

Abstract
The study aimed to evaluate the effect of cupping therapy at a clinical setting for knee osteoarthritis. A randomized, controlled clinical trial was conducted. Cupping was performed on 0-6th day; 9-11th day and 14th day, i.e., 11 sittings follow-up to determine longer term carryover of treatment effects utilizing both objective and subjective assessment. The assessment was performed before and after treatment spreading over a period of 15 days. The results of this study shows significant and better results in the overall management of knee osteoarthritis, particularly in relieving pain, edema, stiffness and disability. The efficacy of treatment with cupping therapy in relieving signs and symptoms of knee osteoarthritis is comparable to that of acetaminophen 650 mg thrice a day orally, in terms of analgesia, anti-inflammatory and resolution of edema with minimal and temporary side-effects like echymosis and blister formation while as control drug has greater side-effects particularly on upper gastrointestinal tract. It is recommended that further studies are conducted with a larger study samples and of longer duration.
Keywords: Cupping therapy, knee osteoarthritis, regimenal therapy
INTRODUCTION
Regimenal therapy is a category of treatment modality that utilizes various mechanisms like massage, exercise and leeching etc., to change local and thereafter systemic hemodynamic. Cupping a component of regimenal therapy is utilized for local bloodletting and for local hemo dynamic changes. It ensures enhancement of tissue metabolism by increasing the blood circulation of that site.[1,2,3,4,5]
These chemical changes through physical procedures and subsequent diversion resulting in excretion from the site or body are known as Imala.[6,7]
Cupping is of three types; dry cupping is caused by creating a vacuum through mechanical means. Wet cupping utilizes a scarifier to cause bloodletting before or together with dry cupping, whereas, the third type uses fire to create the desired vacuum.[2,3,4,5]
In osteoarthritis, the proteoglycans synthesis rate is brought down from a half-life of weeks to a more rapid one whereas, that of collagen from a half-life of several years to a shorter period leading to chondriocystic loss. This loss is a result of disturbance in the three dimensional framework that holds the proteoglycans in collagen. Hence, there is a failure in repair of both proteoglycans and collagen.[8,9,10] Imala has the potential to change the chemical form of the compounds by breaking them into simpler ones and to change their chemical structure for example uric acid accumulated in tissues is changed to ureates or into uric acid excretable through urine.[7,6]
Osteoarthritis is the most common of all joint disorders and the most expensive in terms of productivity, both in terms of days lost from work and in terms of cost of treatment. Another disadvantage of the disease is the absence of treatment to prevent or ameliorate the basic process. Keeping the effects of cupping in mind the present study was conducted to evaluate the efficacy of cupping in osteoarthritis from a clinical point of view.
MATERIALS AND METHODS
Diagnosed cases of knee osteoarthritis attending the Pain Clinic at New Delhi were selected for the study after obtaining their written consent. Patients were randomly allocated either to test Group A or control Group B, The duration of the study was 8 months, whereas the duration of the treatment was 15 days.
A 15-day follow-up was conducted to determine longer term carryover of treatment effects utilizing both objective and subjective assessment. Measurements of subjects were taken pre-and post-test.
Inclusion Criteria
Subjects with osteoarthritis aged between 30 and 60 years old.
Subjects who did not receive cupping to the knee region before or to any other region of the body 6 months prior to the study.
Exclusion Criteria
Subjects with gross deformity.
Osteoarthritis of joints other than the knee.
The subjects fulfilling the criteria were randomly allotted Group A or B. Group A patients received cupping therapy whereas Group B was given Acetaminophen 650 mg thrice a day orally with water.
Basic Cupping therapy equipment was utilized including a hand suction pump, plastic cups of the same size and anti-septic tools.
The Procedure
The following procedure was adopted while performing cupping:
Prior to commencing application of treatment, we ensured that:
The subjects had complied with the pre-cupping requirements (inclusion criteria).
