

Abstract
Objective:
To present recommendations that decrease the risk of cervical spine fractures and dislocations in football players.
Background:
Axial loading of the cervical spine resulting from head-down contact is the primary cause of spinal cord injuries. Keeping the head up and initiating contact with the shoulder or chest decreases the risk of these injuries. The 1976 rule changes resulted in a dramatic decrease in catastrophic cervical spine injuries. However, the helmet-contact rules are rarely enforced and head-down contact still occurs frequently. Our recommendations are directed toward decreasing the incidence of head-down contact.
Recommendations:
Educate players, coaches, and officials that unintentional and intentional head-down contact can result in catastrophic injuries. Increase the time tacklers, ball carriers, and blockers spend practicing correct contact techniques. Improve the enforcement and understanding of the existing helmet-contact penalties.
Keywords: catastrophic injuries, cervical spine, head injuries, injury prevention, neck injuries, paralysis, quadriplegia
Catastrophic cervical spine injuries (CSIs) resulting in quadriplegia (paralysis of all 4 extremities) are among the most devastating injuries in all of sport. In football, the primary mechanism for these injuries is axial loading that occurs, whether intentional or unintentional, as a result of head-down contact and spearing. Head-first contact also increases the risk of concussion and closed head injury. In 1976, the National Collegiate Athletic Association (NCAA) and the National Federation of State High School Associations (NFSHSA) changed their football rules to broaden the concept of spearing to include any deliberate use of the helmet as the initial point of contact against an opponent. They did this in an effort to reduce the incidence of catastrophic CSIs.
Subsequent data on the occurrence of quadriplegia in organized football dramatically demonstrated that the NCAA and NFSHSA rule changes were successful. The incidence has remained at a relatively low level, with a mild increase at the end of the 1980s (Figure 1). However, in spite of this accomplishment, head-down contact still occurs frequently. The helmet-contact penalties also are not enforced adequately. Clearly, a reduction in the incidence of head-down contact and increased enforcement of the existing rules will further reduce the risk of both paralytic and nonparalytic injuries.
Figure 1.

Incidence of quadriplegia in high school and college athletes. Data from the National Football Head and Neck Injury Registry (1976–1991) and the National Center for Catastrophic Sports Injury Research (1992–present).1–4
The purpose of this position statement is to (1) provide scientifically proven concepts and recommendations to minimize the risk of catastrophic CSIs in football; (2) clarify that head- down contact and spearing pose a risk to all positional players regardless of intent; (3) establish the value and necessity of ongoing educational practices for players, coaches, and officials regarding dangerous and proper playing techniques; and (4) emphasize that increasing safety depends on the participation of sports medicine professionals, coaches, players, officials, administrators, and governing bodies.
RECOMMENDATIONS
The National Athletic Trainers' Association (NATA) recommends the following regarding head-down contact and spearing in football. These recommendations should be considered by sports medicine professionals, coaches, players, officials, administrators, and governing bodies who work with athletes at risk for cervical spine injuries.
Practices and Concepts
Axial loading is the primary mechanism for catastrophic CSI. Head-down contact, defined as initiating contact with the top or crown of the helmet, is the only technique that results in axial loading.
Spearing is the intentional use of a head-down contact technique. Unintentional head-down contact is the inadvertent dropping of the head just before contact. Both head-down techniques are dangerous and may result in axial loading of the cervical spine and catastrophic injury (Figure 2).
Catastrophic CSI resulting from axial loading is neither caused nor prevented by players' standard equipment.
Injuries that occur as a result of head-down contact are technique related and are preventable to the extent that head-down contact is preventable.
Attempts to determine a player's intent regarding intentional or unintentional head-down contact are subjective. Therefore, coaching, officiating, and playing techniques must focus on decreasing all head-down contact, regardless of intent.
Catastrophic CSI occurs most often to defensive players. However, all players are at risk. Ball carriers and blockers have also become quadriplegics by lowering their heads at contact. Expanding the concept of head-down contact beyond tackler spearing and the “intentional attempt to punish an opponent” will decrease the risk of serious injury to players in other positions.
As emphasized in the college and high school rule books, making contact with the shoulder or chest while keeping the head up greatly reduces the risk of serious head and neck injury. With the head up, the player can see when and how impact is about to occur and can prepare the neck musculature for impact. Even if inadvertent head-first contact is made, then the force is absorbed by the neck musculature, the intervertebral discs, and the cervical facet joints. This is the safest contact technique.
Each time a player initiates contact with his head down, he risks paralysis. Therefore, increased attention to the frequency of head-down contact occurring in games and practices is needed. It is a reasonable conclusion that a reduction in the cause (head-down contact) will further reduce the effect (catastrophic CSI).
Data collection on all catastrophic CSIs is important. Attention to the number of nonparalytic cervical spine fractures and dislocations is needed, as each incident has the potential for paralysis. These data are less reliable and harder to obtain than data for paralytic injuries. Both injury types require diligent reporting to the National Center for Catastrophic Sports Injury Research (mailing address: CB 8700, 204 Fetzer Gymnasium, University of North Carolina, Chapel Hill, NC 27599-8700, mueller@email.unc.edu).
Figure 2.

Head-down contact poses significant risks of catastrophic cervical spine injury. This defensive back (dark jersey) sustained fractures of his 4th, 5th, and 6th cervical vertebrae. The hit resulted in quadriplegia.
Rules and Officiating
Officials should enforce the existing rules to further reduce the incidence of head-down contact. A clear discrepancy exists between the incidence of head-down/head-first contact and the level of enforcement of the helmet-contact penalties. Stricter officiating would bring more awareness to coaches and players about the effects of head-down contact.
The current annual education programs for all officials should emphasize the purpose of the helmet-contact rules and the dangers associated with head-down/head-first contact. Emphasis should be on the fact that the primary purpose of the helmet-contact penalties is to protect the athlete who leads with his head. Although the technique is dangerous to both players, it is the athlete who initiates head-down contact who risks permanent quadriplegia.
Not all head-first contacts that result in serious injury are intentional. A major area of concern for officials remains application of the penalties to athletes who unintentionally initiate contact with their helmets. Athletic governing bodies should address this issue in order to improve penalty enforcement.
Athletic governing bodies should coordinate a protocol to document and quantify all penalties called through their organizations. This will identify the enforcement level of the helmet-contact penalties.
Athletic governing bodies should periodically survey their football officials regarding their interpretations and perceptions of the helmet-contact rules. Existing rules and comments need to specifically include the ball carrier in the application of these penalties.
Those preparing the football rule books should consider revising the wording “blocking and tackling techniques” with “contact techniques” (or similar). This revised wording would then include all position players and all types of contact.
A task force of athletic trainers, coaches, team physicians, officials, and league administrators should be developed at all levels of play to monitor rule enforcement and the frequency of head-down contact by an annual, random review of game films.
Education and Coaching
The athlete should know, understand, and appreciate the risk of making head-down contact, regardless of intent. Formal team educational sessions (conducted by the athletic trainer or team physician or both with the support of the coaching staff) should be held at least twice per season. One session should be conducted before contact begins and the other at the midpoint of the season. Parents should be invited to the first educational session at the high school level. Recommended topics are mechanisms of head and neck injuries, related rules and penalties, the incidence of catastrophic injury, the severity and prognosis of these injuries, and the safest contact positions. The use of videos such as Prevent Paralysis: Don't Hit With Your Head,5 See What You Hit,6 or the prevention portion of Spine Injury Management7 should be mandatory (Table 1). The use of supplemental media and materials are strongly recommended.
Correct contact technique should be taught at the earliest organized level. Pop Warner, Midget, and Pee Wee football leagues should perpetually emphasize the importance of coaching and teaching heads-up football.
