

Abstract
Objective:
To examine college athletic trainers' confidence in helping female athletes who have eating disorders.
Design and Setting:
We mailed a 4-page, 53-item survey to head certified athletic trainers at all National Collegiate Athletic Association Division IA and IAA institutions (N = 236). A 2- wave mailing design was used to increase response rate.
Subjects:
A total of 171 athletic trainers returned completed surveys for a response rate of 77%. Eleven institutions either did not identify their head athletic trainer or did not have an identifiable mailing address. Two surveys were undeliverable because of incorrect mailing addresses.
Measurements:
The survey consisted of 4 subscales: (1) efficacy expectation, (2) outcome expectation, (3) outcome value, and (4) experience in dealing with eating disorders. Content validity was established by review from a national panel of experts. Reliability ranged from .66 to .73 for the subscales.
Results:
Although virtually all athletic trainers (91%) had dealt with a female athlete with an eating disorder, only 1 in 4 (27%) felt confident identifying a female athlete with an eating disorder, and only 1 in 3 (38%) felt confident asking an athlete if she had an eating disorder. One in 4 athletic trainers (25%) worked at an institution that did not have a policy on handling eating disorders. Almost all athletic trainers (93%) felt that increased attention needs to be paid to preventing eating disorders among collegiate female athletes.
Conclusions:
Collegiate athletic programs are encouraged to develop and implement eating-disorder policies. Continuing education on the prevention of eating disorders among athletes is also strongly recommended.
Keywords: collegiate issues, counseling, psychology, female athlete triad
Disordered eating behaviors include such conditions as anorexia nervosa, bulimia nervosa, and eating disorders not otherwise specified.1 The American Psychiatric Association1 stated that individuals must meet all of the following criteria for a proper diagnosis of anorexia nervosa to be made: “refusal to maintain body weight at or above a minimally normal weight for age and height (eg, weight loss leading to maintenance of body weight less than 85% of that expected); intense fear of gaining weight or becoming fat, even though underweight; disturbance in the way in which one's body weight or shape is experienced, undue influence of body weight or shape on self-evaluation, or denial of the seriousness of the current low body weight; in postmenarchal females, amenorrhea (ie, the absence of at least 3 consecutive menstrual cycles).” Regarding bulimia nervosa, individuals must meet all of the following criteria: “recurrent episodes of binge eating …; characterized by eating in a discrete amount of time, eating an amount of food that is definitely larger than most people would eat during a similar period of time and under similar circumstances, and having a sense of lack of control over eating during the episode; having recurrent inappropriate compensatory behaviors in order to prevent weight gain such as self-induced vomiting, misuse of laxatives, diuretics, enemas, or other medications, fasting, or excessive exercise.”1
Eating disorder not otherwise specified has been used to categorize all other disordered-eating behaviors that do not meet all of the criteria for anorexia nervosa or bulimia nervosa. Eating disorders affect 1% to 4% of all young women in the United States.1 The prevalence of eating disorders among college-aged individuals (18–22 years) is problematic and has dramatically increased during the past decade.2 Female athletes are up to 3 times more likely than female nonathletes to develop eating disorders.3 In the most recent National Collegiate Athletic Association (NCAA) study, 70% of responding institutions reported at least one case of an eating disorder, with 90% of those cases occurring in female sports,4 a significant increase from the same study conducted in 1990. Sports emphasizing leanness such as gymnastics, cross-country, swimming, and track and field tend to show the highest incidence of eating disorders.4,5
A collegiate athletic trainer's primary responsibility is to assist athletes in maintaining optimal health.6 Such a responsibility also includes identifying athletes with eating disorders, identifying athletes at risk, preventing the development of eating disorders, and intervening when necessary. If such steps are missed or overlooked, then athletes with eating disorders may not be identified and may, in turn, fail to receive the help they need.
