
Surgeries are extremely stressful events and post-operative pain control is one of the greatest concerns for both physicians and patients. Patients' postoperative experiences influence their existential aspects of lifelong after surgery.7 Surprisingly, few studies treated suffering from postoperative pain as a particular topic. This highlights the need for more qualitative research exploring specific postsurgical experiences such as postoperative pain. In the present study, we tried to examine the level of pain relief after heart surgery.
The highest pain score was observed 1 hour after extubation and highest level of analgesic prescription was given to prevent pain at this time; the pain level was reduced over time and reached its lowest level one hour after transferring to the wards. The differences between reported pain scores at different point were significant (Table 2). The analgesic medications were administrated according to World Federation of Societies of Anesthesiologists (WFSA) Analgesic Ladder; strong opioids for moderate to severe pain, NSAIDs or acetaminophen with weak opioids for moderate pain score and NSAIDs or acetaminophen for mild pain score. The analgesic administration method was an issue, because the pain relief was not provided at certain time intervals and given when a patient was in need of analgesia. This was less apparent in case of NSAIDs, acetaminophen or acetaminophen/codeine compounds and was more evident in case of strong opioids.
Table 2. Comparison of pain scores during 4 pain assessments [after 1h (assessment 1) and 4h (assessment 2) after extubation, and before (assessment 3) and one hour (assessment 4) after transferring to wards].
| Compared Pairs | P value |
| Assessment 1 - Assessment 2 | <0.001 |
| Assessment 1 - Assessment 3 | <0.001 |
| Assessment 1 - Assessment 4 | <0.001 |
| Assessment 2 - Assessment 3 | 0.006 |
| Assessment 2 - Assessment 4 | <0.001 |
| Assessment 3 - Assessment 4 | <0.001 |
It is possible that a varying misconception may deter professionals and patients from providing adequate pain relief. The fear of the possibility of development of physical dependence, tolerance, addiction, and side effects especially respiratory depression could prevent physicians from prescribing it and make patients anxious about its usage. It is certainly important to consider the risk of dependence when using these drugs therapeutically. Despite this risk, under no circumstances should adequate pain relief ever be withheld because an opioid exhibits the potential for abuse or because legislative controls complicate the process of prescribing narcotics. However, certain principles can be observed by the clinicians to minimise problems presented by tolerance and dependence when managing pain with opioid analgesics. Undertreated severe pain may have physiological consequences increasing the stress response to surgery, seen as a cascade of endocrine-metabolic and inflammatory events that ultimately may contribute to organ dysfunction, morbidity, increased hospital stay and mortality. The pain often causes the patient to remain immobile, thus becoming vulnerable to deep venous thrombosis, pulmonary atelectasis, muscle wasting and urinary retention. Besides, restlessness caused by severe pain may contribute to postoperative hypoxemia.8 The peripheral neural activation, together with central neuroplastic changes, associated with postoperative pain may in some patients continue into a chronic pain state.9
The experience of pain varies between patients and various factors causes opioid effects to vary between individuals,10-13 therefore the dosage of morphine and other opioids need to be assessed for each individual in order to achieve adequate pain control. Some even suggest pain assessment as fifth vital sign. Analgesics or compounds with less pronounced dependency or tolerance should be used, if possible, and finally, analgesic therapy and the patient’s need for opioid should be evaluated frequently.
Another problem was the lack of oral opioid formulation in Iran, specially the strong opioids. This is less problematic in the present study because of the nature of pain after surgery and unreliable oral medication absorbance after surgeries, but it is an important issue in case of pain management in chronic pain such as one seen in cancer patients.
There are methods, that could reduce pain level in post-operative patients and therefore reduce the amount of needed opioids, such examples are intra-operative magnesium sulfate administration,14-18 sub-anesthetic dose of ketamine,19-25 lowering patient’s Pre-operative anxiety26-28 and music.29,30
Despite the facts that the experienced pain was mostly moderate, still patients reported satisfaction from their pain management. This could be the result of the belief that pain is an inevitable part of post-surgery experience.
In summary, prescription patterns for post operative pain relief have not changed to include many of the new methods presently available such as patients control analgesia (PCA). Only one or two routes of administration are still used for a limited range of opioid and non-opioid drugs. Patients still experience a high incidence of mild to moderate to even unbearable pain in the post operative period. This can be improved by prescribing drugs at shorter intervals to reflect their pharmacokinetics and using newer techniques of drug administration.
Conflict of Interest
The authors report no conflicts of interest.