Contra-indications were eliminated
Equipment was sterilized
Subjects were explained and subsequently reassured regarding the temporary and minor side-effects such as echymosis and blister formation.
As per surface anatomy dry cupping was done on vastus lateralis, vastus intermedius, tibialis anterior and biceps femoris insertion laterally, medially it was done on tendons of Sartorious, gracilis and semitendinosus inferiorly and superiorly on vastus medialis[11] for 15 min.
Cupping was done on 0-6th day; 9-11th day and 14th day, i.e., 11 sittings in all.
Assessment Scales
Pain scale
G1 — No pain
G2 — Aching intermittent pain
G3 — Constant severe pain
G4 — Pain with restricted movement
G5 — Movement difficult without assistance
Stiffness scale
G1 — No stiffness
G2 — Occasional stiffness
G3 — Stiffness during flexion
G4 — Stiffness while climbing
G5 — Stiffness while walking
Tenderness scale
G1 — No tenderness
G2 — Occasional tenderness
G3 — Tenderness on flexion
G4 — Tenderness while climbing
G5 — Tenderness while walking
Movement disability scale
G1 — No movement disability
G2 — Occasional movement disability
G3 — Disability in flexion
G4 — Disability while climbing
G5 — Disability while walking
Edema scale
G1 — No edema
G2 — edema occasionally present
G3 — Moderate edema
G4 — Severe edema
Crepitation scale
G1 — No Crepitations
G2 — Crepitations occasionally present
G3 — Crepitations present all the time
Nocturnal pain scale
G1 — No Nocturnal Pain
G2 — Presence of Nocturnal Pain
Statistical Analysis
Results were assessed based on symptoms, signs which were graded accordingly. Calculations were done with Biostatistics software Graphpad instat 3.10 version by using Paired t-test. Percentage change was calculated by: (y2-y1)/y1 × 100 formula.
RESULTS
Group A
A total of 30 volunteers consented to take part in the study. Three volunteers dropped out because they were afraid of the echymosis. A total of 27 volunteers began the study; five volunteers dropped because of excessive pain and two volunteers were unable to attend the final three appointments and the remaining 20 volunteers completed the trial (n = 20).
Group B
A total of 32 patients were booked for the trial. Two volunteers dropped out as they found the treatment expensive. Thirty volunteers started the study of which two dropped because they felt the results were not satisfactory, whereas eight developed gastrointestinal symptoms and had to stop the study therefore 20 volunteers completed the trial (n = 20).
Epidemiological Data
Group A
The constitution of the twenty volunteers in the study was as follows: Male (n = 6, 30%), female (n = 14, 70%) as shown in Table 1 and Graph 1
Table 1.
Distribution of patients according to gender
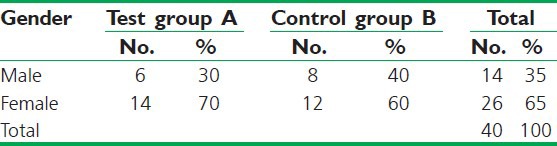
Graph 1.
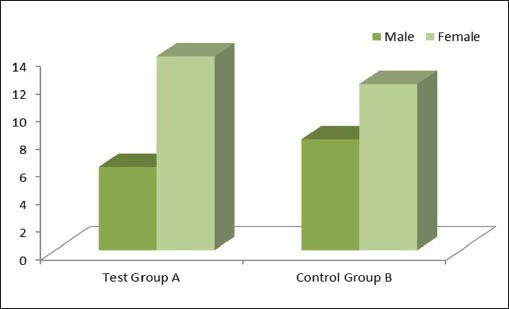
Gender
The patients belonging to age group 30-40 (n = 1, 5%) the patients of 40-50 years is n = 8.40%. 50-60 years n = 11, 55% as shown in Table 2 and Graph 2.
Table 2.
