

Abstract
Objectives
Understanding and effectively addressing persistent health disparities in minority communities requires a clear picture of members’ concerns and priorities. This study was intended to engage residents in urban and rural communities in order to identify environmental health priorities. Specific emphasis was placed on how the communities defined the term environment, their perceptions of environmental exposures as affecting their health, specific priorities in their communities, and differences in urban versus rural populations.
Study design
A community-engaged approach was used to develop and implement focus groups and compare environmental health priorities in urban versus rural communities.
Methods
A total of eight focus groups were conducted: four in rural and four in urban communities. Topics included defining the term environment, how the environment may affect health, and environmental priorities within their communities, using both open discussion and a predefined list. Data were analysed both qualitatively and quantitatively to identify patterns and trends.
Results
There were important areas of overlap in priorities between urban and rural communities; both emphasized the importance of the social environment and shared a concern over air pollution from industrial sources. In contrast, for urban focus groups, abandoned houses and their social and physical sequelae were a high priority while concerns about adequate sewer and water services and road maintenance were high priorities in rural communities.
Conclusions
This study was able to identify environmental health priorities in urban versus rural minority communities. In contrast to some previous risk perception research, the results of this study suggest prioritization of tangible, known risks in everyday life instead of rare, disaster-related events, even in communities that have recently experienced devastating damage from tornadoes. The findings can help inform future efforts to study, understand and effectively address environmental issues, and are particularly relevant to developing effective community-based strategies in vulnerable populations.
Keywords: Community-engaged approach, Rural versus urban communities, Minority populations, Community-based interventions, Risk perception
Introduction
Identifying environmental priorities at the community level is essential for understanding environmental health concerns, planning and implementing guided research and future interventions, and addressing the issues of greatest concern.1 However, this process may not always be simple in communities characterized by persistent health disparities and a historically-based lack of trust of health professionals.
Persistent health disparities exist in the US, particularly between races2 and across urban–rural gradients. There is an important distinction between disparities in health outcomes due to differential healthcare access versus disparities in health outcomes associated with other causes, such as differences in lifestyle or environmental factors. Access to and quality of medical care received are often highlighted as primary reasons for differences in health outcomes across urban–rural gradients.3 Rural residents tend to have fewer visits to healthcare providers and are less likely to receive recommended preventive services.4 Rural minorities can be particularly disadvantaged, with differences observed in cancer screening, management of cardiovascular disease and diabetes, and mental health.2 An analysis of birth outcomes in rural and urban Alabama shows significantly heightened preterm birth rates and low birth weight rates in African Americans and preterm birth rates and low birth rates are declining in suburban and urban areas, but not in isolated rural areas.5
Differences in the physical environments in urban and rural settings may affect health outcomes. Previous studies have linked aspects of the built environment, such as density of recreational facilities, to health disparities in obesity.6 Other studies have identified specific behaviours and activities that may contribute to differences in exposures to pesticides, water pollutants, and soil contamination.7 Proximity to industrial facilities may also influence health outcomes related to environmental exposures in urban and rural settings.8 In general, rural communities may experience more exposures due to agricultural, forestry, or mining practices9–12 while urban communities may experience more exposures due to traffic-related emissions, power generation, and industrial processes.13–15
Differences in the social environment may also play an important role in defining urban–rural differences in health.10 Inder et al. (2012) found that higher levels of perceived community improve the well-being of and are protective for psychological distress in older rural populations especially when overcoming isolating factors.16 Berkman and Syme (1979) found that social contacts including informal and formal groups associations had a protective effect against mortality in the 1965 Human Population Lab survey.17 McKinlay et al. (1989) prioritized social change over medical services based on their review of the effects of medical measures on morbidity and mortality.18 Particularly in the South, a historical context may be useful in understanding the social context of the significant health disparities that exist. For example, the syphilis study conducted in Tuskegee, AL eventually led to modern bioethics and human subjects’ protections, yet mistrust of the medical profession is still prevalent today.19,20
Persistent health disparities suggest traditional interventions may not always be effective for underserved populations across the urban–rural continuum. This may be in part due to the widening of socio-economic inequalities over the last 20 years21,22 and the hierarchical relationship between providers and patients complicated with trust issues.23 A community-engaged approach, which involves the inclusion of community members as partners in all stages of the research,24 can be effective in identifying and minimizing health effects related to environmental exposures by building capacity, resources, and skill sets within communities.25–27 A community-engaged framework also bridges the gap between academic institutions and communities to allay misconceptions, fears, or suspicions.25 Each partner contributes unique skills and knowledge to the project to initiate sustainable, effective change that is relevant to the communities’ health needs.1
The goal of the present research is to identify environmental health priorities in underserved urban and rural communities in Alabama. This includes how the communities define the term environment, how they perceive the environment to affect their health, specific priorities in their communities, and urban–rural differences.
Methods
The use of qualitative methods, such as focus groups, to prioritize environmental exposures of concern improves understanding the influence of social factors on environmental health and of exposure pathways.25 An exposure pathway is the route or course that a substance (i.e. chemical or pollutant) takes from the source to the target or end point considering how an individual comes into contact with it.28,29 Focus groups have been successful in tailoring lead and tobacco smoke exposure reduction programs to specific cultures and in developing community-based exposure surveillance systems, directly linking data gathering and community action.30 A community-engaged research strategy was utilized.31,32
Study populations
Birmingham, AL, the urban study site, is the largest city in Alabama with an estimated population of 212,413, where 26% of the population lives below the poverty line and 73% are self-identified as African American or Black.33 West Central AL, or The Black Belt region, originally named for the rich black topsoil, includes some of the poorest isolated rural counties in the United States. The focus groups included representatives from five Black Belt counties (Dallas, Monroe, Lowndes, Sumter, and Wilcox), with an estimated total population of 133,264 (63% Black), and 30% living below the poverty line.