References
- 1.Crombie I. Epidermiology of persistent pain. In: Jensen T, Turner J, Wiesenfeld-Hallin Z, editors. Proceeding of the 8th World congress on pain. Seattle: IASP pree; 1997.
- 2.Hamilton GR, Baskett TF. In the arms of Morpheus the development of morphine for postoperative pain relief. Can J Anaesth . 2000;47(4):367–74. doi: 10.1007/BF03020955. [DOI] [PubMed] [Google Scholar]
- 3.Rawal N. Postoperative pain relief using regional anaesthesia. Curr Anaesth Crit Care . 2007;18(3):140–8. [Google Scholar]
- 4.Mashayekhi SO, Ghandforoush-Sattari M, Routledge PA, Hain RD. Pharmacokinetic and pharmacodynamic study of morphine and morphine 6-glucuronide after oral and intravenous administration of morphine in children with cancer. Biopharm Drug Dispos. 2009;30(3):99–106. doi: 10.1002/bdd.649. [DOI] [PubMed] [Google Scholar]
- 5.World Health Organization. Essential medicines: WHO model list. 14th ed. 2005. Available from: http://whqlibdoc.who.int/hq/2005/a87017_eng.pdf.
- 6.Charlton E. The Management of Postoperative Pain. Update in Anaesthesia. World Anesthesia Online 1997(7):1-7. [Google Scholar]
- 7.Leegaard M, Fagermoen MS. Patients' key experiences after coronary artery bypass grafting: a synthesis of qualitative studies. Scand J Caring Sci . 2008;22(4):616–28. doi: 10.1111/j.1471-6712.2007.00556.x. [DOI] [PubMed] [Google Scholar]
- 8.Loach A. The management of postoperative pain. In: Orthopaedic anaesthesia. 2nd ed. Edward Arnold: London; 1994. p. 65.
- 9.Perkins FM, Kehlet H. Chronic pain as an outcome of surgeryA review of predictive factors. Anesthesiology. 2000;93:1123–33. doi: 10.1097/00000542-200010000-00038. [DOI] [PubMed] [Google Scholar]
- 10.Sattari M, Routledge P, Mashayekhi S. The influence of active transport systems on morphine -6-glucuronide transport in MDCKII and MDCK-PGP cells. Daru. 2011;19(6):412–6. [PMC free article] [PubMed] [Google Scholar]
- 11.Mashayekhi SO, Sattari MR, Routledge PA. Evidence of active transport involvement in morphine transport via MDCKII and MDCK-PGP cell lines. Res Pharm Sci . 2010;5(2):99–106. [PMC free article] [PubMed] [Google Scholar]
- 12.Mashayekhi SO, Ghandforoush-Sattari M, Buss DC, Routledge PA, Hain RD. Impact of anti-cancer drugs and other determinants on serum protein binding of morphine 6-glucuronide. Daru . 2010;18(2):107–13. [PMC free article] [PubMed] [Google Scholar]
- 13.Mashayekhi SO, Hain RD, Buss DC, Routledge PA. Morphine in children with cancer: impact of age, chemotherapy and other factors on protein binding. J Pain Palliat Care Pharmacother . 2007;21(4):5–12. [PubMed] [Google Scholar]
- 14.Ferasatkish R, Dabbagh A, Alavi M, Mollasadeghi G, Hydarpur E, Moghadam AA. et al. Effect of magnesium sulfate on extubation time and acute pain in coronary artery bypass surgery. Acta Anaesthesiol Scand . 2008;52(10):1348–52. doi: 10.1111/j.1399-6576.2008.01783.x. [DOI] [PubMed] [Google Scholar]
- 15.Oguzhan N, Gunday I, Turan A. Effect of magnesium sulfate infusion on sevoflurane consumption, hemodynamics, and perioperative opioid consumption in lumbar disc surgery. J opioid manag . 2008;4(2):105–10. doi: 10.5055/jom.2008.0015. [DOI] [PubMed] [Google Scholar]
- 16.Ozcan PE, Tugrul S, Senturk NM, Uludag E, Cakar N, Telci L. et al. Role of magnesium sulfate in postoperative pain management for patients undergoing thoracotomy. J Cardiothorac Vasc Anesth . 2007;21(6):827–31. doi: 10.1053/j.jvca.2006.11.013. [DOI] [PubMed] [Google Scholar]
- 17.Cizmeci P, Ozkose Z. Magnesium sulphate as an adjuvant to total intravenous anesthesia in septorhinoplasty: a randomized controlled study. Aesthetic Plast Surg . 2007;31(2):167–73. doi: 10.1007/s00266-006-0194-5. [DOI] [PubMed] [Google Scholar]