In a comprehensive review of the literature, we found no published study that used Bandura's7 self-efficacy model to examine collegiate athletic trainers' perceived confidence in identifying athletes with eating disorders. Therefore, we examined the following research questions: (1) To what extent do collegiate athletic trainers believe they can identify female college athletes at risk for an eating disorder? (2) To what extent do collegiate athletic trainers believe that identifying female college athletes at risk for an eating disorder will reduce eating-disorders complications? and (3) What overall value do collegiate athletic trainers place on reducing female collegiate athletes' eating-disorders complications?
METHODS
Subjects
Participants in this study were head certified athletic trainers at NCAA Division IA and IAA institutions. All 236 institutions were sampled, and names and addresses were obtained through the National Athletic Trainers' Membership Directory 2000–2001.8
Instrumentation
We developed a 4-page, 53-item questionnaire using Bandura's7 self-efficacy model to examine athletic trainers' efficacy expectations, outcome expectations, and outcome values regarding female athletes with eating disorders. According to Bandura,7 efficacy expectation refers to the belief that one can successfully perform a specific behavior. Outcome expectation refers to the belief that if one successfully performs a specific behavior, it will lead to a desired result. Outcome value refers to the perceived importance of the desired result. In our study, efficacy expectation refers to athletic trainers' beliefs that they can effectively take specific steps to help athletes with eating disorders. Outcome expectation refers to athletic trainers' beliefs that performing specific steps will increase the chances the athlete will receive the help that he or she needs. Outcome value refers to athletic trainers' perceived importance in increasing the chances that athletes with eating disorders receive help.
The efficacy-expectation subscale consisted of 5 items, which required athletic trainers to respond using a 7-point Likert scale (1 = strongly disagree, 7 = strongly agree). Similarly, the outcome-expectation subscale consisted of 5 items, and the outcome-values subscale consisted of 4 items, each requiring the athletic trainers to respond using the same 7- point Likert scale.
To establish face and content validity, we developed the survey instrument based on a comprehensive review of the literature. After approval from the Human Subjects Committee at the University of Cincinnati, the survey was distributed to 2 athletic-training experts, 2 health-promotion experts, and 1 nutrition expert. Their recommendations were incorporated into the final instrument.
To assess stability reliability, a convenience sample of 15 certified athletic trainers received the survey instrument on 2 separate occasions 2 weeks apart. Intraclass correlation coefficients were computed for each of the 3 subscales: efficacy expectation (.64), outcome expectation (.74), and outcome value (.58). Internal consistency reliability of the survey was assessed via a series of Cronbach alphas: efficacy expectation (.66), outcome expectation (.60), and outcome value (.73).
Procedures
Participants received a signed cover letter describing the purpose of the study and assuring confidentiality, a copy of the survey instrument, and a self-addressed stamped envelope. A second mailing was sent to nonrespondents approximately 2 weeks after the initial mailing. Another signed cover letter, survey instrument, and self-addressed stamped envelope were included. All data analyses were performed using the SPSS statistical software package (version 10.1; SPSS Inc, Chicago, IL).
RESULTS
Of the 236 Division IA and IAA institutions, 11 institutions either did not identify their head athletic trainer or did not have an identifiable mailing address and were therefore omitted from this study. Two surveys were undeliverable because of incorrect mailing addresses. Overall, 171 surveys were returned, resulting in a 77% response rate (171 of 223).
The mean age of the athletic trainers was 36.9 years (SD = 10.0). The mean number of years employed as an athletic trainer was 15.2 (SD = 9.1), and the mean number of years working at the current institution was 10.9 (SD = 8.9). The mean number of students at an institution was 141 532.2 (SD = 10 383.1). Most of the athletic trainers responding were male (59%) and white (92%). Subject demographic and background characteristics are shown in Table 1. One third worked in an urban institution (38%), one third worked in a suburban institution (35%), and one fourth worked in a rural institution (27%). Although most (94%) reported they had never had an eating disorder, almost half (48%) reported having a friend with an eating disorder.
Table 1.