Distribution of patients according to age
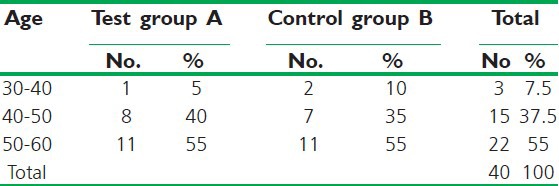
Graph 2.
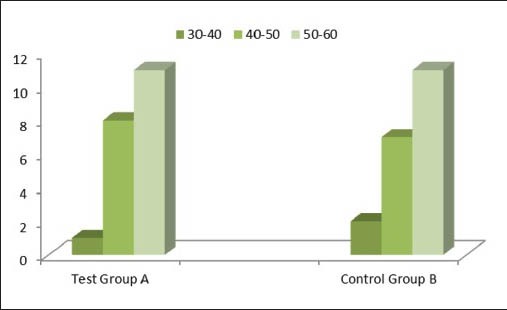
Age
Of the 20 patients, 13 (65%) patients reported joint stiffness and tenderness and whereas 10 (50%) patients reported movement disability. Majority of the patients gave a negative family history (n = 12 60%). As shown in Table 3 and Graph 3, 9 (45%) patients had edema and crepitations, while 3 (15%) had nocturnal aches at night, 2 (10%) had muscle wasting Tables 4 and Graph 4.
Table 3.
Distribution of patients according to family history
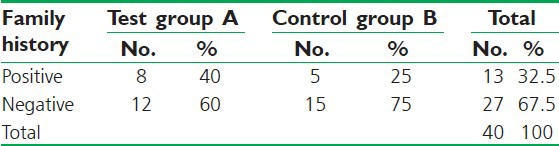
Graph 3.
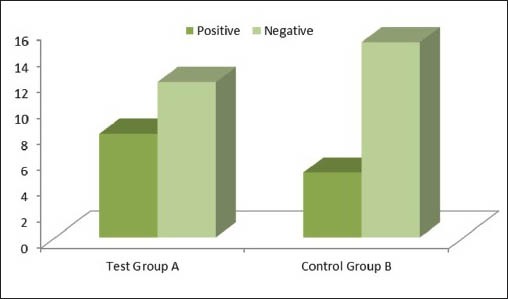
Family History
Table 4.
Distribution of patients according to muscle wasting
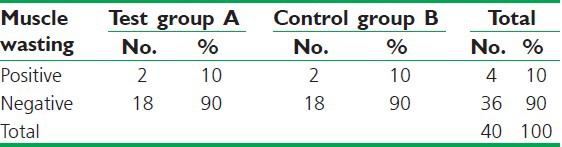
Graph 4.
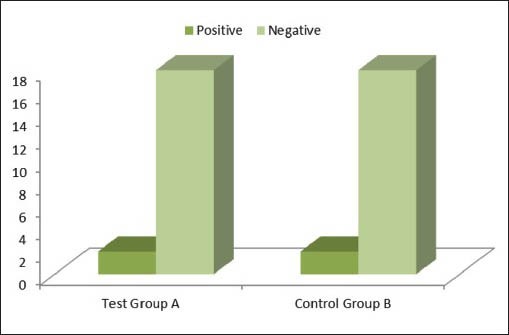
Muscle Wasting
Group B
The constitution of the twenty volunteers in the study was as follows: male (n = 8, 40%), female (n = 12, 60%) as shown in Table 1 and Graph 1.
The patients belonging to age group 30-40 (n = 2, 10%) the patients of 40-50 years is n = 7, 35%. 50-60 years n = 11, 55% as shown in Table 2 and Graph 2.
Of the 20 patients, 14 (70%) patients reported joint stiffness and tenderness and whereas; 11 (55%) patients reported movement disability. Majority of the patients gave a negative family history (n = 15 75%). 10 (50%) patients had edema and crepitations while. 6 (30%) had nocturnal aches at night. 2 (10%) had muscle wasting Table 4 and Graph 4.