- 18.Bilir A, Gulec S, Erkan A, Ozcelik A. Epidural magnesium reduces postoperative analgesic requirement. Br J Anaesth . 2007;98(4):519–23. doi: 10.1093/bja/aem029. [DOI] [PubMed] [Google Scholar]
- 19.Nesher N, Ekstein MP, Paz Y, Marouani N, Chazan S, Weinbroum AA. Morphine with adjuvant ketamine vs higher dose of morphine alone for immediate postthoracotomy analgesia. Chest . 2009;136(1):245–52. doi: 10.1378/chest.08-0246. [DOI] [PubMed] [Google Scholar]
- 20.Moustafa AM, Negmi HH, Rabie ME. The combined effect of ketamine and remifentanil infusions as total intravenous anesthesia for scoliosis surgery in children. Middle East J Anesthesiol . 2008;19(5):1151–68. [PubMed] [Google Scholar]
- 21.Nesher N, Serovian I, Marouani N, Chazan S, Weinbroum AA. Ketamine spares morphine consumption after transthoracic lung and heart surgery without adverse hemodynamic effects. Pharmacol Res . 2008;58(1):38–44. doi: 10.1016/j.phrs.2008.06.003. [DOI] [PubMed] [Google Scholar]
- 22.Sim TB, Seet CM. To study the effectiveness and safety of ketamine and midazolam procedural sedation in the incision and drainage of abscesses in the adult emergency department. Eur J Emerg Med . 2008;15(3):169–72. doi: 10.1097/MEJ.0b013e3282efdd7a. [DOI] [PubMed] [Google Scholar]
- 23.Zhao Y, Guo QL, Zhang Z, Wang E, Xiong YC, Zou WY. [Three subanaesthetic dose ketamines mixed with butorphanol in the postoperative continuous intravenous analgesia] Zhong Nan Da Xue Xue Bao Yi Xue Ban . 2008;33(3):266–9. [PubMed] [Google Scholar]
- 24.Choudhuri AH, Dharmani P, Kumarl N, Prakash A. Comparison of caudal epidural bupivacaine with bupivacaine plus tramadol and bupivacaine plus ketamine for postoperative analgesia in children. Anaesth Intensive Care . 2008;36(2):174–9. doi: 10.1177/0310057X0803600206. [DOI] [PubMed] [Google Scholar]
- 25.Neuhauser C, Preiss V, Feurer MK, Muller M, Scholz S, Kwapisz M. et al. Comparison of S-(+)-ketamine- with sufentanil-based anaesthesia for elective coronary artery bypass graft surgery: effect on troponin T levels. Br J Anaesth. 2008;100(6):765–71. doi: 10.1093/bja/aen095. [DOI] [PubMed] [Google Scholar]
- 26.Woodhead J, Harding SA, Simmonds M, Dee S, Mcbride-Henry K. Premedication for cardiac catheterization and percutaneous coronary intervention: does it increase vascular access site complications? . J Cardiovasc Nurs. 2007;22(6):466–71. doi: 10.1097/01.JCN.0000297386.14002.f2. [DOI] [PubMed] [Google Scholar]
- 27.Seers K, Crichton N, Tutton L, Smith L, Saunders T. Effectiveness of relaxation for postoperative pain and anxiety: randomized controlled trial. J Adv Nurs. 2008;62(6):681–8. doi: 10.1111/j.1365-2648.2008.04642.x. [DOI] [PubMed] [Google Scholar]
- 28.Montin L, Leino-Kilpi H, Katajisto J, Lepisto J, Kettunen J, Suominen T. Anxiety and health-related quality of life of patients undergoing total hip arthroplasty for osteoarthritis. Chronic illness. 2007;3(3):219–27. doi: 10.1177/1742395307084405. [DOI] [PubMed] [Google Scholar]
- 29.Ebneshahidi A, Mohseni M. The effect of patient-selected music on early postoperative pain, anxiety, and hemodynamic profile in cesarean section surgery. J Altern Complement Med. 2008;14(7):827–31. doi: 10.1089/acm.2007.0752. [DOI] [PubMed] [Google Scholar]
- 30.Nilsson U, Unosson M, Rawal N. Stress reduction and analgesia in patients exposed to calming music postoperatively: a randomized controlled trial. Eur J Anaesthesiol. 2005;22(2):96–102. doi: 10.1017/s0265021505000189. [DOI] [PubMed] [Google Scholar]