Demographic and Background Characteristics of Athletic Trainers*
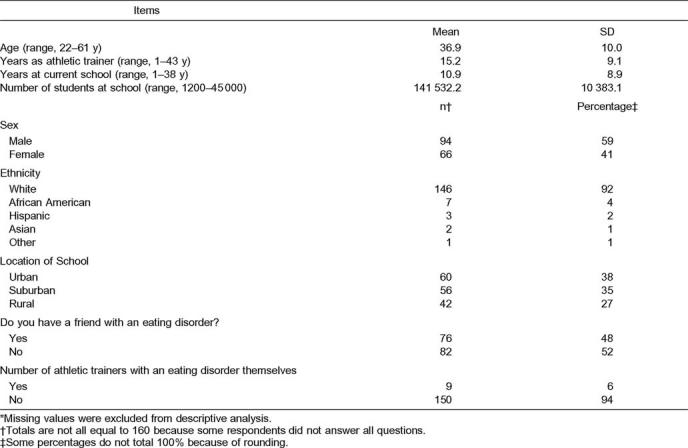
Most athletic trainers (n = 134, 84%) believed it was their role to identify female collegiate athletes at risk for an eating disorder. One in 4 (n = 40, 25%) worked at an institution that did not have a policy on handling eating disorders. More than half reported working at an institution that did not provide training or education on eating disorders to athletic trainers (n = 108, 69%) but did provide training or education to athletes. The overwhelming majority (n = 146, 91%) had dealt with an athlete with an eating disorder.
Demographic Interactions
We conducted analyses to test for potential interaction effects among demographic variables; χ2 analyses were performed for nonparametric demographic variables, whereas correlations and one-way analyses of variance were performed for parametric demographic variables. If these analyses showed significant interactions, then covariates were used during further analyses of the study. In this manner, potential confounding variables were controlled.
Efficacy Expectations Regarding Female Athletes With Eating Disorders
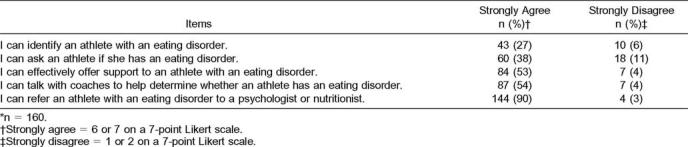
Only 27% of athletic trainers believed they could identify an athlete with an eating disorder, and 1 in 3 (38%) believed he or she could ask an athlete if she had an eating disorder (Table 2). Approximately one half (53%) stated they could effectively offer support to an athlete with an eating disorder, and 54% believed they could talk with coaches to help determine whether an athlete has an eating disorder. Most (90%) believed they could refer an athlete with an eating disorder to a psychologist or nutritionist.
Table 2.
Athletic Trainers' Efficacy Expectations Regarding Female Athletes With Eating Disorders*
We conducted multivariate analyses of variance and multivariate analyses of covariance (MANCOVAs) to examine the effects of the demographic and background variables on respondents' efficacy-expectation scores. These scores differed significantly based on whether the institution had a policy for handling eating disorders (F5,153 = 3.870, P < .05). More specifically, athletic trainers who worked at institutions with an eating-disorder policy were significantly more likely than athletic trainers who worked at an institution with no eating- disorder policy to feel confident identifying an athlete with an eating disorder (P = .002), talking to an athlete with an eating disorder (P = .036), asking an athlete whether she has an eating disorder (P = .034), effectively offering support (P = .018), and referring an athlete for professional help (P= .003).
Efficacy-expectation scores also differed significantly based on whether the athletic trainer was male or female (F5,148 = 2.28, P < .05). Female athletic trainers felt significantly more confident than male athletic trainers in identifying athletes with eating disorders (P = .034) and talking to athletes with eating disorders (P = .002). Whether an athletic trainer had dealt with an athlete with an eating disorder also significantly affected efficacy-expectation scores, (F5,157 = 2.38. P < .05). Athletic trainers who had dealt with an athlete with an eating disorder felt significantly more confident identifying an athlete with an eating disorder (P = .019) and referring an athlete with an eating disorder for professional help (P = .036) than athletic trainers who had not dealt with an athlete with an eating disorder.
