

Abstract
Background and Aims:
The hemodialysis (HD) patients are experiencing high biopsychosocial stress on all levels. Therefore, this study was designed to survey on physiologic and psychosocial stressors among HD patients in two educational hospitals of Northern Iran.
Materials and Methods:
This cross-sectional study included 80 HD patients who were referred to Khomeini and Fatemeh Zahra hospitals in Mazandaran (Northern Iran) during the year 2011. Data were collected using a demographic information record sheet and Baldree Hemodialysis Stress Scale.
Finding:
The following physiologic stressors were noted: Fatigue (51.25%), limited time and places for enjoyment (46.25%), and physical activation limitation (32.5%). Similarly the following psychosocial stressors were observed: Fistula (58.75%), limitation of drinking water (47.5%), low quality of life (47.5%), travelling difficulties to the dialysis center (45%), treatment cost (41.5%), and low life expectancy. The stress level was high in women who were married, younger, less dialysis vintage, and belonged to a low education level.
Conclusion:
This study reports that HD patients have with significant physical and psychosocial problems and they need education, family, and social supports.
Keywords: Chronic renal failure, Hemodialysis patients, Psychosocial stress
INTRODUCTION
Chronic renal failure is a progressive deterioration of renal function that causes uremia, and has comorbidity with disease of water and body electrolyte metabolism.[1] Once glomerular filtration rate (GFR) falls below 15 mL/min/1.73 m2 and patients progress into the stage of renal failure, renal replacement therapies such as dialysis and transplantation are required.[2] A 15% increase of these patients has been seen annually in Iran.[3] The most common treatment methods included renal transplantation, hemodialysis (HD), and peritoneal dialysis.[4] Although these methods help to increase the lifetime of patients, they could significantly affect the physical, social, and mental functions.[5] They suffer from a number of dialysis-specific stressors in addition to many medical problems and direct physical effects of rental disorder that leads to change their lifestyle during the time.[6] HD is a source of economic burden and various complications. Compared to the general population, individuals with HD have elevated symptoms of anxiety, depression, and low life expectancy. The patients in the age group 40-44 and 60-64 have 7-10 and 4-5 years life expectancy, respectively.[7],[8] In the last few decades, researchers have highlighted the importance of psychological factors in chronic renal failure.[9] Although mental health directly depends on physical health,[10],[11] inappropriate responses to stressors could lead to poor quality of life quality in HD patients.[12]
Only limited studies are available in this area in Iran and there is some inconsistency even in conducted studies. In these patients, identifying and introducing stressor factors is the first step of intervention and planning. Therefore, we conducted a study on the physical and psychosocial stressors that can affect the social health and planning to support HD patients.
MATERIALS AND METHODS
This study was a cross-sectional study and has been conducted during the period January 2011 to November 2011. The study subjects included all HD patients present in two main hospitals of Mazandaran province: Emam Khomeini and Fatemeh Zahra. Of 168 patients, 80 met the inclusion criteria. The inclusion criteria were: Age range 18-65; history of HD at least for 2 months in a dialysis center; and no disability or other chronic disease (except diabetes and hypertension). The exclusion criteria were use of antistress and anxiety medicines, disaster experienced during the last 6 months, and peritoneal dialysis or a kidney transplant procedure.
We used a demographic information record sheet and Hemodialysis Stress Scale (HSS: Baldriee, Murphy, and Powers, 1982) to collect the data. The demographic questionnaire comprised information about age, gender, marital status, income, education level, dialysis course during the day and week, dialysis vintage, shelter status, other diseases, and use of medicines except rental disease.
HSS is a self-report measurement that composed of 29 specific items (6 physiological and 23 psychosocial stressors). Responses indicated item intensity via a 4-point Likert-scale: No stress (0), less stress (1), low stress (2), the average stress (3), and high stress. The patients were asked to mark every item in the questionnaire on the basis of severity. The total score of HSS is between 0 and 116 and depends on patients’ response and is categorized into three levels: Low stress (0-40), the average stress (41-80), and high stress (81-116).[13] The validity of the questionnaire was assessed in a previous study in another country.[14] In Iran, recently one study validated the questionnaire of HD patients, who meet inclusion criteria and participated. To validate the questionnaire, they repeated the same procedure after 14 days with the same subjects. Test-retest (ICC analysis) reliability at 2-week intervals was showed a correlation of 81.[15]
The descriptive statistic data included frequency, percentage, etc., and analyzed by using SPSS software.