It is crucial that educational programs extend to the television, radio, and print media for both local and national affiliates regarding the dangers of head-down contact and the reasons for the helmet-contact rules. This will promote awareness of these issues and provide extended education to viewers, listeners, and readers.
Initiating contact with the shoulder/chest while keeping the head up is the safest way to play football. The game can be played aggressively with this technique with much less risk of serious injury (Figure 3). However, it is a technique that must be learned. To be learned, it must be practiced extensively. Athletes who still drop their head just before contact require additional practice time. It is imperative for coaches to teach, demonstrate, and practice this technique throughout the year for all position players. Specific emphasis should be placed on contact techniques at least 4 times spread over the entire season. Tacklers, ball carriers, and blockers must receive practice time until it is instinctive to keep the head up.
Initiating contact with the face mask is a rules violation and must not be taught. If the athlete uses poor technique by lowering his head, he places himself in the head-down position and at risk of serious injury.
Every coaching staff must display and implement a clear philosophy regarding the reduction of head-down contact. The head coach should clearly convey this philosophy to the assistant coaches and the entire team and pursue an enforcement policy during practice. A player's technique must be corrected anytime he is observed lowering his head at contact. Coaches should also use weekly game film reviews to provide players with feedback about their head positions.
Athletes should have a year-round supervised neck- strengthening program with appropriate equipment and techniques. Although the role of strength training is secondary to correcting contact technique in axial-loading injury prevention, it provides the strength and endurance required to maintain the neck in extension. It also provides protection against cervical nerve root neurapraxia (burners).
Schools, responsible administrators, and the sports medicine team should recognize cyclic turnover in coaches and establish programs that educate new and re-educate existing coaches to appropriate teaching and practicing methods. This will provide a documented and consistent approach to the prevention of these injuries.
Table 1.
Available Videos
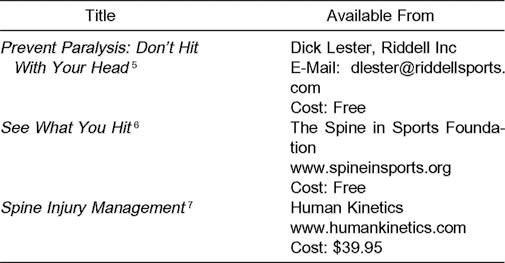
Figure 3.

Initiating contact with the shoulder while keeping the head up reduces the risk of catastrophic injury, as demonstrated by the blocker and potential tackler.
HISTORY AND BACKGROUND
In 1931, the American Football Coaches Association compiled the first Football Fatality Report.8 By 1962, its findings caused the American Medical Association Committee on Medical Aspects of Sports to host a national conference on head protection for athletes.8 The conference convened the principal authorities of that era in what was emerging as “sports medicine” to discuss the current issues involving changes in the football helmet and the advent of the football face mask. The focus was the rapidly rising fatality rate among high school and college football players suffering from closed head injuries. Football authorities were divided as to whether the new protective headgear was good for the sport.
Into the 1970s, opinion was more prevalent than scientific data in addressing these problems. The American Medical Association Committee arrived at a collective expert opinion and encouraged pragmatic scholarly attention to the health and safety issues within sport. Among the recommendations resulting from the 1962 conference were condemning the practice of spearing and the need for research to develop standards for football helmets.9 Initially, spearing was defined by rule as “intentionally and maliciously striking the opponent with one's helmet after the opponent had been downed.”
After the 1962 conference, Blyth from the University of North Carolina assumed the data collection for the Fatality Report of the America Football Coaches Association.10 Helmet manufacturers began to sponsor research on impact standards for helmets, and high school and college rules committees confirmed that spearing was an illegal form of football contact after the whistle.
American Medical Association Position Statement
The practice of teaching “face into the numbers” was growing in the 1960s as the helmets evolved and coaches felt that players could therefore better withstand the use of the helmeted head.8,11,12 “Face into the numbers” was increasingly popular, because it allowed the blocker or tackler to keep his eyes forward and neck “bulled” and to move with the opponent, without having the intent to spear.8 In essence, coaches considered using the helmet as the primary point of contact a superior technique.
In 1967, however, the American Medical Association Committee on Medical Aspects of Sports declared, in a groundbreaking position statement, its opinion that most spearing was unintentional and non-malicious, ie, “inadvertent.”11 It identified the flaw with teaching “face-into-the-numbers” contact. Athletes do not always execute with precision, and the tendency to duck the head at contact is natural. This position statement was adopted by the NFSHSA as a joint statement in 1968.
Football Helmet Standards
In spite of this timely recognition of unsafe head position, the annual football fatality data reports revealed a continued rise in frequency during the 1960s.10 Although it was reported that the risk of death from football did not exceed the actuarial risk of death among males of that age in non-football activities,13 the need for helmet design standards became more and more evident.
Consequently, the helmet manufacturers agreed in 1969 to pool their resources through a newly devised interdisciplinary National Operating Committee for Safety in Athletic Equipment (NOCSAE).8 This committee was charged with the development of consensus standards for helmets in football by an independent investigator. Hodgson, from Wayne State University, was selected as the investigator because of his extensive research in this area.14 A safety standard was achieved in 1973, and the first helmets were tested on the NOCSAE standard in 1974.12 The NOCSAE standards went into effect for colleges in 1978 and for high schools in 1980.15 It was commonly understood that the helmets being produced and used by the mid-1970s met the NOCSAE standards, and all helmets being worn were, in fact, associated with the same low rates of clinical concussions.16
The increase in head injury fatalities throughout the 1960s and early 1970s was attributed to the introduction of hardshell helmets and face masks in the early 1960s, which resulted in playing techniques that increased exposure of the head to contact.1,8 Helmet standards and head injuries received football's priority attention during this time.8 Similar attention to serious neck injuries in the 1960s was lacking because the incidence of nonfatal quadriplegia was not being tracked and therefore was unknown.
Catastrophic Injury Data
The Annual Football Fatality Report was the only ongoing source of data into the 1970s. Schneider17 included serious neck injuries in his landmark survey of catastrophic injuries in football in the early 1960s. But it was not until the mid- 1970s that 2 concurrent and independent studies by Clarke18 and Torg et al19,20 again examined quadriplegia. These data revealed the increased incidence of paralyzed football players.
The total number of head and neck injuries from 1971 to 197519,20 was calculated and retrospectively compared with the data from 1959 to 1963 compiled by Schneider.17 The number of intracranial hemorrhages and deaths had decreased by 66% and 42%, respectively. This suggested that the new helmet standards had been effective in minimizing serious head injuries. However, the number of cervical spine fractures, subluxations, and dislocations had increased by 204%, and the number of athletes with cervical quadriplegia had increased by 116%.
Clarke and Torg led the proponents of the spearing rule changes that were implemented by the NFSHSA and NCAA in 1976. These rule changes preceded the publication of their data.18–20 The purpose of the rule changes was to protect the spearer, whether inadvertent or intentional, from neurotrauma.5,8,11,12,15,21–25 On the basis of these data, it was concluded that the improved protective capabilities of the polycarbonate helmets accounted for a decrease in head injuries but encouraged playing techniques that used the top or crown of the helmet as the initial point of contact and put the cervical spine at risk.1
The results of the 1976 rule change are an example of one of the most successful injury interventions in sport (Figures 1 and 4). In the first year after the rule change, the number of injuries resulting in quadriplegia in high school and college players decreased by 53%.1 By 1984, the number dropped by 87%. Other than increases in 1988, 1989, and 1990 to the low teens, these cases have remained in the single digits through the most recent years of available data. This decrease is attributed to the rule change and to improved coaching techniques at the high school and college levels.8,12,15,19,23,24,26–34
Figure 4.

Incidence of cervical fractures and dislocations in high school athletes. Data from the National Football Head and Neck Injury Registry.
