

Abstract
Denture-induced hyperplasia is a reactive lesion arising from excessive and chronic mechanical pressure on the vestibular oral mucosa. It has a female predilection and it is mostly seen in the maxilla. The size of the lesion may be as small as a few millimeters to massive lesion involving the entire vestibule. It is usually asymptomatic but sometimes severe inflammation and ulceration can occur. Elimination of the inflammation and excision of the lesion is the treatment of choice. Denture induced hyperplasia in right maxillary buccal vestibule in a middle age old female patient was presented. Surgical excision was done and new denture was fabricated.
Keywords: Denture hyperplasia, Denture, Epulis fissuratum
Introduction
Denture-induced hyperplasia otherwise called epulis fissuratum is a hyperplastic condition of the oral mucosa caused by low-grade chronic trauma from ill-fitting dentures.[1] It is a reactive lesion of the oral mucosa to excessive mechanical pressure on the mucosa.[2] Resorption of residual alveolar bone leads to overextension of denture border which if not attended to causes chronic irritation of the oral mucosa in the region of the sulcus. When the offending denture is removed, a characteristic fissure bounded by hyperplastic soft tissue on both sides is seen. The chronic nature of the process means that discomfort is often not a prominent feature and therefore the patient may continue to wear the offending denture until hyperplastic lesions of considerable size develops before the patient becomes aware of the lesion and need for treatment.[3] However, the lesion may be associated with discomfort and pain when ulceration occurs. It is more commonly seen in females.[4,5] It occurs in 5-10% of the jaws with complete dentures and more in maxilla.[2] Denture-induced hyperplasia can be treated conservatively or surgically depending on the size of the lesion.[1]
Case Report
A 51-year-old female patient visited the department of Oral Medicine and Radiology, Yenepoya Dental College, Mangalore with a complaint of pain while chewing since 1 year. She also gave a history of small soft tissue mass in relation to the upper arch which has developed to the present size over a 12-month period. The patient has been wearing upper removable complete denture for 6 years. Pain was moderate and intermittent. The patient used to wear the denture during night time also. Her denture had become loose over a period of time and teeth were attrited. Her medical and family history was noncontributory. She had no deleterious habit like tobacco chewing. Extra oral examination showed no abnormality. She was moderately built and nourished. Intraoral examination revealed multiple hyperplastic tissue folds in the right maxillary buccal vestibule extending from the right lateral incisor region to the third molar area with maxillary denture flange fitting in between the tissue folds [Figure 1]. There was an irregular ulcer measuring 2 × 1 cm in diameter on the surface of the lesion in relation to first molar covered with slough. The lesion was firm, nontender except in the area where ulcer was present. Palatal mucosa was normal and there was generalized recession of gingiva in the lower arch and bilaterally molars were missing. The denture hygiene was poor. On the basis of history and clinical examination a provisional diagnosis of denture-induced hyperplasia was made. The patient was instructed not to wear the denture. Hexigel ointment was prescribed to be applied on the ulcer. Oral prophylaxis was done in the lower arch. The patient was educated and motivated to maintain the oral hygiene. Seeing the extent of the lesion, a surgical resection was planned along the full length of the maxilla after reviewing the patient for any medical condition. The tissue was infiltrated with local anesthesia containing adrenaline 2% and posterior superior alveolar, infraorbital and greater palatine nerve blocks were given. Using a no. 15 surgical blade an outline for resection in a wedge shape was made along the length of the lesion. The resection was then carried out from the midline till the posterior tuberosity region. Hemostasis was achieved. The field was cleaned with betadine and saline solution. A primary closure was achieved using 3-0 vicryl suture material [Figure 2]. Postoperatively, antibiotics and analgesics were prescribed. The patient was instructed not to wear the denture and rinse the mouth with chlorhexidine mouthwash. The excised specimen [Figure 3] was sent for histolopathological examination. It revealed hyperplastic epithelium in most of the areas, and the underlying connective tissue was fibrous, with moderate inflammatory infiltrate consisting of predominantly lymphocytes. The patient was recalled for follow-up after a week and the healing was satisfactory. The new denture was fabricated after 1 month [Figure 4]. The patient is on regular follow-up for 6 months and there was no recurrence of the lesion till date [Figure 5].
Figure 1.

Multiple hyperplastic tissue folds in the right maxillary buccal vestibule
Figure 2.
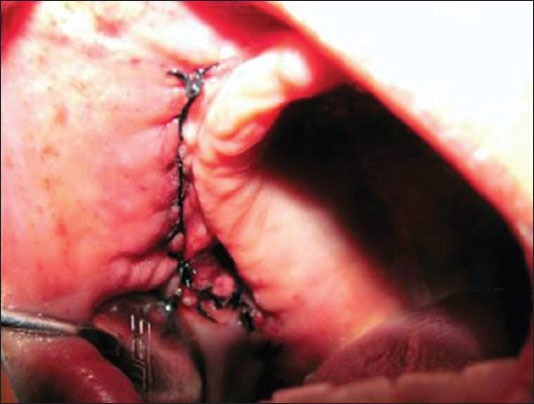
A primary closure
Figure 3.

Excised specimen
Figure 4.
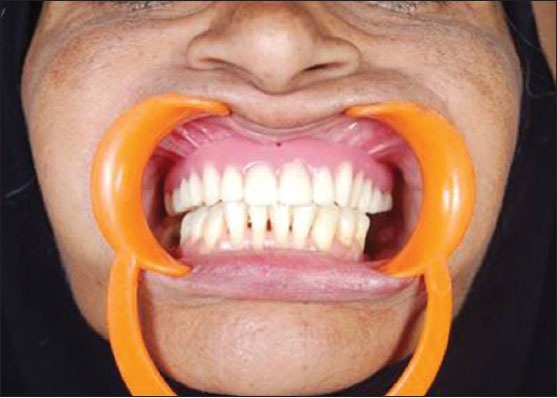
The new denture was fabricated after one month
Figure 5.