Outcome Expectations Regarding Female Athletes With Eating Disorders
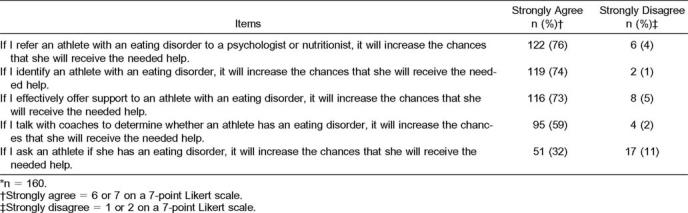
Most athletic trainers believed that referring an athlete at risk to a psychologist or nutritionist (76%), identifying an athlete at risk of an eating disorder (74%), and effectively offering support to an athlete at risk (73%) would increase the chances that the athlete would receive the needed help (Table 3). More than half (59%) believed that talking with coaches to determine whether an athlete had an eating disorder would increase the chances of that athlete receiving the needed help. However, only 32% felt that asking an athlete whether she had an eating disorder would increase the chances of receiving the needed help.
Table 3.
Athletic Trainers' Outcome Expectations Regarding Female Athletes With Eating Disorders*
The MANCOVAs were conducted to examine the effects of the demographic variables on athletic trainers' outcome-expectation scores. Outcome-expectation scores differed significantly based on whether the athletic trainer had had a friend with an eating disorder, (F5,152 = 2.26, P = .041). More specifically, athletic trainers who had had a friend with an eating disorder were more likely than athletic trainers who had not had a friend with an eating disorder to feel that talking with coaches to determine whether an athlete had an eating disorder would increase the chances that she would receive the needed help (P = .003). Outcome-expectation scores also varied significantly based on age (F10,302 = 2.38, P < .01). Athletic trainers age 30 years or younger were significantly more likely than older athletic trainers to feel that offering support to a female athlete would increase the chances that she would receive the needed help (P = .003).
Outcome Values Regarding Female Athletes With Eating Disorders
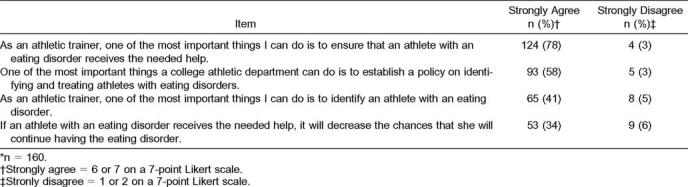
Most respondents believed that, as athletic trainers, one of the most important things they could do is to ensure that an athlete with an eating disorder receives the needed help (78%; Table 4). More than half (58%) of athletic trainers believed that one of the most important things a collegiate athletic department can do is to establish a policy on identifying and treating athletes with eating disorders (58%). More than one third (41%) believed that, as athletic trainers, one of the most important things they can do is to identify an athlete with an eating disorder, and 34% believed that if an athlete with an eating disorder receives the needed help, it will decrease the chances that she will continue having the eating disorder.
Table 4.
Athletic Trainers' Outcome Values Regarding Female Athletes With Eating Disorders*
The MANCOVAs were conducted to examine the effects of demographic variables on athletic trainers' outcome-values scores. Outcome-values scores differed significantly based on sex (F3,151 = 3.61, P = .015). More specifically, females were significantly more likely than males to believe that one of the most important things a collegiate athletic department can do is to establish a policy on identifying and treating athletes with eating disorders (P = .003) and that one of the most important things an athletic trainer can do is to identify an athlete with an eating disorder (P = .050).