Assessment of Efficacy
Effect on pain
The effect of both the cupping and acetaminophen was statistically extremely significant in relieving pain with P value in both the cases being <0.0001. The percentage change in pain after treatment for cupping group was observed as 46.37% while Group B had 43.055%. The comparable percentage change was 3.32% higher with Group A [Table 6, Graph 6].
Table 6.
Effect on pain
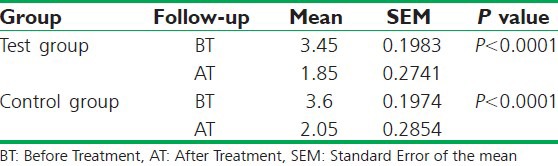
Graph 6.
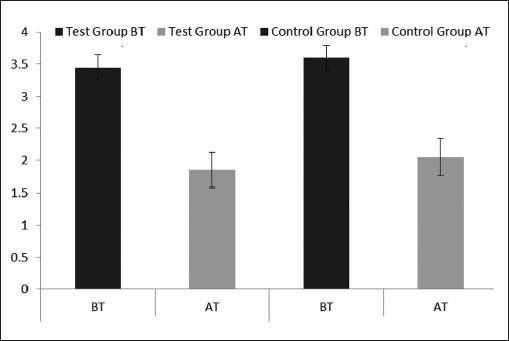
Pain
Effect on morning stiffness
The effect of both the cupping and acetaminophen was extremely significant with P value in both the cases being <0.0001. The percentage change for cupping group was observed as 49.09% while Group B had 42.30%. The comparable percentage change was 6.79% higher with Test Group A [Table 7, Graph 7].
Table 7.
Effect on morning stiffness
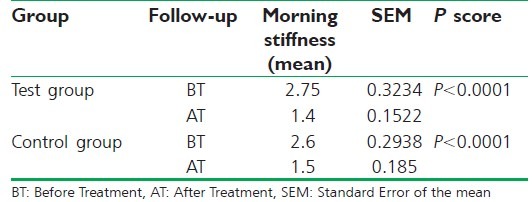
Graph 7.
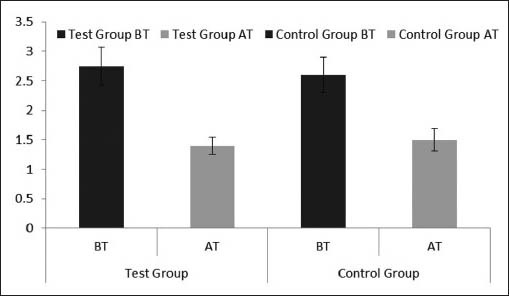
Morning Stiffness
Effect on tenderness
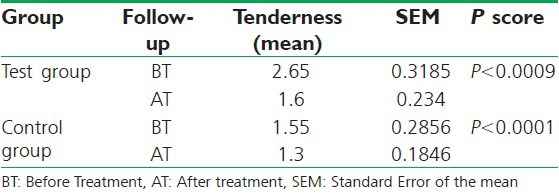
The effect of both the cupping and acetaminophen was extremely significant with P value in test Group A as <0.0009 whereas in the control Group B as <0.0001. The percentage change for cupping group was observed as 39.62% while Group B had 38%. The comparable percentage change was 1.62% higher with Group A [Table 8, Graph 8].
Table 8.
Effect on tenderness
Graph 8.
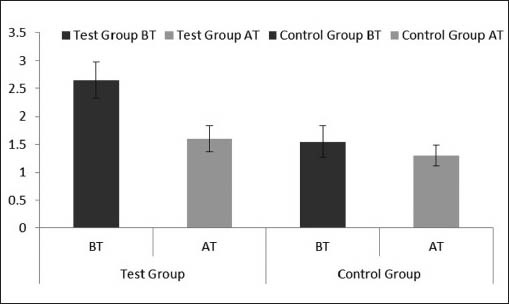
Tenderness
Effect on crepitations
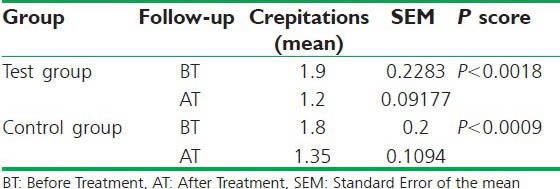
The effect of both the cupping and acetaminophen was extremely significant with P value in Group A < 0.0018, whereas in Group B was <0.0009. The percentage change for cupping group was observed as 36.84% while Group B had 25%. The comparable percentage change was 11.84% higher with Group A [Table 9, Graph 9].