This study involved University of Alabama at Birmingham (UAB) researchers collaborating with two community organizations working in urban and rural communities with high disease burdens and similar demographic compositions. In Birmingham, the authors partnered with Friends of West End (FoWE) 501(c)3, which serves to educate, engage, and advocate for Birmingham’s poorest and most underserved neighbourhoods and has implemented several health-related projects. In the Black Belt region, they worked with West Central Alabama Community Health Improvement League (WCACHIL) 501(c)3, which has partnered with UAB researchers on numerous projects for over 15 years. WCACHIL employs Community Health Advisors to educate and bring community members together on specific public health topics in the rural Black Belt region, which has some of the highest poverty and disease burdens in the US. The protocol was approved by the UAB Institutional Review Board. The community organizations recruited participants between the ages of 19–65 without regard to sex, race, or ethnicity. WCACHIL recruited 40 participants from five counties while FoWE recruited 33 participants from 17 Birmingham neighbourhoods (Fig. 1).
Fig. 1.
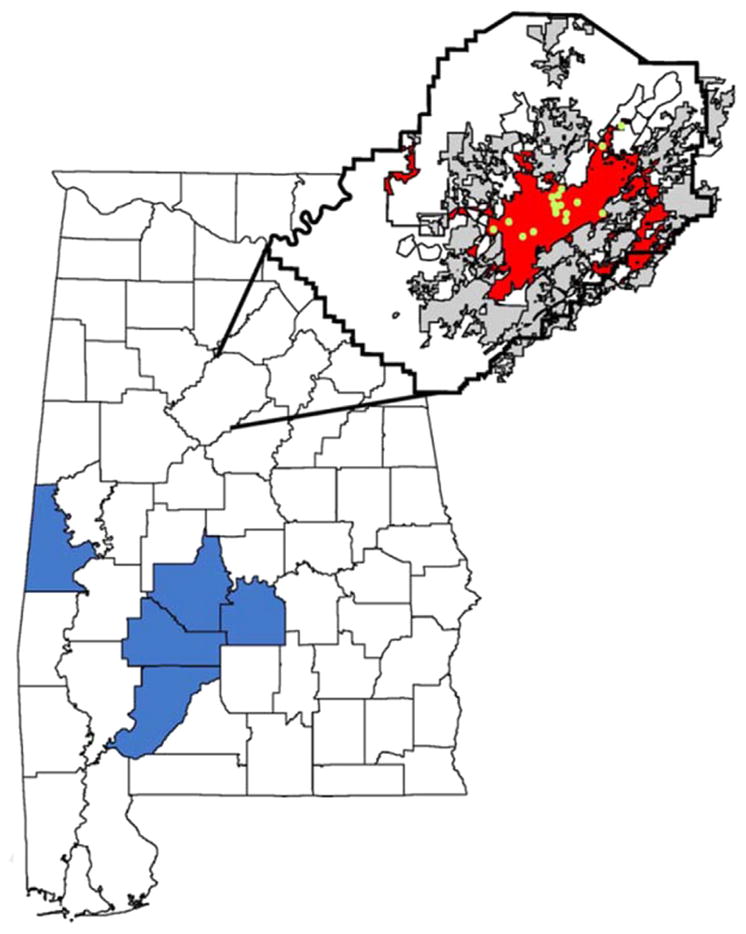
Map of focus group participant’s county or neighbourhood of residences. Rural focus group participants were from counties highlighted in blue (Wilcox, Dallas, Lowndes, Monroe, and Sumter Counties). Urban focus group participants were from highlighted Birmingham neighbourhoods in Jefferson County. Birmingham is red, with highlighted points representing 17 neighbourhoods: West End, Collegeville, Norwood Park, Harriman Park, Wylam, Kingston, Oakwood Place, East Pinson, Southside, Fountain Heights, Druid Hills, Evergreen, North Birmingham, Sun Hill (Center Point), Southtown, Irondale, and Ensley. Alabama basemap61 and Birmingham basemap.62
Focus group format
Researchers and community members worked collaboratively to develop the focus group format. Two of the eight focus groups (one urban and one rural) were moderated by community members trained by UAB staff,34 while the others were moderated by UAB researchers. The focus group moderators and observers participated in a training session and two additional practice sessions where moderators took turns practicing with the guide. The moderators were taught how to draw out concerns while avoiding introduction of bias by sharing their own views or engaging directly in the discussion, reflect back ideas to ensure clarity, and engage all participants.35–38 The moderator of each focus group was assisted by an observer, a UAB researcher or community member, who took notes and helped with informed consent. The moderators asked participants to respect their fellow participants’ opinions and to protect their fellow participants’ confidentiality outside of the discussion. Focus group discussions were recorded and all data was stored in locked cabinets or on encrypted files on a secured network.
The focus group discussion was developed to address four main elements: a) positive attributes of participants’ communities, b) defining the term ‘environment,’ c) discussing environmental priorities specific to the individuals’ communities, and d) establishing environmental priorities based on a prepared list of potential environmental concerns, following the guidelines suggested by Lobdell et al. (2005).30
Briefly, participants introduced themselves and stated one positive attribute of their community. Then discussion turned to use of the term ‘environment’ in the media and in their community, what the term ‘environmental problems’ meant to them, and whether they considered environmental problems to be related to one’s health. The participants were then asked to identify environmental problems in their own communities. Finally, a list of 28 potential environmental concerns was distributed and read aloud. The list of environmental exposures was collaboratively formulated based on Slovic’s work on risk perception (1987),39 recent known environmental exposures (i.e. tornados) experienced by these populations, and based on the community leaders’ expertise and insight into their specific communities.39 Participants were asked to note those that are considered big concerns in their community and then circle their greatest concern. There was additional space for the participants to write in their own concerns.