Findings
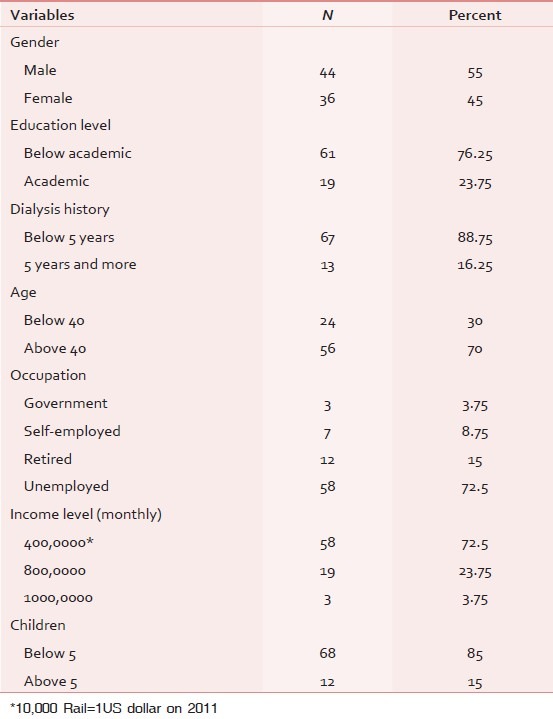
Among the HD patients, 44 (55%) were male and 36 (45%) female. The average age was 47.98 ± 12.53. The minimum and maximum age was 18 and 65, respectively. The majority of patients, i.e., 72.5%, were under treatment with the support of family members because they were housekeepers (39.75%) or unemployed (32.75%). Of them, 71 (88.8%) were married, 8 (10%) were single, and one (1.2%) was divorced. Sixty-one patients (76.255%) were below undergraduate, Fifty-eight (72.5%) had income less than 400,0000 Rail (400 US dollar) per month. Further, 67 (83.75%) were below 5-year dialysis and 68 (85%) had less than 5 children [Table 1].
Table 1.
Distribution of demographic characters of patients
The physiological factors physical stress, fatigue (51.25%), limited time and places for enjoyment and entertainment (46.25%), and limited physical function (32.5%) were the highest stressor factors [Figure 1]. The psychosocial stressors were worry about fistula (58.75%), limitation of water drinking (47.5%), low quality of life (47.5%), travelling difficulties to the dialysis center (45%), treatment cost (41.5%), and low life expectancy [Figure 2].
Figure 1.
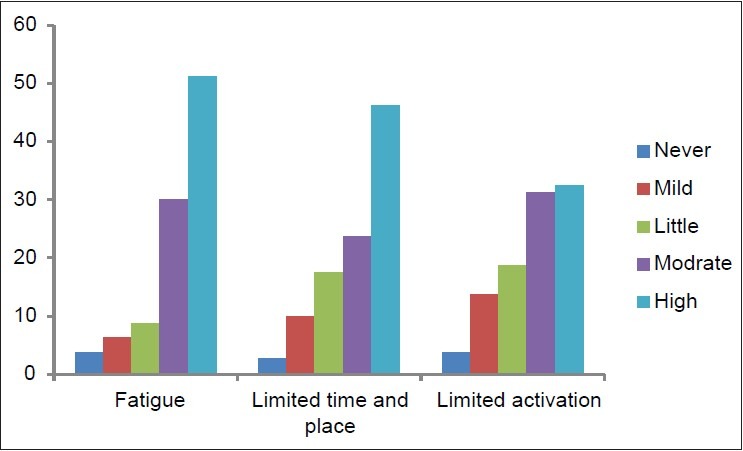
Distribution of physiologic stressor factors in hemodialysis patient
Figure 2.
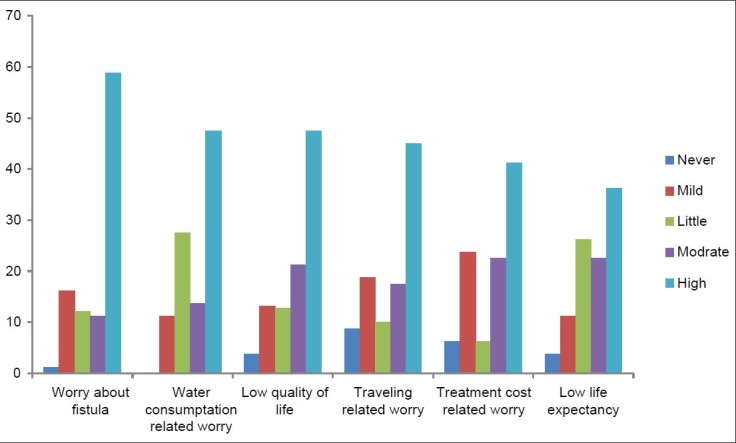
Distribution of psychosocial stressor factors in hemodialysis patients
DISCUSSION
The results showed that fatigue, limited time and places for enjoyment, and limited activation played the crucial roles in physical stressors. Fistula-related worry, water drinking related worry, low quality of life, travelling-related worry, treatment cost-related worry, and low life expectancy were the highest psychosocial factors among the patients.