DISCUSSION
We found that most of the athletic trainers felt it was their role to identify (78%) and help (97%) athletes with eating disorders. (These percentages are not found in any of the tables because they are not measures of efficacy expectation, outcome expectation, or outcome values. However, they were asked of all athletic trainers.) Yet only 1 in 4 (27%) felt effective in identifying an athlete with an eating disorder, and only 1 in 3 (38%) felt effective in asking an athlete if she had an eating disorder. Interestingly, female athletic trainers felt significantly more confident than male athletic trainers in identifying athletes with eating disorders. Females may feel more confident because eating disorders affect more females than males. Therefore, it is more likely that a female has had a friend with an eating disorder, resulting in increased confidence in identifying and helping athletes. Other possible factors explaining why females felt more confident may include a greater likelihood of their talking to other females about eating disorders and the issues involved with eating disorders, such as the loss of the menstrual cycle. In addition, female athletic trainers may be more amenable to, and more comfortable with, discussing emotional issues with female athletes.
Athletic trainers who work at institutions with an eating- disorder policy were also more confident in identifying eating disorders than athletic trainers who worked at institutions with no eating-disorder policy. Grandjean9 found that specific implementation of policies, procedures, and behaviors of athletic staff reduced the risk of eating disorders. Avoiding the emphasis on weight as a factor in athletic performance, encouraging proper dietary behaviors, and instituting private weigh- ins to reduce anxiety were all recommended actions.
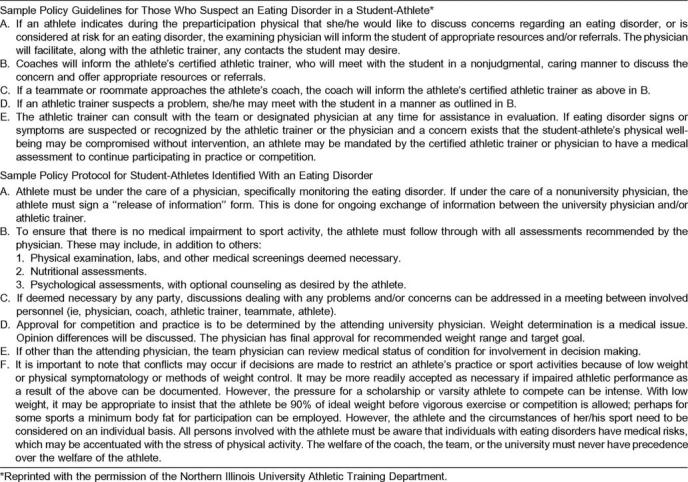
Several reasons may explain why having an institutional policy in place contributes to athletic trainers' increased confidence in identifying athletes with eating disorders. First, a policy provides a guideline that an athletic trainer can use as a reference tool. Second, an individual on staff likely created or helped to create the eating-disorder policy and therefore has some understanding of eating disorders. As a result, this person could be a resource for other athletic trainers. Also, with the development and implementation of an eating-disorder policy, the athletic staff may be more willing to review and discuss the issues of eating disorders. This may enhance athletic trainers' knowledge and awareness of the problem and increase their feelings of confidence in dealing with eating disorders. A sample policy on eating disorders is provided in Table 5, courtesy of Northern Illinois University.10
Table 5.
Sample Policy on Eating Disorders
The overwhelming majority of athletic trainers in this study (91%) reported dealing with an athlete with an eating disorder, and almost half (48%) of athletic trainers had a friend with an eating disorder. Having personally worked with an athlete with an eating disorder was associated with increased efficacy-expectation scores, and having a friend with an eating disorder was associated with increased outcome-expectation scores. Social cognitive theory supports these findings by asserting that individuals who have related experience to a behavior tend to successfully perform that behavior more often than individuals who have no related experience.7 Behavioral exposure and experience help to increase individuals' perceived confidence surrounding specific skills.
Age was also a significant factor affecting outcome-expectation scores. Athletic trainers 30 years and younger had increased outcome-expectation scores regarding eating disorders. Younger athletic trainers are closer to their academic coursework, having more recently graduated from college, and may therefore be more eager to help and intervene with athletes with problems such as eating disorders. Recent athletic training graduates are more likely to have received formal instruction regarding eating disorders than older graduates. Moreover, any information about eating disorders delivered in their coursework would still be fresh in their minds. In addition, society has become more open to discussions regarding the topic of eating disorders than in years past. Subsequently, younger athletic trainers may feel more comfortable talking about eating disorders and have a greater awareness that their role in identifying and providing help is critical toward resolving the problem.