Table 9.
Effect on crepitations
Graph 9.
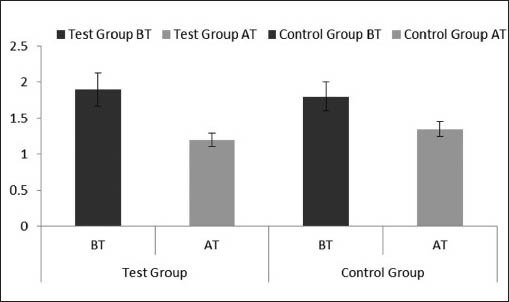
Crepitations
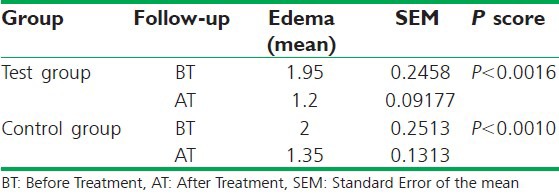
Effect on edema
The effect of both the cupping and acetaminophen was extremely significant with P value in Group A <0.0016, whereas in Group B was <0.0010. The percentage change for cupping group was observed as 38.46% while Group B had 32.5%. The comparable percentage change was 5.96% higher with Group A [Table 10, Graph 10].
Table 10.
Effect on edema
Graph 10.
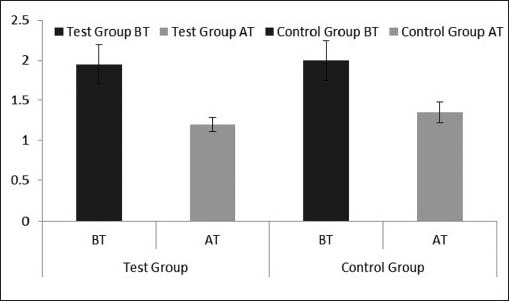
Edema
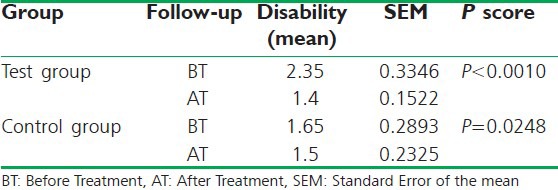
Effect on disability
The effect of both the cupping and acetaminophen was extremely significant with P value in Group A <0.0010, whereas in Group B was = 0.0248. The percentage change for cupping group was observed as 40.42% while Group B had 21.42%. The comparable percentage change was 19% higher with Group A [Table 11, Graph 11].
Table 11.
Effect on disability
Graph 11.
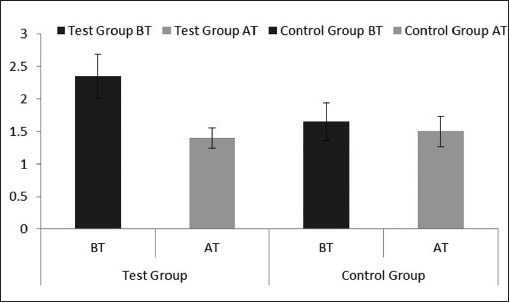
Disability
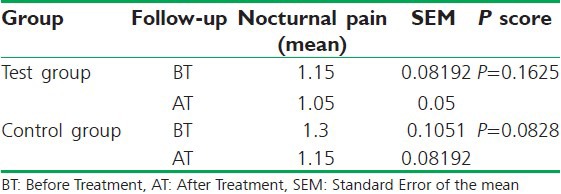
Effect on nocturnal pain
The effect of both the cupping and acetaminophen was extremely significant with P value in Group A =0.1625 whereas in Group B was =0.0828. The percentage change for cupping group was observed as 8.69% while Group B had 11.53%. The comparable percentage change was 2.84% higher with Group B [Table 12, Graph 12].