Regular follow-up and there were no recurrence
Discussion
Injury to oral tissue by ill fitting denture is one of the causes of denture-induced hyperplasia. It has a female predilection. Firoozmand et al.[5] reported that 78% of females had denture-induced hyperplasia which is mostly seen in maxilla. The size of the lesion may be as small as few millimeters to massive lesion involving the entire vestibule. It is usually asymptomatic but sometimes severe inflammation and ulceration can occur. The reported case also had lesion in maxillar of a female patient. Denture-induced hyperplasia may be the result of ill-fitting dentures, poor oral hygine, wearing dentures all day and all night, smoking, age-related changes, and systemic conditions. Irritation and trauma to the palatal salivary glands and inappropriate relief chambers in dentures are also considered as etiological factors.[2] In our reported case ill-fitting denture and poor oral hygine were the causes.
Denture-induced hyperplasia may be treated conservatively or surgically. In the early stages of fibrous hyperplasia, when fibrosis is minimal, nonsurgical treatment with a denture in combination with a soft liner is frequently sufficient for reduction or elimination of this tissue. When the lesion is completely healed the acrylic flange may be relined and redesigned to avoid any further trauma to the mucosa. When the condition has been present for some time and significant fibrosis exists within the hyper plastic tissue, this will not respond to nonsurgical treatment. Excision of hyperplastic tissue is the treatment of choice in such cases. Since the lesion was large it was treated with surgical excision followed by fabrication of new denture and the patient was educated on the need to maintain the oral hygiene.[1]
Three techniques have been used successfully for treatment of inflammatory fibrous hyperplasia. When the area to be excised is minimally enlarged, electrosurgical or laser techniques provide good results for tissue excision.[1] If the tissue is extensive, simple excision and reapproximation of the remaining tissue is preferred. Electrosurgical techniques in such cases may result in excessive vestibular scarring. The redundant areas of tissue are grasped with tissue pickups, a sharp incision is made at the base of the excessive fibrous tissue down to the periosteum, and the hyperplastic tissue is removed. The adjacent tissue is gently undermined and reapproximated using interrupted or continuous sutures.[6]
When areas of gross tissue redundancy are found, simple excision frequently results in total elimination of the vestibule. In such cases, excision of the epulae, with peripheral mucosal repositioning and secondary epithelialization, is preferable.[6] In this procedure the hyperplastic soft tissue is excised superficial to the periosteum from the alveolar ridge area. A clean supraperiosteal bed is created over the alveolar ridge area, and the unaffected margin of the tissue excision is sutured to the most superior aspect of the vestibular periosteum with an interrupted suture technique. A surgical splint or denture lined with soft tissue conditioner is inserted and worn continuously for the first 5-7 days with removal only for oral saline rinses. Secondary epithelialization usually takes place and denture impressions can be made within 4 weeks.[1] Laser excision of large epulis allows complete removal without excessive scarring or bleeding.[7] A denture relined with soft liner can provide for additional postoperative comfort.
The hyperplastic tissue usually represents only the result of an inflammatory process; however, other pathologic conditions may exist. It is therefore imperative that representative tissue samples should always be submitted for pathologic examination after removal.[8]
Conclusion
A case of successfully managed extensive denture-induced hyperplasia is presented. The need for regular maintenance visits and good denture hygiene habits is also highlighted. Patients with epulis fissuratum should be educated about the benign nature of the condition, treatment options, and importance of not to wear the dentures at night time.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Kafas P, Upile T, Stavrianos C, Angouridakis N, Jerjes W. Mucogingival overgrowth in a geriatric patient. Dermatol Online J. 2010;16:7. [PubMed] [Google Scholar]
- 2.Canger EM, Celenk P, Kayipmaz S. Denture-related hyperplasia: A clinical study of a Turkish population group. Braz Dent J. 2009;20:243–8. doi: 10.1590/s0103-64402009000300013. [DOI] [PubMed] [Google Scholar]
- 3.Bhasker RM, Davenport JC, Thomson JM. 5th ed. UK: Willy-Blackwell; 2001. Prosthetic treatment of the edentulous patients. [Google Scholar]
- 4.Espinoza I, Rojas R, Aranda W, Gamonal J. Prevalance of oral mucosal lesions in elderly people in Santiago Chile. J Oral Pathol Med. 2003;32:571–5. doi: 10.1034/j.1600-0714.2003.00031.x. [DOI] [PubMed] [Google Scholar]
- 5.Firoosmand LM, Almeide JD, Cabral LA. Study of denture-induced fibrous hyperplasia cases diagnosed from 1979-2001. Quintessence Int. 2005;36:825–9. [PubMed] [Google Scholar]
- 6.Omal PM, Mathew SA. Denture-induced extensive fibrous inflammatory hyperplasia (Epulis fissuratum) Kerala Dent J. 2010;3:154–5. [Google Scholar]
- 7.Naveen Kumar J, Bhaskaran M. denture induced fibrous hyperplasia. Treatment with carbon dioxide laser and a two year follow-up. Indian J Dent Res. 2007;18:135–7. doi: 10.4103/0970-9290.33791. [DOI] [PubMed] [Google Scholar]
- 8.Bhusal D, Joshi S. Comprehensive complete denture rehabilitation, a way to achieve recovery of abused tissue: A case report. J Nepal Dent Assoc. 2010;11:59–6. [Google Scholar]