Introducing the list of potential priorities after the discussion was intended to permit the individuals the ability to share their ideas without any preconceived notions, limitations of the definition of environment, or influences of the researchers. The list was to spark any additional comments, prevent a dominant group member from controlling the group’s input, and allow participants to write in ideas with additional privacy and confidentiality. Researchers utilized the quantitative data (counts from the survey) to compliment data from the qualitative discussions (that draw out the research questions how and why) as well as for standardization across the various groups and populations studied.30 The combination of focus groups and surveys provides an examination of the prevalence of the issues or themes from the focus groups40 and assists in development and early testing for further topic specific focus groups.41
The WCACHIL focus groups were held at the Wilcox Female Institute, Camden, AL and the FoWE focus groups were held at the West End Public Library, Birmingham, AL. The participants received dinner and were randomly divided into four evenly-distributed small groups to minimize the potential for bias. After reviewing informed consent procedures, the participants filled out a demographic survey, participated in the 45-min focus group, and finally gathered for a large group discussion to discuss priorities and identify the next steps for researchers and community members. The participants received a small incentive to help cover transportation costs.
Data analysis
The demographics were summarized and compared to identify any significant differences between the urban and rural sites. Focus group recordings were transcribed by one researcher and then independently verified by another listener. A grounded theory approach was used to analyse the data.42 Coding was developed to identify positive attributes, definitions of environment, environmental issues that affect health, and environmental concerns in participants’ communities. At least two researchers independently coded the transcripts.43 Together they verified coding to create the final results for each focus group. Inter-rater reliability was 87.3% meaning 52 of the 408 responses were different between the two coders. For each difference, all three coders discussed the difference and a final consensus conclusion was found. Environmental priorities brought up during discussion and environmental priorities presented on the list were grouped into six broad categories (Table 1). Both qualitative and quantitative methods were used, following previous research.44–47 To examine responses quantitatively, the number of urban and rural participants and the number of urban and rural focus groups that identified each positive attribute, definition of environment, or environmental concern was noted to monitor for group effects. Qualitative analysis methods included exploring individual responses to examine the context of the quantitative estimates.
Table 1.
Categorization of environmental health concerns.a
| Discussion items | |||||
|---|---|---|---|---|---|
| Pests | Weather & geology | Built environment | Waste and emissions | Transportation | Other |
| Stray dogs | Abandoned houses | Septic tanks leakage & improper sewage control | Road maintenance, logging trucks | No community places for seniors, kids, groceries | |
| Mosquitoes & bees | Burning houses/over grown lots | Unclean drinking water – taste, smell chlorine | Speeding | Papermills: lack regulations enforcement & workplace safety | |
| Youth: need curfew & place to play | Pollution from industry (papermill) | Noise – cars, clubs, people | |||
| No water access – wells dry | Air pollution: cars | Insufficient fire dept, trucks, hydrants | |||
| Air Pollution: plants Dumping & garbage Sewer issues Fertilizer |
Lack youth support Drugs Crime |
||||
|
| |||||
| List itemsa
| |||||
| Pests | Weather & Geology | Built environment | Waste & emissions | Transport | Other |
|
| |||||
| Rats, snakes, & other pests | Tornados & other natural disasters | Abandoned houses overgrown lots | Pollution in local streams or lakes | Train derailments or truck accidents involving dangerous chemicals | Unsafe working conditions |
| Mosquitoes, ticks, & other insects | Summer heat | House fires | Dangerous chemicals in the soil | Abandoned cars | Terrorism |
| Dog poop | Winter cold Radon Flooding |
Lead paint Mould |
Landfills/dumps Unsafe drinking water Air pollution Garbage piling up Litter Smog |
Too much traffic | Noise Graffiti |
For analysis, the potential concerns on the list were collapsed into broad groups as shown here, but were listed in a randomized order without categorization when distributed to focus group participants. Participants were able to write in additional priorities not listed. Rural residents wrote in stray animals (n = 2), factory fumes (1), children in the streets (1), drunk drivers (1), bad roads (1), and old city pipes (1). Urban residents wrote in bad road conditions (1), speeding (1), bad sewer (1), and drugs (1).
Environmental priorities brought up during discussion (prior to the introduction of the prepared list of environmental issues) were compared to environmental priorities identified from the list of 28 concerns by first developing a ranked list based on the number of participants who identified the priority. In addition, a network diagram using Cytoscape48 was developed. Triangles represent environmental priorities vocalized by participants during the discussion and edges (lines) represent connections made between environmental priorities. Edges between items are based on similarity of topic. Size of the node is based on the total number of people identifying the priority multiplied by the number of focus groups the priority was identified. Circles represent top environmental priorities identified from the list. The size of the list nodes are based on the total participants that identified the concern as the top priority from the list, multiplied by the number of focus groups. For participants who circled more than one top priority, the circled top priorities are divided by the number circled.
Results
Study population
The demographics of focus group participants at both urban and rural sites indicate that the participants were predominately from low-income (50% making less than $20K) African American communities (Table 2). A high proportion of participants in both communities had some college courses (Rural 32.5%, Urban 42.4%), but few had completed higher level degrees (Rural 20%, Urban 21.2%). More females participated in the focus groups at both sites (Rural 80%, Urban 72.7%). The median age of participants was 52 (Camden) and 56 (Birmingham) with the same range of ages present (20–80) in both communities.
Table 2.
Demographics of focus group participants.