Table 12.
Effect on nocturnal pain
Graph 12.
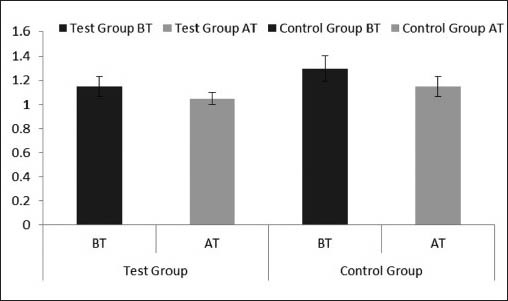
Nocturnal Pain
DISCUSSION
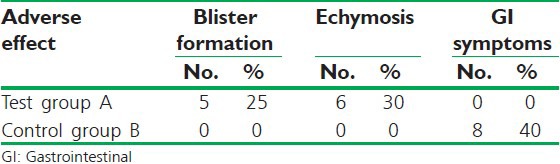
Cupping on the said sites ensured erythema, ecchymosis, release of sebum, water vapor and even blister formations. The erythema and ecchymosis were circular in shape and were directly proportional with symptomatic improvement. Blisters too appeared on the anterio medial aspect of the knee. The blisters gave the characteristic burning sensation and appearance of pressure blister. These varied in number from two to three to plentiful, i.e., 15 with straw colored fluid. The blisters were ruptured under aseptic conditions with a sterile needle. No further treatment was necessary for the blisters. The fluid from such blisters varied from 0.05 ml to 0.2 ml per sitting. The blistered site was given rest for a day or two for healing. The knee improved dramatically after blister formation especially in terms of edema, crepitations and stiffness. Blisters usually formed after 4 to 5 days of cupping. The blisters formed easily and larger in numbers during summers and under increased room temperature. Individuals reacted differently to the same amount of pressure, time of application and room temperature. Some gave severe ecchymosis where as others had blisters Table 5 and Graph 5 while some other had no changes at all. This difference in reaction can be attributed to:
Table 5.
Distribution of patients according to adverse effects
Graph 5.
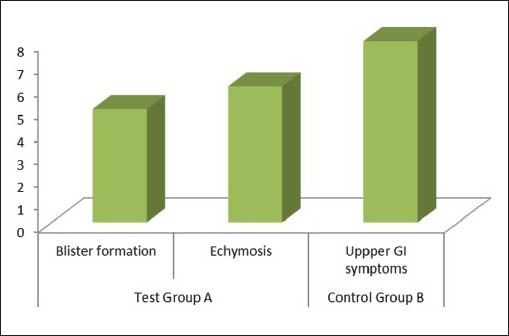
Adverse Effects
Personal temperament
Temperament of the Ma-adda ghair mehmooda or metabolites.
Fat deposition in the area. The fats deposited are inversely proportionate to the ecchymosis, blisters, etc.
The severity of disease — the amount of metabolites accumulated or the pathological changes since cupping ensures imala, the more the metabolites the more time is spend in diversifying them.
History of prior cupping — if the patient had been undergoing cupping for some time his metabolites are already in a state of movement.
Bathing or perspiration — if the patient has had a bath prior to cupping session. The water absorbed by the skin during bathing or post perspiration is excreted in the form of blisters during cupping sessions.
Local use of anti-inflammatory drugs — the anti-inflammatory drugs too cause a change in the metabolitic status of the joint.