In order to track nonfatal catastrophic injuries, Torg et al1 established the National Football Head and Neck Injury Registry in 1975, which collected data on CSIs through the early 1990s. In 1977, the NCAA initiated funding for a National Survey of Catastrophic Injuries directed by Mueller and Blyth.2–4 In 1982, this project was expanded to include all sports and renamed the National Center for Catastrophic Sports Injury Research. Both projects used similar methods of collecting data. These sources included coaches, school administrators, medical personnel, athletic organizations, a national newspaper-clipping service, and professional associates. The collection of these data was crucial in preventing catastrophic injuries.12
In 1987, a joint endeavor was initiated between the National Center for Catastrophic Sports Injury Research and the section on Sports Medicine of the American Association of Neurological Surgeons. As a result, Cantu became responsible for monitoring the collected medical data.2 This project continues to collect data on these injuries.
Mechanism of Injury
In the early 1970s, several theories existed regarding the mechanisms of CSIs and quadriplegia. The theories of hyperflexion and hyperextension, based on postinjury radiographs, were considered 2 primary causes.1 Forced hyperflexion was considered a primary cause of severe CSI in football and other sports.1,35–57 Hyperextension and the concept of the posterior rim of the helmet acting as a guillotine also received attention as an injury mechanism.58–62 Both of these injury mechanisms received acceptance throughout the 1970s.
In contrast to these early theories, Torg et al19,20 determined that most cases of permanent quadriplegia occurring between 1971 and 1975 were due to head-down contact or direct compression to the cervical spine. This resulted from the player initiating contact with the top of his helmet. The direct-compression or axial-loading concept eventually replaced the numerous other inaccurate, theoretic mechanisms of CSI. The identification of an accurate mechanism of injury was vitally important to the prevention of these injuries.12,30 This allowed the development of a precise plan to reduce the incidence of quadriplegia.8 Axial loading is now accepted as the primary cause of cervical-spine fracture and dislocation in football. Numerous studies have supported the role of axial loading20,63–97 in catastrophic CSI and refuted the role of hyperflexion and hyperextension in these injuries.1,19,23,24,30–32,63–65,68,72,94,98,99
Axial Loading
In the course of contact activity, such as football, the cervical spine is repeatedly exposed to dangerous energy inputs.93 Fortunately, most forces are dissipated by controlled spinal motion through the cervical paravertebral muscles, eccentric contractions, and intervertebral discs.19 However, the vertebrae, intervertebral discs, and supporting ligamentous structures can be injured when contact occurs on the top or crown of the helmet with the head, neck, and trunk positioned in such a way that forces are transmitted along the vertical axis of the cervical spine. In this situation, the cervical spine can assume the characteristics of a segmented column. With the neck in the neutral position, the cervical spine is extended as a result of normal cervical lordosis (Figure 5). When the neck is flexed to 30°, the cervical spine becomes straight. When a force is applied to the vertex, the energy is transmitted along the longitudinal axis of the cervical spine and is no longer dissipated by the paravertebral muscles. This results in the cervical spine being compressed between the abruptly decelerated head and the force of the oncoming trunk.65 Essentially, the head is stopped, the trunk keeps moving, and the spine is crushed between the two. When maximum vertical compression is reached, the cervical spine fails in a flexion mode, with a fracture, subluxation, or facet dislocation resulting.63 In the laboratory, fracture or dislocation has occurred with less than 150 ft-lb of kinetic energy.28 A running football player can possess 1500 ft-lb of kinetic energy.28
Figure 5.

(A) Axial loading of the cervical spine (B) first results in compressive deformation of the intervertebral discs. As the energy input continues and maximum compressive deformation is reached, angular deformation and buckling occur (C). The spine fails in a flexion mode, with resulting fracture, dislocation, or subluxation (D and E).
Distribution of Serious Injuries
Defensive football players receive the majority of fatalities and catastrophic CSIs, accounting for approximately 4 times those of offensive players.2–4,12,15,19,20,23 Tackling is the leading cause, followed by being tackled and then blocking.2–4,12,15 By position, defensive backs and special teams players are at the greatest risk2,3,12,15,16,19,23 with ball-carrier positions, linebackers, and defensive linemen having the next highest incidences of serious injury.2,12,15
Each time a player initiates contact with his head down, he risks quadriplegia.2,15,19,22–25,27–33,97,100–106 Each time an athlete initiates contact head first, he increases the risk of concussion.22,29,101–103,107,108 Although catastrophic injuries have occurred to position players at various rates, mechanism of injury does not discriminate by position or intent.103,105,107,109 Head-down contact poses a risk to every player who employs this technique.22,103–105
Incidence of Head-Down Contact
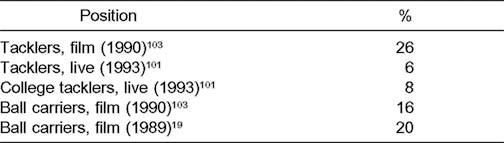
According to Hodgson and Thomas,28 the number of paralyzed players does not accurately identify the risk of hitting with the head down. Because of the decrease in catastrophic injuries since the 1976 rule changes, it is often assumed that head-down contact rarely occurs. Two authors have examined the incidence of head-down contact in the 1990s:22,101,103 twice on film in slow motion and once in live situations. Selected data appear in Tables 2 and 3.
Table 2.
Percentage of Plays Involving at Least 1 Head-Down Contact Between Tacklers and Ball Carriers During a 1990 High School Season103
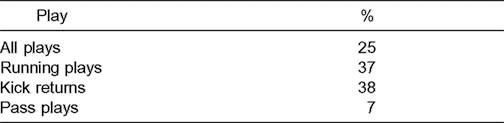
Table 3.
Percentage of Plays Involving Head-Down Contact by High School and College Tacklers or Ball Carriers
One study compared the incidence of head-down contact between tacklers and ball carriers before and after the rule change on the high school level.103 No significant change was seen in the incidence of head-down contact between the seasons. Approximately 20 head-down contacts occurred per team in a single game. There was 1 head-down contact for every 1.8 kick returns. Special teams' players have been among the leading position players associated with catastrophic injuries. Considering that kicking plays account for only about 7% of the plays involving a ball carrier, this play is probably the most dangerous play in football.
Ball-carrier spearing (Figure 6) is interesting in that defensive players were 4 times more likely to hit with their head down when tackling a head-down ball carrier. It is possible that a head-down ball carrier influences a tackler to “get lower” and use a similar technique.22,103 This coincides well with Drake's101,102 finding that tacklers were 3 times more likely to make head-down contact when tackling below the waist.
Figure 6.

Ball-carrier head-down contact, an often overlooked danger, increases the risk of head and neck injuries.
During the 1990 season, 200 head-down contacts occurred during one team's season, and an estimated 2.8 million head- down contacts took place nationally between tacklers and ball carriers on the high school level. This translated into approximately 1 case of quadriplegia for every 251 000 head-down contacts. Based upon these numbers, a high school should have 1 case of quadriplegia for every 11 000 games.103 Although these numbers are rough estimates at best, they demonstrate the room for additional improvement in decreasing the incidence of spearing and head-down contact.
Rules and Officiating
The current helmet-contact rules for high school and college are shown in Tables 4 and 5, respectively. In 1976, the high school rule change defined butt blocking and face tackling and made them illegal. It was also a “point of emphasis” that coaches could no longer teach “face in the numbers” as a contact technique.112 On the collegiate level, the rules were adapted to make “deliberate” use of the helmet illegal. Also, the rule book included a “Coaching Ethics” statement from the American Football Coaches Association that the helmet cannot be used as a primary point of contact in the teaching of blocking and tackling.113 Since 1976, 2 significant changes to the helmet-contact rules have been made. First, in the mid- 1980s, the spearing penalty was lessened from an automatic ejection to a 15-yard penalty. Second, in the early 1990s, the NCAA made the face mask an official part of the helmet.