CONCLUSIONS
We examined the confidence levels of athletic trainers in dealing with collegiate female athletes with eating disorders and offer several recommendations based on our findings. First, universities should develop and implement an eating- disorder policy for the institution. This would serve as a reference tool for athletic trainers and can help increase their confidence levels. Second, for athletic trainers to identify and offer support to athletes with eating disorders, education and training should be provided by universities and made available to all athletic trainers, coaches, and athletes. More training regarding this issue is clearly needed.11 Third, a registered dietitian should be on staff of all university athletic programs. If a dietitian cannot be on staff, one should be provided on campus and used as a reference and referral source for athletes. Athletic trainers are confident in referring athletes with an eating disorder, and having a consistent, known professional such as a counselor or psychologist to accept referrals may help as well. Psychological counseling is often needed to assist the athlete in resolving this condition.
Because female athletic trainers feel more confident in dealing with eating disorders than male athletic trainers, specific educational programs developed to help male athletic trainers may be beneficial. Ongoing discussion groups with female athletic trainers and female athletes may help to increase their overall confidence levels. Finally, having worked with an athlete with an eating disorder was found to increase confidence among athletic trainers. To help enhance confidence levels, mock situations involving eating disorders may prove useful.
In summary, we focused on the confidence levels of athletic trainers in dealing with collegiate female athletes having eating disorders. Eating-disorder policies have been shown to be a key factor in helping athletic trainers deal with athletes. Additional research is needed to examine the most effective policies and procedures toward eating-disorder prevention among female college athletes.
ACKNOWLEDGMENTS
We extend our gratitude to the University of Cincinnati College of Education for helping to fund this study through the 2000 Graduate Student Faculty Research Mentoring Grant.
REFERENCES
- 1.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Washington, DC: American Psychiatric Association; 1994. [Google Scholar]
- 2.Johnston CS, Christopher FS. Anorexic-like behaviors in dietetic majors and other student populations. J Nutr Educ. 1991;23:148–153. [Google Scholar]
- 3.Burckes-Miller M, Black DR. Male and female college athletes: prevalence of anorexia nervosa and bulimia nervosa. Athl Train JNATA. 1988;23:137–140. [Google Scholar]
- 4.Dick RW. Eating disorders in NCAA athletic programs: replication study of a 1990 study. NCAA Sport Sciences Education Newsletter. 1993 Apr 14;:3–4. [Google Scholar]
- 5.Smolak L, Murnen SK, Ruble AE. Female athletes and eating problems: a meta-analysis. Int J Eat Disord. 2000;27:371–380. doi: 10.1002/(sici)1098-108x(200005)27:4<371::aid-eat1>3.0.co;2-y. [DOI] [PubMed] [Google Scholar]
- 6.Arnheim DD, Prentice WE. Principles of Athletic Training. 10th ed. Boston, MA: McGraw-Hill Co, Inc; 2000. [Google Scholar]
- 7.Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84:191–215. doi: 10.1037//0033-295x.84.2.191. [DOI] [PubMed] [Google Scholar]
- 8.National Athletic Trainers' Association. National Athletic Trainers' Association Membership Directory 2000–2001. Timonium, MD: Dawson Publications; 2000. [Google Scholar]
- 9.Grandjean AC. Eating disorders: the role of the athletic trainer. J Athl Train. 1991;26:105–112. [Google Scholar]
- 10.Northern Illinois University. Policy Guidelines for Those Who Suspect an Eating Disorder in a Student Athlete. DeKalb, IL: Northern Illinois University; 2003. Northern Illinois University Athletic Training Department. [Google Scholar]
- 11.Turk JC, Prentice WE, Chappell S, Shields EW., Jr Collegiate coaches' knowledge of eating disorders. J Athl Train. 1999;34:19–24. [PMC free article] [PubMed] [Google Scholar]