| Camden, AL | Birmingham, AL | |
|---|---|---|
| n | 40 | 33 |
| Age | ||
| Maximum | 80 | 80 |
| Minimum | 20 | 20 |
| Median | 52 | 56 |
| Unknown | 2 | 1 |
| Sex by count (%) | ||
| Male | 7 (17.5) | 8 (24.2) |
| Female | 32 (80) | 24 (72.7) |
| Unknown | 1 (2.5) | 1 (3) |
| Race by count (%) | ||
| Black or African American | 39 (97.5) | 28 (84.8) |
| Some other race or mixed race | 0.0 | 5 (15.2) |
| Unknown | 1 (2.5) | 0.0 |
| Hispanic or Latino by count (%) | ||
| Yes | 0.0 | 1 (3) |
| No | 39 (97.5) | 30 (90.9) |
| Unknown | 1 (2.5) | 2 (6.1) |
| Highest level of education by count (%) | ||
| Less than a high school diploma | 2 (5) | 4 (12.1) |
| High school diploma | 13 (32.5) | 5 (15.2) |
| Postsecondary certificate | 3 (7.5) | 2 (6.1) |
| Some college courses or associate’s degree | 13 (32.5) | 14 (42.4) |
| Bachelor’s degree | 2 (5) | 6 (18.2) |
| Graduate degree | 6 (15) | 1 (3) |
| Unknown | 1 (2.5) | 1 (3) |
| Income, pre-tax by count (%) | ||
| Less than $20,000 | 20 (50) | 16 (48.5) |
| $20,000–$49,999 | 16 (40) | 11 (33.3) |
| $50,000–$74,999 | 2 (5) | 2 (6.1) |
| $75,000+ | 0.0 | 1 (3) |
| Unknown | 2 (5) | 3 (9.1) |
Positive attributes as identified by community members
Similarities and differences in positive attributes of participants’ communities expressed during the focus groups are summarized in Fig. 2. Participants in both locations identified quiet, family-oriented, and friendliness of people as positive attributes of their community, but more rural participants identified quiet and family-oriented, while friendliness was identified by more urban participants. In addition, urban participants, but not rural participants, identified convenient location and community involvement as positive attributes of their community, while low crime and outdoors were identified in rural focus groups. For example, a female resident from a rural focus group observed the quiet and that there is ‘never a problem with breakins, people never get in fights, nothing like that’ and a male stated ‘I like fishing and hunting....fishing environment is good. Hunting environment is good. Walking environment is good because you’re not confined to a certain area.’
Fig. 2.

Venn diagram of positive attributes of participants’ communities. Numbers in parentheses reflect the total number of people who identified the attribute followed by the number of focus groups represented. Average positive attributes per urban participant (1.27), average positive attributes per rural participant (1).
Definition of the term ‘environment’
Focus group participants were asked to describe if and where they have heard the term environment, and what the word ‘environment’ means to them. This was to determine whether rural and urban populations had a similar definition of the term and whether their responses (environmental priorities) could be compared (urban versus rural). Several urban and rural participants emphasized social as well as physical aspects of the environment in their answers, using terms such as ‘all that surrounds us’ or ‘surroundings including air, water, and people.’ One urban participant described environment as ‘It’s not always the chemicals. Sometimes it’s the company that you keep, or the friends that you have, or the neighbourhood that you live in is a high crime area and that’s going to affect you later in life.’ Other participants gave specific examples, such as a rural participant stating ‘You can smell the odor coming from that mill and smell that it’s just bad, bad environment because you’re breathing it in.’ No clear differences between urban and rural groups in defining environment were evident when answers were coded as physical environment (Rural n = 16, Urban n = 15), social environment (Rural n = 7, Urban n = 6), or both physical and social environment (Rural n = 6, Urban n = 8) where n = the number of participants who responded with each respective environmental definition category. The categorization of physical environment, social environment, or a combination of the two, was necessary to understand the scope of the participant’s priorities.
Environmental health priorities (EHP)
Participants were asked to discuss environmental problems in their communities that concerned them the most, and then to identify top priorities from a list of 28 concerns. Urban residents highlighted abandoned houses as a clear priority whereas responses from rural residents were more varied and included pollution from industry, garbage, water and pest problems (Table 3). A male from an urban focus group expressed his concerns over abandoned houses:
One of mine will be overgrown lots and vacant houses. Or houses that have caught on fire and been there for a year and a half or two years now…may be homeless people, and a lot of time they go and set those places a-fire. That is just not good for the neighborhood.
Table 3.
Top five environmental priorities in urban (Birmingham) and rural (West Central) Alabama based on 8 focus groups (n = 40, rural; n = 33, urban) conducted in June, 2012.
| Top priorities during discussiona | Top priorities marked on list (after discussion)b | ||
|---|---|---|---|
| Birmingham | West Central AL | Birmingham | West Central AL |
| Abandoned houses (23, 4) | Industrial pollution (16, 3) | Abandoned houses (14.3, 4) Air pollution (6, 4) |
Mosquitoes, ticks, and other insects (9.8, 4) |
| Air pollution from 2 plants (13, 3) Crime (12, 4) |
Road issues (14, 4) Garbage and dumping (13, 4) |
Dangerous chemicals in the soil (3, 3) Noise (1.6, 3) |
Air pollution (3.6, 4) Unsafe drinking water (2.8, 2) Litter (2.6, 4) |
| Dumping garbage (8, 4) | Septic tank and sewer issues (9, 3) | Litter (1.3, 2) | Tornados and other natural disasters (2.5, 3) |
| Lack of community places (7, 2) | Drinking water quality (8, 2) | ||
Numbers in parentheses reflect the total number of people followed by the number of focus groups represented. Urban participants averaged 2.4 priorities per person, rural participants averaged 2.3 priorities per person.
For individuals circling multiple items, each item was assigned a fraction by dividing by the number of top priorities circled.
Air pollution and waste were considered top priorities in both urban and rural communities, based on both discussion and subsequent listed survey results. In rural focus groups, the list item ‘mosquitoes, ticks, and other insects’ ranked as a top priority, but was sparsely mentioned during the initial discussion. Additional items that were brought up in the urban and rural discussion were the lack of community places and crime, while rural residents brought up septic tank and sewer issues in their discussion. For example, a female from West Central Alabama describes the sewage issue:
You actually smell the smell. And you don’t actually see the raw sewage, but it’s still the water, the water that is running along draining. I guess it’s coming from a pipe that they were using to build a sewer line. And the water’s just sitting there on top of that. They got little kids out there playing in it.
In the urban focus groups, the postlist discussion clarified issues brought up earlier, expanded their ideas of environmental priorities, and also discussed potential next steps for the community to address certain issues. One woman clarified that cars are the source of litter issues. Another woman clarified about the mould issue in public houses and its effects on the health of children, elderly, and disabled residents. Abandoned houses was brought up in three groups (one group did not have time for discussion), reinforcing the participants’ prior concern, while the call for organized leadership was brought up in two groups.
The rural participants responded with health concerns from inhaling the air from the industrial plants and breathing the exhaust from the logging trucks as connected with lung disease, breast and other cancers, asthma, allergies, and sinus issues. The threat of dogs and their potential to attack was connected to concerns for physical safety and as a deterrent to walking or exercising in the neighbourhoods. They connected the concerns about trash and littering to keeping their drinking water safe and clean. (Nutrition and high blood pressure were also mentioned. Some were concerned about the crime, drugs, and alcohol and their negative effects on the physical and spiritual well-being of the children of the community.)
