

Abstract
Aspiration or ingestion of a foreign body has frequently been reported in the pediatric and in the adult population. Among many foreign bodies to be ingested, artificial denture is one to be impacted in the esophagus, especially among the elderly. Radiolucency of dental prosthesis complicates early diagnosis of an impacted or ingested dental prosthesis. Rigid and flexible esophagoscopes have been used to retrieve the foreign body from the esophagus but the need for open surgery to remove the foreign body as a rescue procedure to endoscopy or the primary procedure has not been well defined. Here we report a case of impacted foreign body esophagus which was managed primarily by surgery and another case where surgery was performed after trials of endoscopic approach had failed.
Keywords: Impacted foreign body, Esophagus, Esophagoscope, Surgery
Ingested foreign body in esophagus is a frequent occurrence and a very common otolaryngological emergency. The problem can occur in all age groups. The most frequently ingested foreign bodies in children are coins and alkaline batteries while in adults, they are meat and fish bones. In elderly patients, especially with dementia, impacted dental prosthesis in esophagus can create serious problems [1]. The majority of foreign bodies that reach the GI tract, true foreign objects and food bolus impactions, generally pass spontaneously. However, 10–20 % will require nonoperative intervention, and 1 % or less will require surgery [2]. Ingestion of a dental prosthesis can be a challenging problem requiring intervention, delay in which, can lead to significant morbidity and even mortality [3]. Most impacted dentures can be safely removed endoscopically employing specialized techniques of flexible or rigid endoscopy. The endoscopic retrieval however may, at times be impossible requiring transcervical Pharyngo-Esophagotomy. We hereby report two cases of impacted dentures where patients required open pharyngo-esophagotomy after failed endoscopic retrieval. The related literature is reviewed. We have also attempted to define indications of retrieval of dentures by external incisions.
Case 1
42 years old female presented to our OPD with complaints of dysphagia, odynophagia and hoarseness for 1 year. She had a chronic neck abscess that was drained elsewhere leading to a fistulous tract. Her endoscopy by gastroenterologist revealed a stricture in upper esophagus. Barium swallow showed a short segment (C6-T1) eccentric narrowing of cervical esophagus.
She also had history of use of ill fitting denture which she had misplaced but gave no definite history of ingestion or impaction of dentures. On examination there was ~2 cm × 3 cm irregular shaped purulent discharging sinus with friable edges on left paramedian area at the level of thyroid. Indirect Laryngoscope showed left vocal cord palsy. CT scan revealed soft tissue thickening extending into strap muscle, radio opaque attenuation in the esophagus and hypodense area in retropharyngeal space (Fig. 1).
Fig. 1.

Radio opaque attenuation in esophagus and hypodense area in retropharyngeal space at C6-T1 vertebral level with soft tissue thickening extending into strap muscles
The radio-opaque opacity aroused our suspicion of foreign body. Diagnostic Hypopharyngoscopy revealed a stricture just below cricopharynx. Hypopharyngoscope could not be passed beyond 15 cm from incisors. Cervical incision was hence made and retropharyngeal space was entered from left side and esophagotomy was done. Foreign body in its cervical part was palpated and removed (Fig. 2). The esophageal evaluation through the esophagotomy opening was normal and did not reveal a stricture. Post operative period was uneventful and oral feeds were resumed on day 8.
Fig. 2.
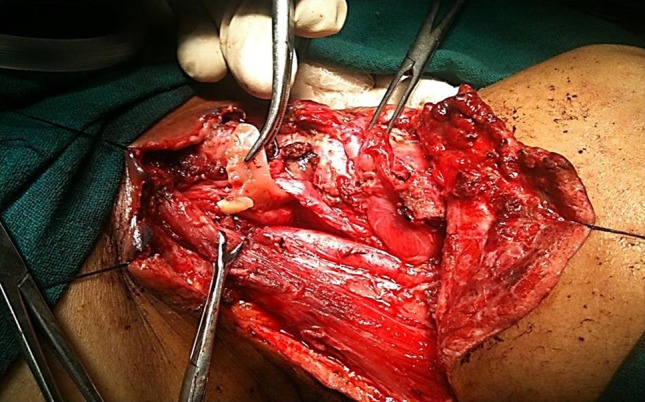
Intraoperative removal of foreign body via transcervical approach
Case 2
65 years male who accidentally ingested artificial denture presented with dysphagia & odynophagia for 2 days. Esophagoscopic removal was attempted elsewhere, but failed due to impaction in the esophageal wall. There was no respiratory distress/bleeding/chest pain/fever. There was pooling of saliva in bilateral pyriform sinuses in indirect laryngoscopy. X ray neck showed artificial denture at the level of C6 vertebra.
Esophagoscopic removal of foreign body was attempted. Only edge of foreign body was visible. Pin was not seen inside the lumen so it was abandoned and converted into transcervical approach. The pin was found to be protruding out of the esophageal wall. Esophagotomy was performed and foreign body was retrieved. Mucosa over cricopharynx and esophagus was closed in two layers (Fig. 3).
Fig. 3.