In the Bahrami Nejad study conducted in Qazvin of Iran, the main reported stressors were limited physical activation, limited time and place for enjoyment, and decreased social activations.[11] In another study carried out in China by Mug et al., limitation in eating and drinking, inching, fatigue, and treatment cost were the most effective stressors on the HD patients.[16] These reported studies were in good agreement the present study. In another study carried out in Taiwan, Jenifer et al., reported dependency to medical treatments, blood vessel problems, and infertility as the major stressors of HD patients.[16] According to Mug et al., physical stressors were more effective than psychosocial stressors.[17] However, Baldree et al. manifested no difference between two kinds of stressors (physical and psychosocial). In contrast, Dewince et al. reported physical factors such as diet, occupation, and treatment costs as high stressors.[17]
Logan et al. demonstrated factors such as fatigue and drinking limitation are the most prevalent stress sources among these patients.[18] Mahmoudi et al. reported that low income families are more vulnerable and they followed a more emotional coping style. The emotional coping style would lead to isolation, avoidance, and suppression of feelings.[19] In the Bahrami Nejad study, the role of low income was also highlighted and emphasized that the patients commonly does not have regular income event the government covered most treatment costs.[11],[19] Sajadi (2010) reported that the people who had low income or were unemployed experienced more fatigue.[20]
Shafiipoor et al. (2009) noted that unemployed persons experienced low level of quality of life.[20],[21] Mollaoglu (2009) and Salivan (2007) reported that the high level of activation is related to fatigue. The people who are active and employed experience less fatigue.[21],[22] These studies are in good agreement with our study results. In another study, Cinar et al. (2009) finding showed the limited recreation, fatigue, and disappointment toward the future are the effective stressors in HD patient's life.[23] Lok (1996) in his research released that the most common reasons on stress among HD patients are low life quality, disappointment about the future, and fatigue.[24]
CONCLUSION
The results demonstrated the most common physical and psychosocial problems of HD patients, which included fatigue, treatment costs, travelling, limited activation, limited drinking, and limited time and places for entertainment. Some differences and contrasts have seen in reported research studies and evidence that most were related to differences of cultures and geography and social values. Generally, the patient's problems were not extremely different, which depended on social and family supports.
There were some limitations in our study. This study was a cross-sectional study with a limited number of patients and conducted only in two centers, which are located in Mazandaran, with a heterogeneous sample. Therefore, factors such as local belief and culture regarding Mazandaran surrounded by village areas and lack of awareness about psychological methods are the significant factors. They affect physical behaviors, education levels, and income, which are mostly high in this area of Iran compared to other parts of Iran. Therefore, these factors limited the generalization of the results of this study to other regions. Further studies on dialysis centers with a greater sample size and indifference geographical areas are needed.
ACKNOWLEDGMENT
We are thankful to Fateme Zahra and Khomeini hospitals staff and patients for their corporation.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Heidarzadeh M, Atashpeiker S, Jalilazar T. Relationship between quality of life and self care ability in patients receiving hemodilysis. Iran J Nurs Midwifery Res. 2010;15:66–71. [PMC free article] [PubMed] [Google Scholar]
- 2.Baykan H, Yargic I. Depression, Anxiety Disorders, Quality of Life and Stress Coping Strategies in Hemodialysis and Continuous Ambulatory Peritoneal Dialysis Patients. J Clin Psychopharmacol. 2012;22:167–76. [Google Scholar]