Table 4.
Helmet-Contact Rules and Selected Comments from the 2002 National Federation of State High School Associations' Official Football Rules110
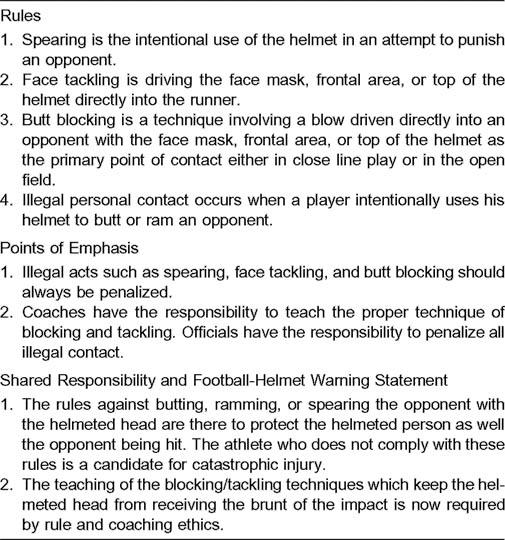
Table 5.
Helmet-Contact Rules and Comments in the National Collegiate Athletic Association's 2001 Football Rules and Interpretations111
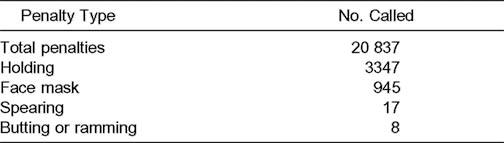
Although the rule change is credited with reducing catastrophic injuries, the role officials have played by enforcing these rules is questionable (Table 6). To illustrate this, in 2001, college officials called 1 spearing penalty in every 73 games and 1 butting or ramming penalty in every 156 games. No spearing penalties were called in 12 of the 20 major Division 1 conferences.114 During the 1992 NCAA season, officials called 55 spearing penalties (1 in every 21 games) and 16 related to butting or ramming.115
Table 6.
Selected 2001 National Collegiate Athletic Association Penalty-Enforcement Data from Major Division 1 Conferences114
On the high school level, officials called an estimated 1 spearing penalty in every 20 games.116 During one team's high school season, no spearing penalties were called.20 This appears to be the norm rather than the exception. These data contradict the NFSHSA recommendation that infractions involving a safety issue should always be enforced.110,117 At this level of enforcement, it is doubtful whether actual penalties have decreased the incidence of head-down contact or the mechanism of injury.116 If illegal helmet contact is not penalized, the message is sent that the technique is acceptable.118 Adequate enforcement of the rules will clearly further reduce the risk of catastrophic injuries.4,12,15,21–23,29–31,101,102,106,115
Surveys of football officials have revealed many inconsistencies with regard to the helmet-contact penalties. Football officials may not have a uniform understanding of these rules. Fifty percent of New Jersey officials felt that all head-first contact was illegal.116 Thirty-two percent felt that the rules were difficult to interpret.116 Another 38% were unsure whether the rules were written in a way that allowed easy enforcement.116 A survey of college officials found similar results regarding the wording of the rules.115 A large number of high school and college officials believed that determining an athlete's intent made the rules difficult to enforce.
The helmet-contact penalties are unique in football because they are the only action penalties that penalize a player for his own protection.105,109 However, many officials and coaches erroneously perceive the primary purpose of the penalties as protecting the athlete who gets hit.105,109,115,116 This is reflected by one group's findings that nearly one third of high school players did not know that it was illegal to tackle with the top of the helmet or run over an opponent head first.119
Despite the intent of the 1976 rule change to address unintentional or inadvertent spearing, the primary rule still has an association with the “intentional attempt to punish.” The wording of the helmet-contact rules does imply the need for intent.116 On the college level, the rules do not address unintentional head-down contact at all. High school rules do address head-down contact through the penalties for face tackling and butt blocking; however, these rules exclude mention of the ball carrier. Although rules do exist at the high school level, officials may enforce them even less than they enforce the spearing penalty.116,120 Football's objective should be to alter athlete behavior to eliminate head-down contact, not merely to discourage it.121
An appropriate inquiry, which cannot be answered, is, “How many of the approximately 200+ hits resulting in paralysis were flagged at the time of contact?” Although a penalty flag on a play that involves a head or neck injury cannot prevent that injury, it may prevent one later on.120 In reviewing the video Prevent Paralysis: Don't Hit With Your Head, football officials did not feel that the rules allowed them to penalize the majority of the hits demonstrated on this film that resulted in quadriplegia.122 A “litmus test” for the enforcement of the helmet-contact rules is their application to actual hits that have resulted in paralysis. There is no better definition of the type of contact that we must eliminate.
Safest Contact Position
Initiating contact with the shoulder while keeping the head up is the safest contact position.2–4,11,12,15,22,28,49,103,110,123 With the head up, the athlete can see when and how impact is about to occur and can prepare the neck musculature. This information applies to all position players, including ball carriers. The game can be played just as aggressively with this technique with much less risk of serious injury. Tacklers can still “unload” a big hit, and ball carriers can still break tackles.105,109
Conversely, with the head down, the athlete does not have the advantage of good vision and preparation for the instant of contact. He is likely to receive the full force of the impact on the head instead of the shoulders, chest, or arm. He is more apt to hit low on the opponent's body (including the opponent's hard-driving knees), and exposes his cervical spine to impact in its most vulnerable position.11 Albright et al124 found that college and high school players had sufficient nonfatal CSIs to warrant concern over the teaching of head-butting techniques.
Coaches have expressed that they have taught players to tackle correctly, but the players still have a tendency to lower their heads just before contact.15,28 It seems that players have learned to approach contact with their head up, but they need to maintain this position during contact.103–105,109 It is instinctive for players to protect their eyes and face from injury by lowering their heads at impact.22,103–105,109 Coaches must spend enough practice time to overcome this instinct. Players who drop their heads at the last instant are demonstrating that they need additional practice time with correct contact techniques in game-like situations. In addition to teaching correct contact in the beginning of the season, coaches should put specific emphasis on this 3 more times throughout the season.21,22,104
The “See What You Hit” concept has gained popularity in recent years. It is intended to teach athletes to keep their heads up and can be an effective tool. However, caution is required to ensure that coaches and athletes do not misinterpret this slogan as support for initiating contact with the face mask.
Strengthening the neck musculature is an accepted part of neck-injury prevention.15,29,49,97,100 Although such strengthening cannot prevent axial loading in the head-down position, it can help athletes keep the head up during contact. Athletes should have access to some type of neck-strengthening equipment, and, ideally, the program should be year round. If this is not possible, then adequate time (4 to 6 weeks before the season begins) should be allowed for strength gains. During the season, athletes should continue to lift at least 1 day per week to maintain their strength levels.125
Litigation
The occurrence of a catastrophic head or neck injury is characteristically accompanied by litigation.126–140 The proliferation of litigation for these injuries began in the 1980s. Multimillion-dollar verdicts are now common. Of the $45.8 million awarded in verdicts between 1970 and 1985, $38.7 million was awarded between 1980 and 1985.126,127 Ironically, the litigation in football is inversely proportional to the injury statistics. During the time when there was a drastic decrease in catastrophic injuries, litigation increased.126 Any allegation of fault can have devastating financial consequences for school districts, coaches, medical personnel, and equipment manufacturers.