The urban participants also focused on what they were breathing and how it negatively affected their health. They identified poor air quality as inducing cancer, coughing, asthma, headaches, allergies, and affecting individuals who suffered from other ailments. They suggested the recent smoking ban in buildings was beneficial to their health. Breathing mould was also thought to cause illness in some communities. Like the rural participants, the urban participants mentioned the importance of availability of nutritious foods and exercising.
The rural community’s discussion after the list reinforced what they selected as top priorities, expanded their definition of environment, and linked their selection to health effects. For instance, mosquitoes were emphasized in three groups and were linked to flooding and inability of children to play outside. One woman linked the problem of house fires and the one fire truck serving the whole community, while another discussed the problem that churches serving as improvised shelters take on legal liability during tornadoes. A network approach was used to visualize environmental priority results from focus group discussion and survey results (Fig. 2). The figure shows edges (lines) between environmental priorities vocalized during discussion (triangles) and those subsequently circled from among the listed concerns (circles).
Categorization of discussion and list items into six themes are identified by colour (Key within Fig. 3). Waste and emissions (green) were emphasized in both urban and rural focus groups based on both the discussion and list survey results. Urban focus group discussions, and to a lesser extent rural focus groups, emphasized social environmental concerns such as lack of community places and drugs. Representation of the urban results shows the built environment, particularly abandoned houses, and how they may be associated with other environmental priorities including pests, crime, and drugs.
Fig. 3.

Network diagram of environmental priorities in urban and rural communities. Data from Birmingham, AL focus groups (A.) and Camden, AL focus groups (B.). Size of nodes based on number of participants multiplied by number of focus groups identifying the item in discussion (triangles) or on list (circles). Categorization of items (colour) described in the key. Edges (lines) between nodes based on discussion (triangle to triangle) or based on similarity of topic between discussion and list items (triangle to circle).
In general, findings indicate risks associated with rare events were not prioritized by urban or rural participants (Fig. 3). While tornadoes and other natural disasters, terrorism, train derailments/chemical accidents, flooding, and house fires were part of the list of environmental issues, neither urban nor rural participants ranked them highly in either discussion or list. In addition, results indicate participants focused on issues that have tangible approaches to address the problem, such as abandoned houses, dumping and garbage, road maintenance, and sewer and septic issues. For example when the focus group moderator read aloud the list of priorities, after ‘summer heat’ was read, a rural female focus group participant asked ‘What [are] we going to do about that?’
Discussion
In environmental health research, community-engaged focus groups are increasingly being used to explore the complex interaction between social and physical factors as it relates to variations in exposures and health outcomes.25 As Macintyre and Ellaway (2003) suggest, many of the individual-level factors epidemiologists commonly control for (e.g. race, income, sex, education) may represent variables on the causal pathway between neighbourhood exposures and individual health outcomes.49 Using a combination of quantitative and qualitative methods,44–47 it has been identified community definitions of environment and compared environmental priorities in urban and rural communities with known health disparities. The goal of the present study was to engage communities to determine similarities and differences in environmental concerns to develop hypotheses of environmental factors that may contribute to health disparities in these settings.
Results show demographics were similar across urban and rural focus group participants and definitions of environment were inclusive, emphasizing both physical and social aspects in both urban and rural focus groups, eliminating sources of potential confounding and bias that would make comparisons of environmental priorities across these settings difficult. In discussing environmental concerns, urban focus groups emphasized connections between social and physical aspects, particularly when discussing abandoned houses. This focus on social issues in the urban focus groups is consistent with differences in positive attributes discussed, with urban focus groups noting community involvement and friendliness and rural focus groups noting low crime and outdoors. Rural participants were more varied in their priorities, with road maintenance, water and sewer, and garbage management identified across most of the focus groups during discussion. Listed responses highlighted insect pests as another possible priority in rural focus groups; however, this result was not consistent with open discussion results. The present findings suggest air pollution from nearby industries was a common priority across both urban and rural settings.
Using a combination of methods to analyse and visualize results from structured focus groups developed in partnership with community groups has provided data that can be useful in developing future community-based participatory research hypotheses and in pointing toward follow-on actions and interventions.50 Air pollution from industrial sources and waste management issues are clearly important community concerns in these rural and urban communities; as such, this would be an important area for additional work. Community-based participatory research on the potential health benefits from better addressing the abandoned houses issue would also be valuable in the urban communities, and community-based work to better address sewer and water concerns would be appropriate in the rural communities.
Limitations
Broad generalizations from the results of the current study are limited by small sample size and non-random recruitment of participants. However, active engagement of community members in the design, training, and implementation of the focus groups likely increased the openness of the discussions.51 As with all community-engaged approaches, this study relied on the importance of an engaged community or ‘buy-in’ to research in order to inform and initiate change.50,52 An expanded list of environmental priorities from predominately physical environmental factors to include more social factors which may contribute to exposure and health effects from those exposures may be useful and is supported by the focus group discussions and previous studies.24,25
The lack of focus on tornadoes and disasters in the focus groups was notable. A large body of risk perception research suggests that citizens tend to prioritize ‘dread’ risk factors, characterized by the catastrophic nature, perceived lack of control, and fatal consequences, in regards to demanding policies and regulations.39 In contrast, participants in the focus groups here tended to prioritize tangible issues encountered in everyday life, such as air pollution, garbage, road maintenance, abandoned homes, and lack of community places. One possible explanation is that disasters were seen as rare or distant. Indeed, some research suggests risks associated with rare events are overemphasized in areas just following an event, but underemphasized if rare events are far away in space and/or time.53 Yet particularly destructive tornados had hit many parts of Alabama in the year prior to the focus groups. Another possible explanation is that focus group participants commented on local issues within communities, and that disasters were seen as being more a state and/or national level problem not directly affecting an individual’s everyday life.54 This is akin to the issue of climate change. A recent survey on public perception of risks associated with climate change suggests US citizens perceive climate change as primarily affecting others, but not themselves.55 Another possibility is that most participants see tornados and other disasters as falling into a different category of concern outside of what are viewed as ‘environmental health’ issues.