Wire protruding out from esophageal wall
Post operative course was uneventful. Barium swallow showed no leak. Oral feeds were resumed on day 7.
Discussion
Impaction of foreign body in esophagus is a common problem. It is most often an urgent medical situation. Dentures and meat bones are most commonly found impacted esophageal foreign bodies in adults [2]. Impaction occurs at physiological narrowing, angulations and strictures. Dental prosthesis may have metal clasps or retaining wires that predispose them to impaction when ingested [4].
The sharp foreign bodies may be buried deep in mucosal or muscular layer of esophagus causing mucosal edema leading to tracheal compression, mucosal ulceration, inflammation, infections like para or retropharyngeal abscess, mediastinitis, empyema, perforation, foreign body migration into adjacent structures like trachea or aorta, aortoesophageal fistula which may cause catastrophic bleeding [5, 6]. In the first case, the denture was embedded in the esophageal wall for 1 year complicating as deep neck space infection, fistula in neck, vocal cord palsy, hypopharyngeal and esophageal stricture mimicking as carcinoma esophagus. While in second case, the denture was only embedded in the esophageal wall without any complication.
Management of impacted foreign body depends upon type of dentures and its site of impaction. In 1937 Jackson and Jackson [7] described management of upper airway and esophageal foreign body with rigid endoscope. While in 1966, Bigler [8] introduced Foleys catheter as a new technique and in 1970s and 1980s, the flexible fiberoptic instrument was used as an additional option [9]. The success rate of rigid instrument ranges between 94 and 100 % while that of flexible esophagoscopy ranges between 76 and 98.5 %.The incidence of esophageal perforation with rigid endoscope is 0.34 % with a 0.05 % mortality rate while the morbidity (perforation) rate is between 0 and 0.5 % with flexible one [9, 10]. Use of Lower esophageal sphincter relaxants like benzodiazepines, calcium channel blockers and glucagon have been described but without much effect [11].
Considering high rates of successful removal of impacted foreign bodies, endoscopic retrieval almost always remains the preferred option of management. Some cases, like ones we have described, however, make the endoscopic removal impossible. Both the cases had the impacted denture in esophagus that had pierced the mucosal wall. In case 1, chronic impaction had also led to complications in form of proximal stricture and neck abscess. In case 2 also, the denture wires had pierced through esophageal walls and could be seen protruding extraluminally during exploration. In such cases of chronic impaction of foreign bodies or where sharp impaction has occurred and wires cannot be completely seen on rigid esophagoscopy, we recommend transcervical esophagotomy for their retrieval. The decision for open procedure is much safer in such cases than attempts to retrieve endoscopically that is fraught with complications. Various approaches can be cervicotomy, thoracotomy or gastrotomy according to its location. Esophageal perforation, if present, should be closed in two layers [12].
Conclusion
Denture impaction is frequently encountered esophageal foreign body. The treatment of choice is endoscopic removal but in cases where the wires pierce the lumen, open esophagotomy should be considered. The procedure is safe and effective.
References
- 1.Yadav R, Mahajan G, Mathur RM. Denture plate foreign body of esophagus. Ind J Thorac Cardiovasc Surg. 2008;24:191–194. doi: 10.1007/s12055-008-0040-2. [DOI] [Google Scholar]
- 2.Webb WA. Management of foreign bodies of the upper gastrointestinal tract: update. Gastrointest Endosc. 1995;41:39–51. doi: 10.1016/S0016-5107(95)70274-1. [DOI] [PubMed] [Google Scholar]
- 3.Stiles B, Wilson W. Denture esophageal impaction refractory to endoscopic removal in a psychiatric patient. J Emer Med. 2000;18:323–326. doi: 10.1016/S0736-4679(99)00222-X. [DOI] [PubMed] [Google Scholar]
- 4.Nimmo SS, Nimmo A, Chin GA. Ingestion of a unilateral removable partial denture causing serious complications. Oral Surg. 1988;66:24–26. doi: 10.1016/0030-4220(88)90060-6. [DOI] [PubMed] [Google Scholar]
- 5.Monnier P, Savary M (1997) Foreign bodies of the esophagus: a retrospective study in 1436 adults. In: Proceedings of the International Congress of Thorax Surgery, Monduzzi Editore, Bologna, pp 197–200
- 6.Byard RW. Esophageal causes of sudden and unexpected death. J For Sci. 2006;51:390–395. doi: 10.1111/j.1556-4029.2006.00068.x. [DOI] [PubMed] [Google Scholar]
- 7.Jackson C, Jackson CL. Disease of the air and food passages of foreign body origin. Philadelphia: W.B. Saunders; 1937. [Google Scholar]
- 8.Bigler FC. The use of a foley catheter for removal of blunt foreign bodies from the esophagus. J Thorac Cardiovasc Surg. 1966;51:759–760. [PubMed] [Google Scholar]
- 9.Brady PG. Endoscopic removal of foreign bodies. In: Silvis SE, editor. Therapeutic gastrointestinal endoscopy. New York: Igaku-Shoin; 1990. [Google Scholar]
- 10.Webb W. Management of foreign bodies of the upper gastrointestinal tract. Gastroenterology. 1988;94:204–216. doi: 10.1016/0016-5085(88)90632-4. [DOI] [PubMed] [Google Scholar]
- 11.Lyons MF, Tsuchida AM. Foreign bodies of the gastrointestinal tract. Med Clin North Am. 1993;77:1101–1114. doi: 10.1016/s0025-7125(16)30212-7. [DOI] [PubMed] [Google Scholar]
- 12.Athanassiadi K, Gerazounis M, Metaxas E, Kalantzi N. Management of esophageal foreign bodies: a retrospective review of 400 cases. Eur J Cardio-Thorac Surg. 2002;21:653–656. doi: 10.1016/S1010-7940(02)00032-5. [DOI] [PubMed] [Google Scholar]