The increase in litigation had serious effects on the football helmet industry. Between 1975 and 1985, 11 of 14 football helmet manufacturers left the marketplace.126 This exit from the marketplace was due to the cost of defending product liability claims126 and not to shortcomings regarding the NOCSAE helmet standards. Dramatic increases in liability insurance premiums followed the increase in litigation. At that point, many helmet manufacturers became self-insured or accepted the risk of being underinsured. Approximately 40% of the helmet price was set aside for product liability.126 Litigation will continue, and medical practitioners will have to determine, as the helmet manufacturers did, if they can afford to work in athletics.126 For these individuals and others, the implications of the increase in the number of athletic-injury lawsuits are obvious. The chance of being named in a lawsuit is significantly increased, regardless of fault or their role in the injury.126,127,139
Many steps can be taken to decrease the risk of catastrophic injuries and being found at fault for these injuries.104,123,127,140 A top priority is to ensure players know, understand, and appreciate the risks of making head-first contact in football.8,104,140 The videos Prevent Paralysis: Don't Hit with Your Head”5 and See What You Hit6 and the prevention section of Spine Injury Management7 are excellent education tools. Parents of high school players should also be given the opportunity to view at least one of these videos. Coaches have a responsibility to spend adequate time teaching and practicing correct contact techniques with all position players. Everyone associated with football has a moral and legal responsibility to do all in their power to attempt to eliminate head-down contact from the sport.104,105,109,140
ACKNOWLEDGMENTS
We gratefully acknowledge the efforts of Douglas M. Kleiner, PhD, ATC/L, CSCS, FACSM; Frederick O. Mueller, PhD; Robert G. Watkins, MD; and the Pronouncements Committee in the preparation of this document.
DISCLAIMER
NATA publishes its position statements as a service to promote the awareness of certain issues to its members. The information contained in the position statements is neither exhaustive nor exclusive to all circumstances or individuals. Variables such as institutional human resource guidelines, state or federal statutes, rules, or regulations, as well as regional environmental conditions, may impact the efficacy and/or reliability of these statements. NATA advises individuals to carefully and independently investigate each of its position statements (including the applicability of same to any particular circumstance or individual) and states that such position statements should not be relied upon as an independent basis for treatment but rather as a resource available to its members. Moreover, no opinion is expressed herein regarding the quality of treatment that adheres to or differs from NATA's position statements. NATA reserves the right to rescind or modify its position statements at any time.
REFERENCES
- 1.Torg JS, Guille JT, Jaffe S. Injuries to the cervical spine in American football players. J Bone Joint Surg Am. 2002;84:112–122. doi: 10.2106/00004623-200201000-00017. [DOI] [PubMed] [Google Scholar]
- 2.Mueller FO, Cantu RC. Annual survey of catastrophic football injuries: 1977–1992. In: Hoerner EF, editor. Head and Neck Injuries in Sports ASTM STP 1229. Philadelphia, PA: American Society for Testing and Materials; 1994. pp. 20–27. [Google Scholar]
- 3.Mueller FO, Cantu RC. The annual survey of catastrophic football injuries: 1977–1988. Exerc Sport Sci Rev. 1991;19:261–312. [PubMed] [Google Scholar]
- 4.Cantu RC, Mueller FO. Catastrophic football injuries: 1977–1998. Neurosurgery. 2000;47:673–675. doi: 10.1097/00006123-200009000-00029. [DOI] [PubMed] [Google Scholar]
- 5.Torg JS. Prevent Paralysis: Don't Hit With Your Head [videotape] Philadelphia, PA: Penn Sports Medicine; 1992. [Google Scholar]
- 6.See What You Hit [videotape] Atlanta, GA: Kestrel Communications Inc; 2000. [Google Scholar]
- 7.Spine Injury Management [videotape] Champaign, IL: Human Kinetics; 2001. [Google Scholar]
- 8.Clarke KS. Cornerstones for future directions in head/neck injury prevention in sports. In: Hoerner EF, editor. Head and Neck Injuries in Sports ASTM STP 1229. Philadelphia, PA: American Society for Testing and Materials; 1994. pp. 3–9. [Google Scholar]
- 9.Hard-shelled helmets for athletes, experts say. JAMA. 1962;180:23–24. [Google Scholar]
- 10.Blyth C, Arnold D. The Thirty-Ninth Annual Survey of Football Fatalities,1931–1970. Chicago, IL: American Football Coaches Association, National Collegiate Athletic Association, and National Federation of State High School Associations; 1978. [Google Scholar]
- 11.American Medical Association Committee on Medical Aspects of Sports. Spearing in Football: Tips on Athletic Training. Chicago, IL: American Medical Association, National Federation of State High School Athletic Associations; 1968. pp. 6–7. [Google Scholar]
- 12.Mueller FO, Blyth CS. Fatalities from head and cervical spine injuries occurring in tackle football: 40 years' experience. Clin Sports Med. 1987;6:185–196. [PubMed] [Google Scholar]
- 13.Clarke KS. Calculated risk of sports fatalities. JAMA. 1966;197:894–896. [PubMed] [Google Scholar]
- 14.Hodgson V. National Operating Committee on Standards for Athletic Equipment Football Certification Program. Available at: http://www.nocsae.org/nocsae/RESEARCH/Hodgson.htm. Accessed September 23, 2002. [PubMed]
- 15.Mueller FO, Blyth CS, Cantu RC. Catastrophic spine injuries in football. Physician Sportsmed. 1989;17(10):51–53. doi: 10.1080/00913847.1989.11709888. [DOI] [PubMed] [Google Scholar]
- 16.Clarke KS, Powell JW. Football helmets and neurotrauma: an epidemiological overview of three seasons. Med Sci Sports. 1979;11:138–145. [PubMed] [Google Scholar]
- 17.Schneider RC. Serious and fatal neurosurgical football injuries. Clin Neurosurg. 1964;12:226–236. doi: 10.1093/neurosurgery/12.cn_suppl_1.226. [DOI] [PubMed] [Google Scholar]
- 18.Clarke KS. A survey of sport-related spinal cord injuries in schools and colleges, 1973–1975. J Safety Res. 1977;9:140–146. [Google Scholar]
- 19.Torg JS, Quedenfeld TC, Moyer RA, Truex R, Spealman AD, Nichols CE. Severe and catastrophic neck injuries resulting from tackle football. J Am Coll Health Assoc. 1977;25:224–226. [PubMed] [Google Scholar]
- 20.Torg JS, Truex R, Jr, Quedenfeld TC, Burstein A, Spealman A, Nichols CE., III The National Football Head and Neck Injury Registry: report and conclusions, 1978. JAMA. 1979;241:1477–1479. [PubMed] [Google Scholar]
- 21.Heck JF. An analysis of football's spearing rules. Sideliner J Athl Train Soc N J. 1993;9:8,9,15. [Google Scholar]