Despite the important information gleaned from these focus groups, the approach has specific limitations. One such example is the potential for gender bias. Women are more likely to participate in scientific studies than men.56 However, men may have a tendency to dominate conversation in mixed-sex groups, which may irritate or diminish women’s voice in the group.57 Gustafson (1998) indicates that while men and women worry about the same risks, women systematically worry more.58 The study design of going beyond a quantitative study design to incorporate qualitative methods (i.e. open-ended questions) has been identified by Gustafson as helpful at eliciting the differences risk perception according to gender.58 Differences in gender are not the only limitation of focus groups according to recent literature. Higher educated individuals are more likely to participate.56 Those with the exposure are more likely to participate than those who are not exposed.56 In addition, Hollander (2004) indicates the potential for exaggeration of information when you know the other participants in the focus group.59
Using data such as those generated here, researchers and policymakers can better understand how underserved communities perceive environmental health priorities and concerns. This, in turn, can help in the development of more effective strategies for studying and addressing environmental problems. Against a background of mistrust and disparities, establishing a genuine relationship with the community builds trust, allows for identification of key issues, provides the foundation for a bi-directional flow of knowledge,60 and helps to create the kinds of partnership needed for effective interventions and management strategies.
The information gathered at these focus groups was disseminated back to the community and community leaders in June of 2013. The aim was to help identify priorities specific to the communities for local discussion and potential community action. These steps can also help to create longer-term systematic solutions that may be generalizable to other communities. For example, as a result of the identification of priorities and the actions of community leaders, the partnership effectively conducted an environmental education program in the Spring of 2013 targeted at youths in the urban community. In the near future, these priorities will be brought to the local governmental organizations in both communities in order to communicate the needs of the population to the decision-makers. Finally, many urban and rural communities throughout the United States are facing similar issues of environmental injustice. Identification in the scientific literature is a step towards raising awareness of the value of researcher-community partnerships for understanding and addressing local environmental concerns.
Acknowledgments
The authors gratefully acknowledge the support from the National Institute of Health (grant number R21 ES020205). They recognize the crucial role of the Center for the Study of Community Health, supported by the Centers for Disease Control and Prevention (cooperative agreement number U48/DP001915). Thanks to focus group participants and volunteers from community organization partners for their time and efforts. Special thanks to Dzigbodi Doke at the (UAB School of Public Health) and Meagan Sloan (UAB Medical School) for their contributions at the focus groups sessions.
Footnotes
Ethical approval
This study was reviewed and approved by the University of Alabama at Birmingham Institutional Review Board (protocol number X110706005). All subjects gave informed consent to participate.
Competing interests
The authors acknowledge no competing financial or non-financial interests.
References
- 1.Cook WK. Integrating research and action: a systematic review of community-based participatory research to address health disparities in environmental and occupational health in the USA. J Epidemiol Community Health. 2008 Aug;62(8):668–76. doi: 10.1136/jech.2007.067645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.AHQR. Agency for Healthcare Research and Quality. National healthcare disparities report 2011. US Department of Health and Human Services; 2012. [Google Scholar]
- 3.Bolen JC, Rhodes L, Poewll-Giner EE, Bland SD, Holtzman State-specific prevalence of selected health behaviors, by race and ethnicity—Behavioral Risk Factor Surveillance System, 1997. Division of Adult and Community Health, National Center for Chronic Disease Prevention and Health Promotion, USA. MMWR CDC Surveill Summ. 2000 Mar 24;49(2):1–60. [PubMed] [Google Scholar]
- 4.Bennett KJ, Olatosi B, Probst JC. Health disparities: a rural-urban chartbook. Columbia, SC: South Carolina Rural Health Research Center; 2008. [Google Scholar]
- 5.Kent ST, McClure LA, Zaitchik BF, Gohlke JM. Area and individual-level risk factors and birth outcome trends in urban and rural Alabama: a time-series analysis. BMC Public Health. 2013 doi: 10.1186/1471-2393-13-129. in review. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gordon-Larsen P, Nelson MC, Page P, Popkin BM. Inequality in the built environment underlies key health disparities in physical activity and obesity. Pediatrics. 2006 Feb;117(2):417–24. doi: 10.1542/peds.2005-0058. [DOI] [PubMed] [Google Scholar]
- 7.Gochfeld M, Burger J. Disproportionate exposures in environmental justice and other populations: the importance of outliers. Am J Public Health. 2011 Dec;101(Suppl 1):S53–63. doi: 10.2105/AJPH.2011.300121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Fustinoni S, Campo L, Satta G, Campagna M, Ibba A, Tocco MG, et al. Environmental and lifestyle factors affect benzene uptake biomonitoring of residents near a petrochemical plant. Environ Int. 2012 Feb;39(1):2–7. doi: 10.1016/j.envint.2011.09.001. [DOI] [PubMed] [Google Scholar]