- 3.Ghaffari A. Renal transplantation two-day seminar. MED and LAB Enginering Magazine. 2007;8:37. [Google Scholar]
- 4.Einollahi B, Taheri S. Renal transplantation practice in Iran and Middle East: Report from Iran and review of the literature. Ann Transplant. 2008;13:5–14. [PubMed] [Google Scholar]
- 5.Zamanzade V, Heydarzade M, Ashvandi K, Lak D. Relationship between quality of life and social support in hemodialysis patient. Med J Tabriz Univ Sci. 2007;7:49–54. [Persian] [Google Scholar]
- 6.Ibrahim K, Taboonpong S, Nilmanat K. Coping and quality of life among Indonesians undergoing hemodialysis. Thai J Nurs Res. 2009;2:109–17. [Google Scholar]
- 7.Borzou SR, Ghlyaf M, Amini R, Zandieh M, Turkman B. Effect of increasing blood flow rate on dialysis adequacy in hemodialysis patients. Jornal of Shahrkord University of Medical Sciences. 2005;8:60–6. [Google Scholar]
- 8.Finkelsein F, Finkelsein S. Depression in chronic dialysis patients: Assessment and treatment. Nephrol Dial Transplant. 2000;15:1911–3. doi: 10.1093/ndt/15.12.1911. [DOI] [PubMed] [Google Scholar]
- 9.Kimmel P. Psychosocial factors in dialysis patients. Nephrology Forum. Kidney Int. 2001;59:1599–613. doi: 10.1046/j.1523-1755.2001.0590041599.x. [DOI] [PubMed] [Google Scholar]
- 10.Mirzaei M, Azymyan M. Study of neurological complications of Hemodialysis in dialysis patients. Iranian J Neurol. 2009;8:458–64. [Google Scholar]
- 11.Bahrami Nejad N. Psychosocial stressors in Hemodialized patients of Qazvin. JQUMS. 2000;4:90–5. [Google Scholar]
- 12.Shafiipoor V, Jaffrei H, Shafiipoor L. The relationship between stress and quality of life in Hemodialysis patients in Sari hospitals. Sabzevar Univ Med Sci Health Serv. 2007;16:160–55. [Google Scholar]
- 13.Kiani GA, Kermanshahi S, Ahmadi F. Study of the effect of Benson's relaxation technique on hemodynamic parameters and stress of discharge in acute myocardial infarction patients in Tehran, 2002. J Shaheed Sadoughi Univ Med Sci and Health Serv Yazd. 2003;11:50–6. [Google Scholar]
- 14.Rexm S, Haaland K. Kaplan and sadock's comprehensive text book of psychiatry-clinical neropsychology and intellectual assesment of adults. 19th ed. Philadelphia PA: Lippincott Williams & Wilkins; 2010. pp. 953–4. [Google Scholar]
- 15.Elali ES, Mahdavi A, Jannati Y, Yazdani Cherati J, Setareh J. Effects of Benson relaxation responses on stress among hemodialysis patients. Mazand Univ Med Sci. 2012;22:61–8. [Persian] [Google Scholar]
- 16.Yeh SC, Chou HC. Coping Strategies and Stressors In Patients With Hemodialysis. Psychosom Med. 2007;69:182–90. doi: 10.1097/PSY.0b013e318031cdcc. [DOI] [PubMed] [Google Scholar]
- 17.Mok E, Tam B. Stressors and coping methods among chronic haemodialysis patients in Hong Kong. J Clin Nurs. 2001;10:503–11. doi: 10.1046/j.1365-2702.2001.00500.x. [DOI] [PubMed] [Google Scholar]
- 18.Logan S, Pelletier-Hibbert M, Hodgins M. Stressors and coping of in-hospital haemodialysis patients aged 65 years and over. J Adv Nurs. 2006;56:382–91. doi: 10.1111/j.1365-2648.2006.04015.x. [DOI] [PubMed] [Google Scholar]
- 19.Mahmoudi GH, Sharyati A, Behnampoor N. Relationship beetween Quality of life and using of coping sterategies with undergoing Hemodialysis patients. J Golestan Univ. 2003;5:43–52. [Google Scholar]
- 20.Sajadi A, Farmahini Farahani B, Esmaeilpoor Zanjani S, Durmanesh B, Zare M. Determine of factors relation to fatique in patients soffering from ESRD undergoing Hemodialysis treatment. Iranian Journal of Critical Care Nursing. 2010;3:38–3. [Google Scholar]
- 21.Mollaoglu M. Fatigue in people undergoing hemodialysis. Dial Transplant. 2009;38:216–20. [Google Scholar]
- 22.Salivan D, McCarty G. An exploration of the relationship between fatigue and physical functioning in patients with end stage renal disease receiving hemodialysis. J Clin Nurs. 2007;16:276–84. doi: 10.1111/j.1365-2702.2007.01965.x. [DOI] [PubMed] [Google Scholar]
- 23.Cinar S, Barlas G, Slppar S. stressors and coping strategies in Hemodialysis patients. Pak J Med Sci. 2009;25:447–52. [Google Scholar]
- 24.Lok P. Stressors, coping mechanisms and Quality of life among dialysis patients in Australia. J Adv Nurs. 1996;23:873–81. doi: 10.1046/j.1365-2648.1996.00893.x. [DOI] [PubMed] [Google Scholar]