- 22.Heck JF. The incidence of spearing by high school football ball carriers and their tacklers. J Athl Train. 1992;27:120–124. [PMC free article] [PubMed] [Google Scholar]
- 23.Torg JS, Vegso JJ, Sennett B. The National Football Head And Neck Injury Registry: 14-year report on cervical quadriplegia. Clin Sports Med. 1987;6:61–72. [PubMed] [Google Scholar]
- 24.Torg JS, Sennett B, Vegso JJ. Spinal injury at the third and fourth cervical vertebrae resulting from the axial loading mechanism: an analysis and classification. Clin Sports Med. 1987;6:159–183. [PubMed] [Google Scholar]
- 25.Wilberger JE, Maroon JC. Cervical spine injuries in athletes. Physician Sportsmed. 1990;18(3):57–70. doi: 10.1080/00913847.1990.11709993. [DOI] [PubMed] [Google Scholar]
- 26.Albright JP, Mcauley E, Martin RK, Crowley ET, Foster DT. Head and neck injuries in college football: an eight-year analysis. Am J Sports Med. 1985;13:147–152. doi: 10.1177/036354658501300301. [DOI] [PubMed] [Google Scholar]
- 27.Anderson C. Neck injuries: backboard, bench or return to play. Physician Sportsmed. 1993;21(8):23–34. doi: 10.1080/00913847.1993.11947585. [DOI] [PubMed] [Google Scholar]
- 28.Hodgson VR, Thomas LM. Play head-up football. Natl Fed News. 1985;2:24–27. [Google Scholar]
- 29.Saal JA, Sontag MJ. Head injuries in contact sports: sideline decision making. Phys Med Rehabil. 1987;1:649–658. [Google Scholar]
- 30.Torg JS. Epidemiology, pathomechanics, and prevention of athletic injuries to the cervical spine. Med Sci Sports Exerc. 1985;17:295–303. [PubMed] [Google Scholar]
- 31.Torg JS. Epidemiology, pathomechanics, and prevention of football-induced cervical spinal cord trauma. Exerc Sport Sci Rev. 1992;20:321–338. [PubMed] [Google Scholar]
- 32.Torg JS. Epidemiology, biomechanical and cinematographic analysis of football induced cervical spine trauma. Athl Train J Natl Athl Train Assoc. 1990;25:147–159. doi: 10.1177/036354659001800109. [DOI] [PubMed] [Google Scholar]
- 33.Torg JS, Sennett B, Vegso JJ, Pavlov H. Axial loading injuries to the middle cervical spine segment: an analysis and classification of twenty- five cases. Am J Sports Med. 1991;19:6–20. doi: 10.1177/036354659101900103. [DOI] [PubMed] [Google Scholar]
- 34.Diehl J. The National Federation: how rules are written. Paper presented at: National Athletic Trainers' Association 53rd Annual Meeting and Clinical Symposia; June 14–18, 2002; Dallas, TX. [Google Scholar]
- 35.Schneider RC. Head and Neck Injuries in Football: Mechanisms, Treatment, and Prevention. Baltimore, MD: Williams & Wilkins; 1973. [Google Scholar]
- 36.Dolan KD, Feldick HG, Albright JP, Moses JM. Neck injuries in football players. Am Fam Physician. 1975;12:86–91. [PubMed] [Google Scholar]
- 37.Funk FJ, Wells RE. Injuries of the cervical spine in football. Clin Orthop. 1975;109:50–58. doi: 10.1097/00003086-197506000-00007. [DOI] [PubMed] [Google Scholar]
- 38.Silver JR. Injuries of the spine sustained in rugby. Br Med J (Clin Res Ed) 1984;288:37–43. doi: 10.1136/bmj.288.6410.37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Melvin WJ, Dunlop HW, Hetherington RF, Kerr JW. The role of the faceguard in the production of flexion injuries to the cervical spine in football. Can Med Assoc J. 1965;93:1110–1117. [PMC free article] [PubMed] [Google Scholar]
- 40.Ciccone R, Richman RM. The mechanism of injury and the distribution of three thousand fractures and dislocations caused by parachute jumping. J Bone Joint Surg Am. 1948;30:77–97. [PubMed] [Google Scholar]
- 41.Ellis WG, Green D, Holzaepfel NR, Sahs AL. The trampoline and serious neurologic injuries: a report of five cases. JAMA. 1960;174:1673–1676. doi: 10.1001/jama.1960.03030130001001. [DOI] [PubMed] [Google Scholar]
- 42.Hage P. Trampolines: an “attractive nuisance.”. Physician Sportsmed. 1982;10(12):118–122. doi: 10.1080/00913847.1982.11947399. [DOI] [PubMed] [Google Scholar]
- 43.Kravitz H. Problems with the trampoline, I: too many cases of permanent paralysis. Pediatr Ann. 1978;7:728–729. [PubMed] [Google Scholar]
- 44.Tator CH, Edmonds VE. National survey of spinal injuries in hockey players. Can Med Assoc J. 1984;130:875–880. [PMC free article] [PubMed] [Google Scholar]
- 45.Tator CH, Ekong CE, Rowed DW, Schwartz ML, Edmonds VE, Cooper PW. Spinal injuries due to hockey. Can J Neurol Sci. 1984;11:34–41. doi: 10.1017/s0317167100045297. [DOI] [PubMed] [Google Scholar]
- 46.Torg JS, Das M. Trampoline-related quadriplegia: review of the literature and reflections on the American Academy of Pediatrics' position statement. Pediatrics. 1984;74:804–812. [PubMed] [Google Scholar]
- 47.Carvell JE, Fuller DJ, Duthie RB, Cockin J. Rugby football injuries to the cervical spine. Br Med J (Clin Res Ed) 1983;286:49–50. doi: 10.1136/bmj.286.6358.49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Gehweiler JA, Jr, Clark WM, Schaaf RE, Powers B, Miller MD. Cervical spine trauma: the common combined conditions. Radiology. 1979;130:77–86. doi: 10.1148/130.1.77. [DOI] [PubMed] [Google Scholar]
- 49.Leidholt JD. Spinal injuries in athletes: be prepared. Orthop Clin North Am. 1973;4:691–707. [PubMed] [Google Scholar]
- 50.Macnab I. Acceleration injuries of the cervical spine. J Bone Joint Surg Am. 1964;46:1797–1799. [PubMed] [Google Scholar]
- 51.McCoy GF, Piggot J, Macafee AL, Adair IV. Injuries of the cervical spine in schoolboy rugby football. J Bone Joint Surg Br. 1984;66:500–503. doi: 10.1302/0301-620X.66B4.6746681. [DOI] [PubMed] [Google Scholar]
- 52.Paley D, Gillespie R. Chronic repetitive unrecognized flexion injury of the cervical spine (high jumper's neck) Am J Sports Med. 1986;14:92–95. doi: 10.1177/036354658601400117. [DOI] [PubMed] [Google Scholar]
- 53.Piggot J, Gordon DS. Rugby injuries to the cervical cord. Br Med J. 1979;1:192–193. [PMC free article] [PubMed] [Google Scholar]
- 54.Williams JP, McKibbin B. Cervical spine injuries in rugby union football. Br Med J. 1978;2:1747. doi: 10.1136/bmj.2.6154.1747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Wu WQ, Lewis RC. Injuries of the cervical spine in high school wrestling. Surg Neurol. 1985;23:143–147. doi: 10.1016/0090-3019(85)90332-5. [DOI] [PubMed] [Google Scholar]
- 56.O'Carroll PF, Sheehan JM, Gregg TM. Cervical spine injuries in rugby football. Ir Med J. 1981;74:377–379. [PubMed] [Google Scholar]
- 57.Scher AT. “Crashing” the rugby scrum: an avoidable cause of cervical spinal injury: case reports. S Afr Med J. 1982;61:919–920. [PubMed] [Google Scholar]
- 58.Burke DC. Hyperextension injuries of the spine. J Bone Joint Surg Br. 1971;53:3–12. [PubMed] [Google Scholar]
- 59.Edilken-Monroe B, Wagner LK, Harris JH., Jr Hyperextension dislocation of the cervical spine. AJR Am J Roentgenol. 1986;146:803–808. doi: 10.2214/ajr.146.4.803. [DOI] [PubMed] [Google Scholar]
- 60.Forsyth HF. Extension injuries of the cervical spine. J Bone Joint Surg Am. 1964;46:1792–1797. [PubMed] [Google Scholar]