- 9.Lipscomb HJ, Argue R, McDonald MA, Dement JM, Epling CA, James T, et al. Exploration of work and health disparities among black women employed in poultry processing in the rural south. Environ Health Perspect. 2005 Dec;113(12):1833–40. doi: 10.1289/ehp.7912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hartley D. Rural health disparities, population health, and rural culture. Am J Public Health. 2004 Oct;94(10):1675–8. doi: 10.2105/ajph.94.10.1675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Morin A, Brook JR, Duchaine C, Laprise C. Association study of genes associated to asthma in a specific environment, in an asthma familial collection located in a rural area influenced by different industries. Int J Environ Res Public Health. 2012 Aug;9(8):2620–35. doi: 10.3390/ijerph9082620. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lin S, Wang X, Yu IT, Tang W, Miao J, Li J, et al. Environmental lead pollution and elevated blood lead levels among children in a rural area of China. Am J Public Health. 2011 May;101(5):834–41. doi: 10.2105/AJPH.2010.193656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Rioux CL, Gute DM, Brugge D, Peterson S, Parmenter B. Characterizing urban traffic exposures using transportation planning tools: an illustrated methodology for health researchers. J Urban Health. 2010 Mar;87(2):167–88. doi: 10.1007/s11524-009-9419-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Young GS, Fox MA, Trush M, Kanarek N, Glass TA, Curriero FC. Differential exposure to hazardous air pollution in the United States: a multilevel analysis of urbanization and neighborhood socioeconomic deprivation. Int J Environ Res Public Health. 2012 Jun;9(6):2204–25. doi: 10.3390/ijerph9062204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Mohai P, Lantz PM, Morenoff J, House JS, Mero RP. Racial and socioeconomic disparities in residential proximity to polluting industrial facilities: evidence from the Americans’ Changing Lives Study. Am J Public Health. 2009 Nov;99(Suppl 3):S649–56. doi: 10.2105/AJPH.2007.131383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Inder KJ, Lewin TJ, Kelly BJ. Factors impacting on the well-being of older residents in rural communities. Perspect Public Health. 2012;132(4):182–91. doi: 10.1177/1757913912447018. [DOI] [PubMed] [Google Scholar]
- 17.Berkman LF, Syme SL. Social networks, host resistance, and mortality: a nine-year follow-up study of Alameda County residents. Am J Epidemiol. 1979 Feb;109(2):186–204. doi: 10.1093/oxfordjournals.aje.a112674. [DOI] [PubMed] [Google Scholar]
- 18.McKinlay JB, McKinlay SM, Beaglehole R. A review of the evidence concerning the impact of medical measures on recent mortality and morbidity in the United States. Int J Health Serv. 1989;19(2):181–208. doi: 10.2190/L73V-NLDL-G7H3-63JC. [DOI] [PubMed] [Google Scholar]
- 19.Gamble VN. Under the shadow of Tuskegee: African Americans and health care. Am J Public Health. 1997 Nov;87(11):1773–8. doi: 10.2105/ajph.87.11.1773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Brandon DT, Isaac LA, LaVeist TA. The legacy of Tuskegee and trust in medical care: is Tuskegee responsible for race differences in mistrust of medical care? J Natl Med Assoc. 2005 Jul;97(7):951–6. [PMC free article] [PubMed] [Google Scholar]
- 21.Berkman LF. Social epidemiology: social determinants of health in the United States: are we losing ground? Annu Rev Public Health. 2009;30:27–41. doi: 10.1146/annurev.publhealth.031308.100310. [DOI] [PubMed] [Google Scholar]
- 22.AHQR. Agency for Healthcare Research and Quality. National healthcare disparities report. Rockville, MD: 2005. [Google Scholar]
- 23.Berge JM, Mendenhall TJ, Doherty WJ. Using community-based participatory research (CBPR) to target health disparities in families. Fam Relat. 2009;58(4):475–88. doi: 10.1111/j.1741-3729.2009.00567.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Green L, Fullilove M, Evans D, Shepard P. “Hey, mom, thanks!”: use of focus groups in the development of place-specific materials for a community environmental action campaign. Environ Health Perspect. 2002 Apr;110(Suppl 2):265–9. doi: 10.1289/ehp.02110s2265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Scammell MK. Qualitative environmental health research: an analysis of the literature, 1991–2008. Cien Saude Colet. 2011 Oct;16(10):4239–55. doi: 10.1590/s1413-81232011001100030. [DOI] [PubMed] [Google Scholar]
- 26.Kimmel CA, Collman GW, Fields N, Eskenazi B. Lessons learned for the National Children’s Study from the National Institute of Environmental Health Sciences/U.S. Environmental Protection Agency Centers for Children’s Environmental Health and Disease Prevention Research. Environ Health Perspect. 2005 Oct;113(10):1414–8. doi: 10.1289/ehp.7669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Parker EA, Chung LK, Israel BA, Reyes A, Wilkins D. Community organizing network for environmental health: using a community health development approach to increase community capacity around reduction of environmental triggers. J Prim Prev. 2010 Apr;31(1–2):41–58. doi: 10.1007/s10935-010-0207-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Exposure Pathway. Waste cleanup and risk assessment glossary. United States Environmental Protection Agency; 2012. Dec 24, [accessed 20 June 2013]. http://www.epa.gov/oswer/riskassessment/glossary.htm#ehttp://www.epa.gov/opptintr/rsei/tools/glossary.html. [Google Scholar]
- 29.Agency for Toxic Substances and Disease Registry. [accessed 20 June 2013];Glossary of terms. 2009 Jan 1; http://www.atsdr.cdc.gov/glossary.html#G-D-
- 30.Lobdell DT, Gilboa S, Mendola P, Hesse BW. Use of focus groups for the environmental health researcher. J Environ Health. 2005 May;67(9):36–42. [PubMed] [Google Scholar]
- 31.Ross LF, Loup A, Nelson RM, Botkin JR, Kost R, Smith GR, Gehlert S. Human subjects protections in community-engaged research: a research ethics framework. J Empir Res Hum Res Ethics. 2010 Mar 5;(1):5–17. doi: 10.1525/jer.2010.5.1.5. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2946318/ [DOI] [PMC free article] [PubMed]
- 32.Michener L, Cook J, Ahmed SM, Yonas MA, Coyne-Beasley T, Aguilar-Gaxiola S. Aligning the goals of community-engaged research: why and how academic health centers can successfully engage with communities to improve health. Acad Med. 2012 Mar;87(3):285–91. doi: 10.1097/ACM.0b013e3182441680. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Bureau USC. Population statistics. Population estimates. 2010. [Google Scholar]
- 34.Teufel-Shone NI, Williams S. Focus groups in small communities. Prev Chronic Dis. 2010 May;7(3):A67. [PMC free article] [PubMed] [Google Scholar]
- 35.Focus groups in action: a practical guide. University of Washington; [Google Scholar]
- 36.Krueger RA. Focus group kit: moderating focus groups. Vol. 4. Sage Publications; 1997. [Google Scholar]
- 37.Krueger RA. Designing and conducting focus group interviews. 2002 [Google Scholar]
- 38.University of Texas at Austin. [accessed 15 May 2012];Evaluate programs: conducting focus groups. 2011 Web site, http://www.utexas.edu/academic/ctl/assessment/iar/programs/gather/method/focus-conduct.php.
- 39.Slovic P. Perception of risk. Science. 1987;236(4799):280–5. doi: 10.1126/science.3563507. [DOI] [PubMed] [Google Scholar]
- 40.Nassar-McMillan SC, Borders LD. Use of focus groups in survey item development. Qual Rep. 2002 Mar 7;(1) Retrieved 22 June 2013, from: http://www.nova.edu/ssss/QR/QR7-1/nassar.html.
- 41.Morgan David L. Focus groups. Annu Rev Sociol. 1996:129–52. 22. http://www.jstor.org/stable/2083427.
- 42.Snape D, Spencer L. The foundations of qualitative research. In: Ritchie J, Lewis J, editors. Qualitative research practice. London: Sage Publications; 2003. [Google Scholar]
- 43.Goldberg-Freeman C, Kass NE, Tracey P, Ross G, Bates-Hopkins B, Purnell L, et al. “You’ve got to understand community”: community perceptions on “breaking the disconnect” between researchers and communities. Prog Community Health Partnersh. 2007;1(3):231–40. doi: 10.1353/cpr.2007.0021. [DOI] [PubMed] [Google Scholar]
- 44.Carlsen B, Glenton C. Scanning for satisfaction or digging for dismay? Comparing findings from a postal survey with those from a focus group-study. BMC Med Res Methodol. 2012;12:134. doi: 10.1186/1471-2288-12-134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Calderón JL, Baker RS, Wolf KE. Focus groups: a qualitative method complementing quantitative research for studying culturally diverse groups. Educ Health (Abingdon) 2000;13(1):91–5. doi: 10.1080/135762800110628. [DOI] [PubMed] [Google Scholar]
- 46.Quantitative and qualitative evaluation methods. Public Health Institute, Center for Civic Partnerships; 2007. http://www.civicpartnerships.org/docs/tools_resources/Quan_Qual%20Methods%209.07.htm. [Google Scholar]
- 47.Frechtling J, Sharp Westat L, editors. User-friendly handbook for mixed method evaluations. National Science Foundation; Aug, 1997. http://www.nsf.gov/pubs/1997/nsf97153/start.htm. [Google Scholar]
- 48.Smoot ME, Ono K, Ruscheinski J, Wang PL, Ideker T. Cytoscape 2. 8: new features for data integration and network visualization. Bioinformatics. 2011 Feb;27(3):431–2. doi: 10.1093/bioinformatics/btq675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Macintyre S, Ellaway A. Neighborhoods and health: an overview. In: Kawachi I, Berkman LF, editors. Neighborhoods and health. New York: Oxford University Press; 2003. pp. 20–44. [Google Scholar]
- 50.Martinez LS, Rubin CL, Russell B, Leslie LK, Brugge D. Community conceptualizations of health: implications for transdisciplinary team science. Clin Transl Sci. 2011 Jun;4(3):163–7. doi: 10.1111/j.1752-8062.2011.00289.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Israel BA, Coombe CM, Cheezum RR, Schulz AJ, McGranaghan RJ, Lichtenstein R, et al. Community-based participatory research: a capacity-building approach for policy advocacy aimed at eliminating health disparities. Am J Public Health. 2010 Nov;100(11):2094–102. doi: 10.2105/AJPH.2009.170506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Eng E, Salmon ME, Fitzhugh M. Community empowerment: the critical base for primary health care. Fam Community Health. 1992;15(1):1–12. [Google Scholar]
- 53.Slovic P, Weber E. Perception of risk posed by extreme events. Columbia University and Wissenschaftskolleg zu; Berlin: 2002. [Google Scholar]
- 54.Gray L, MacDonald C, Mackie B, Paton D, Johnston D, Baker MG. Community responses to communication campaigns for influenza A (H1N1): a focus group study. BMC Public Health. 2012;12:205. doi: 10.1186/1471-2458-12-205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Akerlof K, DeBono R, Berry P, Leiserowitz A, Roser-Renouf C, Clark KL, et al. Public perceptions of climate change as a human health risk: surveys of the United States, Canada and Malta. Int J Environ Res Public Health. 2010;7:2559–606. doi: 10.3390/ijerph7062559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Galea S, Tracy M. Participation rates in epidemiologic studies. Ann Epidemiol. 2007 Sep;(9):643–53. 17. doi: 10.1016/j.annepidem.2007.03.013. http://www.sciencedirect.com/science/article/pii/S1047279707001470. [DOI] [PubMed]
- 57.Krueger RA, Casey MA. Focus groups: a practical guide for applied research. 4. SAGE; 2009. p. 67. [Google Scholar]
- 58.Gustafson PE. Gender differences in risk perception: theoretical and methodological perspectives. Risk Anal. 1998;18(6):805–11. doi: 10.1023/b:rian.0000005926.03250.c0. [DOI] [PubMed] [Google Scholar]
- 59.Hollander JA. The social contexts of focus groups. J Contemp Ethnogr. 2004 Oct;(5):602–37. 33. http://jce.sagepub.com/content/33/5/602.full.pdf.
- 60.Makosky Daley M, James AS, Ulrey E, Joseph S, Talawyma Choi WS, et al. Using focus groups in community-based participatory research: challenges and resolutions. Qual Health Res. 2010;20(5):697–706. doi: 10.1177/1049732310361468. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Library. Alabama Counties: University of Alabama Map Library. 2012 http://alabamamaps.ua.edu/contemporarymaps/alabama/basemaps/index.html2012.
- 62.Arkyan Jefferson county Alabama incorporated and unincorporated areas Birmingham highlighted. 2007 http://en.wikipedia.org/wiki/File:Jefferson_County_Alabama_Incorporated_and_Unincorporated_areas_Birmingham_Highlighted.svg#file2007.