- 61.Marar BC. Hyperextension injuries of the cervical spine: the pathogenesis of damage to the spinal cord. J Bone Joint Surg Am. 1974;56:1655–1662. [PubMed] [Google Scholar]
- 62.Alexander E, Jr, Davis CH, Jr, Field CH. Hyperextension injuries of the cervical spine. AMA Arch Neurol Psychiatry. 1958;19:146–150. doi: 10.1001/archneurpsyc.1958.02340020026006. [DOI] [PubMed] [Google Scholar]
- 63.Torg JS, Quedenfeld TC, Burstein A, Spealman AD, Nichols CE., III National Football Head and Neck Injury Registry: report on cervical quadriplegia, 1971 to 1975. Am J Sports Med. 1979;7:127–32. doi: 10.1177/036354657900700209. [DOI] [PubMed] [Google Scholar]
- 64.Torg JS, Vegso JJ, O'Neill MJ, Sennett B. The epidemiologic, pathologic, biomechanical, and cinematographic analysis of football-induced cervical spine trauma. Am J Sports Med. 1990;18:50–7. doi: 10.1177/036354659001800109. [DOI] [PubMed] [Google Scholar]
- 65.Torg JS. Epidemiology, pathomechanics, and prevention of athletic injuries to the cervical spine. Med Sci Sports Exerc. 1985;17:295–303. [PubMed] [Google Scholar]
- 66.Yoganandan N, Sances A, Jr, Maiman DJ, Myklebust JB, Pech P, Larson SJ. Experimental spinal injuries with vertical impact. Spine. 1986;11:855–60. doi: 10.1097/00007632-198611000-00001. [DOI] [PubMed] [Google Scholar]
- 67.Mertz HJ, Hodgson VR, Thomas LM, Nyquist GW. An assessment of compressive neck loads under injury-producing conditions. Physician Sportsmed. 1978;6(11):95–106. doi: 10.1080/00913847.1978.11948406. [DOI] [PubMed] [Google Scholar]
- 68.Hodgson VR, Thomas LM. Proceedings of the Twenty-Fourth Staap Car Crash Conference. Warrendale, PA: Society of Automotive Engineers; 1980. Mechanism of cervical spine injury during impact to the protected head; pp. 17–42. [Google Scholar]
- 69.Sances A, Jr, Myklebust JB, Maiman DJ, Larson SJ, Cusick JF, Jodat RW. The biomechanics of spinal injuries. Crit Rev Biomed Eng. 1984;11:1–76. [PubMed] [Google Scholar]
- 70.Gosch HH, Gooding E, Schneider RC. An experimental study of cervical spine and cord injuries. J Trauma. 1972;12:570–576. doi: 10.1097/00005373-197207000-00004. [DOI] [PubMed] [Google Scholar]
- 71.Maiman DJ, Sances A, Jr, Myklebust JB, et al. Compression injuries of the cervical spine: a biomechanical analysis. Neurosurgery. 1983;13:254–260. doi: 10.1227/00006123-198309000-00007. [DOI] [PubMed] [Google Scholar]
- 72.Roaf R. A study of the mechanics of the spinal injuries. J Bone Joint Surg Br. 1960;42:810–823. [Google Scholar]
- 73.White AA, III, Punjabi MM. Clinical Biomechanics of the Spine. Philadelphia, PA: Lippincott; 1978. [Google Scholar]
- 74.Bauze RJ, Ardran GM. Experimental production of forward dislocation in the human cervical spine. J Bone Joint Surg Br. 1978;60:239–245. doi: 10.1302/0301-620X.60B2.659473. [DOI] [PubMed] [Google Scholar]
- 75.Nightingale RW, McElhaney JH, Richardson WJ, Best TM, Myers BS. Experimental impact injury to the cervical spine: relating motion of the head and the mechanism of injury. J Bone Joint Surg Am. 1996;78:412–421. doi: 10.2106/00004623-199603000-00013. [DOI] [PubMed] [Google Scholar]
- 76.Kazarian L. Injuries to the human spinal column: biomechanics and injury classification. Exerc Sport Sci Rev. 1981;9:297–352. [PubMed] [Google Scholar]
- 77.Kewalramani LS, Orth MS, Taylor RG. Injuries to the cervical spine from diving accidents. J Trauma. 1975;15:130–142. doi: 10.1097/00005373-197502000-00005. [DOI] [PubMed] [Google Scholar]
- 78.Albrand OW, Corkill G. Broken necks from diving accidents: a summer epidemic in young men. Am J Sports Med. 1976;4:107–110. doi: 10.1177/036354657600400303. [DOI] [PubMed] [Google Scholar]
- 79.Albrand OW, Walter J. Underwater deceleration curves in relation to injuries from diving. Surg Neurol. 1975;4:461–465. [PubMed] [Google Scholar]
- 80.Maroon JC, Steele PB, Berlin R. Football head and neck injuries: an update. Clin Neurosurg. 1980;27:414–429. [PubMed] [Google Scholar]
- 81.Mennen U. Survey of spinal injuries from diving: a study of patients in Pretoria and Cape Town. S Afr Med J. 1981;59:788–790. [PubMed] [Google Scholar]
- 82.Rogers WA. Fractures and dislocations of the cervical spine: an end- result study. J Bone Joint Surg Am. 1957;39:341–376. [PubMed] [Google Scholar]
- 83.Scher AT. Diving injuries to the cervical spinal cord. S Afr Med J. 1981;59:603–605. [PubMed] [Google Scholar]
- 84.Scher AT. Injuries to the cervical spine sustained while carrying loads on the head. Paraplegia. 1978;16:94–101. doi: 10.1038/sc.1978.15. [DOI] [PubMed] [Google Scholar]
- 85.Scher AT. “Tear-drop” fractures of the cervical spine: radiological features. S Afr Med J. 1982;61:355–356. [PubMed] [Google Scholar]
- 86.Scher AT. The high rugby tackle: an avoidable cause of cervical spinal injury? S Afr Med J. 1978;53:1015–1018. [PubMed] [Google Scholar]
- 87.Scher AT. Vertex impact and cervical dislocation in rugby players. S Afr Med J. 1981;59:227–228. [PubMed] [Google Scholar]
- 88.Bishop PJ. Impact postures and neck loading in head first collisions: a review. In: Hoerner EF, editor. Head and Neck Injuries in Sports ASTM STP 1229. Philadelphia, PA: American Society for Testing and Materials; 1994. pp. 127–141. [Google Scholar]
- 89.Burstein AH, Otis JC. The response of the cervical spine to axial loading: feasibility for intervention. In: Hoerner EF, editor. Head and Neck Injuries in Sports ASTM STP 1229. Philadelphia, PA: American Society for Testing and Materials; 1994. pp. 142–153. [Google Scholar]
- 90.Pintar FA, Yoganandan N, Sances A JF, Cusick JF. Experimental production of head-neck injuries under dynamic forces. In: Hoerner EF, editor. Head and Neck Injuries in Sports ASTM STP 1229. Philadelphia, PA: American Society for Testing and Materials; 1994. pp. 203–211. [Google Scholar]
- 91.Yoganandan N, Pintar FA, Sances A, Jr, Reinartz J, Larson SJ. Strength and kinematic response of dynamic cervical spine injuries. Spine. 1991;16(10 suppl):S511–S517. doi: 10.1097/00007632-199110001-00011. [DOI] [PubMed] [Google Scholar]
- 92.Yoganandan N, Sances A, Jr, Maiman DJ, Myklebust JB, Pech P, Larson SJ. Experiemental spinal injuries with vertical impact. Spine. 1986;11:855–859. doi: 10.1097/00007632-198611000-00001. [DOI] [PubMed] [Google Scholar]
- 93.Burstein AH, Otis JC, Torg JS. Mechanisms and pathomechanics of athletic injuries to the cervical spine. In: Torg JS, editor. Athletic Injuries to the Head, Neck, and Face. Philadelphia, PA: Lea & Febiger; 1982. pp. 139–154. [Google Scholar]
- 94.Torg JS, Truex RC, Jr, Marshall J, et al. Spinal injury at the level of the third and fourth cervical vertebrae from football. J Bone Joint Surg Am. 1977;59:1015–1019. [PubMed] [Google Scholar]
- 95.Allen BL, Jr, Ferguson RL, Lehmann TR, O'Brien RP. A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine. 1982;7:1–27. doi: 10.1097/00007632-198200710-00001. [DOI] [PubMed] [Google Scholar]
- 96.Jackson DW, Lohr FT. Cervical spine injuries. Clin Sports Med. 1986;5:373–386. [PubMed] [Google Scholar]
- 97.Watkins RG. Neck injuries in football players. Clin Sports Med. 1986;5:215–246. [PubMed] [Google Scholar]
- 98.Carter DR, Frankel VH. Biomechanics of hyperextension injuries to the cervical spine in football. Am J Sports Med. 1980;8:302–309. doi: 10.1177/036354658000800502. [DOI] [PubMed] [Google Scholar]
- 99.Virgin H. Cineradiographic study of football helmets and the cervical spine. Am J Sports Med. 1980;8:310–317. doi: 10.1177/036354658000800503. [DOI] [PubMed] [Google Scholar]
- 100.Cantu RC. Head and spine injuries in the young athlete. Clin Sports Med. 1988;7:459–472. [PubMed] [Google Scholar]
- 101.Drake GA. Research provides more suggestions to reduce serious football injuries. Natl Fed News. 1994 Nov-Dec;:18–21. [Google Scholar]
- 102.Drake GA. Catastrophic football injuries and tackling techniques. In: Hoerner EF, editor. Safety in American Football, ASTM STP 1305. Philadelphia, PA: American Society for Testing and Materials; 1996. pp. 42–49. [Google Scholar]
- 103.Heck JF. The incidence of spearing during a high school's 1975 and 1990 football seasons. J Athl Train. 1996;31:31–37. [PMC free article] [PubMed] [Google Scholar]
- 104.Heck JF. Preventing catastrophic head and neck injuries in football. From Gym Jury. 1998;10(1):7. [Google Scholar]
- 105.Heck JF. Re-examining spearing: the incidence of cervical spine injury hides the risks. Am Football Coach. 1999;5(8):52–54. [Google Scholar]
- 106.Football-related spinal cord injuries among high school players: Louisiana, 1989. MMWR Morb Mortal Wkly Rep. 1990;39:586–587. [PubMed] [Google Scholar]
- 107.Buckley WE. Concussions in college football: a multivariate analysis. Am J Sports Med. 1988;16:51–56. doi: 10.1177/036354658801600109. [DOI] [PubMed] [Google Scholar]
- 108.Cantu RC. Guidelines for return to contact sports after a cerebral concussion. Physician Sportsmed. 1986;14(10):75–83. doi: 10.1080/00913847.1986.11709197. [DOI] [PubMed] [Google Scholar]
- 109.Heck JF. The state of spearing in football: incidence of cervical spine injuries doesn't indicate the risks. Sports Med Update. 1998;13(2):4–7. [Google Scholar]
- 110.National Federation of State High School Associations. Official Football Rules. Indianapolis, IN: National Federation of State High School Associations; 2002. [Google Scholar]
- 111.National Collegiate Athletic Association. 2001 Football Rules and Interpretations. Indianapolis, IN: National Collegiate Athletic Association; 2001. [Google Scholar]
- 112.National Federation of State High School Associations. Official Football Rules. Elgin, IL: National Federation of State High School Associations; 1976. [Google Scholar]
- 113.National Collegiate Athletic Association. Football Rules Changes and/ or Modifications. Kansas City, MO: National Collegiate Athletic Association; 1976. January 23. [Google Scholar]
- 114.National Collegiate Athletic Association. 2001 Consolidated NCAA Foul Report. Indianapolis, IN: National Collegiate Athletic Association; 2002. [Google Scholar]
- 115.Peterson TR. Roundtable: head and neck injuries in football. Paper presented at: American Society for Testing and Materials' International Symposium on Head and Neck Injuries in Sports; May 1993; Atlanta, GA. [Google Scholar]
- 116.Heck JF. A survey of New Jersey high school football officials regarding spearing rules. J Athl Train. 1995;30:63–68. [PMC free article] [PubMed] [Google Scholar]
- 117.Lutz R. Good judgment critical in making call. Available at: http://www.mcoa.org/articles/fb_003.html. Accessed July 9, 2002.
- 118.National Federation of State High School Associations. Official Football Rules. Indianapolis, IN: National Federation of State High School Associations; 1988. [Google Scholar]
- 119.Lawrence DS, Stewart GW, Christy DM, Gibbs LI, Ouellette M. High school football-related cervical spinal cord injuries in Louisiana: the athlete's perspective. Available at: http://www.injuryprevention.org/states/la/football/football.htm. Accessed July 15, 2002. [PubMed]
- 120.National Federation of State High School Associations. Official Football Rules. Indianapolis, IN: National Federation of State High School Associations; 1994. [Google Scholar]
- 121.Bishop PJ. Factors related to quadriplegia in football and the implications for intervention strategies. Am J Sports Med. 1996;24:235–239. doi: 10.1177/036354659602400222. [DOI] [PubMed] [Google Scholar]
- 122.Heck JF. The football official's role in the prevention of catastrophic neck injuries. Presented at: Southern New Jersey Football Officiating Association Meeting; September 1994; Audubon, NJ. [Google Scholar]
- 123.Kleiner DM, Almquist JL, Bailes J, et al. Prehospital Care of the Spine-Injured Athlete. Dallas, TX: Inter-Association Task Force for Appropriate Care of the Spine-Injured Athlete; 2001. [DOI] [PubMed] [Google Scholar]
- 124.Albright JP, Moses JM, Feldick HD, Dolan KD, Burmeister LF. Nonfatal cervical spine injuries in interscholastic football. JAMA. 1976;236:1243–1245. [PubMed] [Google Scholar]
- 125.Graves JE, Pollock ML, Leggett SH, et al. Effect of reduced training frequency on muscular strength. Int J Sports Med. 1988;9:316–319. doi: 10.1055/s-2007-1025031. [DOI] [PubMed] [Google Scholar]
- 126.Patterson D. Legal aspects of athletic injuries to the head and cervical spine. In: Torg JS, editor. Athletic Injuries to the Head, Neck, and Face. 2nd ed. St. Louis, MO: Mosey Year Book; 1991. pp. 198–209. [Google Scholar]
- 127.Patterson D. Legal aspects of athletic injuries to the head and cervical spine. Clin Sports Med. 1987;6:197–210. [PubMed] [Google Scholar]
- 128.Boulet v Brunswick Corporation. 126 Mich App 240 (1982)
- 129.Dibortolo v Metropolitan School District. 440 NE2d 506 Ind Ct App (1982)
- 130.Gerrity v Beatty. 71 Ill 2d 47 (1978)
- 131.Green v Orleans Parish School Board. 365 So2d 834, 836 La Ct App (1978)
- 132.Jackson v Board of Education 109. Ill App 3d 716, 441 NE2d 120 (1982)
- 133.Landers v School District #203. 66 Ill App 3d 78, 383 NE2d 645 (1978)
- 134.Low v Texas Tech University. 540 SW2d 297 Tex Supreme Ct (1976)
- 135.Peterson v Multnomah County School District. 669 P2d 387, 393 (1983)
- 136.Stehn v Bernarr Macfadden Foundations, Inc. 434 F2d811 6th Cir (1970)
- 137.Vendrell v School District No 26C. 233 Ore 1 (1962)
- 138.Wissel v Ohio High School Athletic Association. 78 Ohio App 3d 529 (1992)
- 139.Black J. Legal implications for the secondary school athlete. Paper presented at: National Athletic Trainers' Association 53rd Annual Meeting and Clinical Symposia; June 14–18; 2002: Dallas, TX. [Google Scholar]
- 140.Heck JF, Weis MP, Gartland JM, Weis CR. Minimizing liability risks of head and neck injuries in football. J Athl Train. 1994;29:128–139. [PMC free article] [PubMed] [Google Scholar]