The hemodynamic changes brought about through dry cupping are evident from ecchymosis and blister. These biochemical changes that resulted from vacuum are signs of imala. The vacuum pulls the muscle beyond its normal elastic limits and causes breeches in microvasculature of that area ensuring local hyperemia. Thus increasing the blood supply in the capillary system of that specific site. The metabolites that are diversified from the bony tissue towards muscle are taken up by the phagocytes from these capillary beds.
The patients on cupping therapy showed better results terms of pain, morning stiffness, tenderness, edema, crepitations and movement disability when compared with those on acetaminophen. However, patients of acetaminophen responded well to nocturnal pain when compared to those on cupping therapy.
The ecchymosis and blister formation are directly related to the duration and volume of negative pressure created by cupping and are usually the only undesired effects of cupping therapy for the patient besides causing a mild pain during the cupping session due to indrawing of tissues because of suction effect. But when the patient is taken into confidence and informed in advance of such effects and ensured about their transient nature than the patients are not bothered by their occurrence.
CONCLUSION
The study proved cupping to be a good analgesic and anti-inflammatory with efficacy better than acetaminophen. Thus, cupping can be recommended for other painful conditions besides being a line of treatment for osteoarthritis.
Cupping superimposes acute inflammation on chronic inflammation. The chronic inflammation of cartilage that is deep seated has acute inflammation on the skin and muscles. A study conducted by Pete et al. in Poland states that degenerative changes occurs as a result of decreased blood supply. Acute inflammation at a site 1-3 mm from the affected joint does improve the blood circulation of the site for a sustained period of 11 days shows the desired changes.
The effect of this at proteoglycans and collagen level needs evaluation to understand the pharmokinetics of vacuum of healthy and ailing tissue another aspect that needs further attention is the concept of healing by causing acute inflammation in tissue superior to chronic inflammation.
The initial increase in pain in Grade 3 and Grade 4 must be because the pain of osteoarthritis had restricted the use of these muscles and thereby causing a loss in their elasticity hence the additional burden on the elasticity caused pain.
Cupping also proved to be a good exercise to specific muscles besides improving their blood supply.
Footnotes
Source of Support: Nil
Conflict of Interest: Nil.
REFERENCES
- 1.Arzani MA. Lucknow: Matba Nami Grami Munshi Nawal Kishore; 1915. Mufarreh Quloob; pp. 583–8. [Google Scholar]
- 2.Baghdadi IH. Hyderabad: Matbaul Jamia Dairaul Maroof Ul Usmaniya; 1914. Kitab ul Mukhtaraat fit Tibb; pp. 297–9. 1326 H. [Google Scholar]
- 3.Masihi IA. 1st ed. Vol. 1. New Delhi: CCRUM; 1986. Kitab ul Umda fil Jarrah; pp. 194–200. [Google Scholar]
- 4.Razi Z. 1st ed. New Delhi: CCRUM; 1991. Kitab ul Mansoori; pp. 283–4. [Google Scholar]
- 5.Sinna I. Book I. Jamia Hamdard. Vol. 2. New Delhi: Department of Islamic Studies; 1993. Al Qanoon fit Tibb; pp. 364–7. [Google Scholar]
- 6.Arzani MA. Lucknow: Matba Nami Grami Munshi Nawal Kishore; 1915. Mufarreh Quloob; pp. 543–5. [Google Scholar]
- 7.Rushd I. 2nd ed. New Delhi: CCRUM; 1987. Kitab ul Kulliyat; pp. 106–10. [Google Scholar]
- 8.Thomas O, Schnitzer J. Vol. 2. Philadelphia: Harcourt Asia Pte. Ltd; 2000. Cecil's Text Book of Medicine; pp. 1550–2. [Google Scholar]
- 9.Nuki G. 17th ed. London: Churchil Livingstone; 1995. Davidson's Principles and Practice of Medicine; pp. 877–80. [Google Scholar]
- 10.Brandt KD. 14th ed. Vol. 2. New York: Philadelphia; 1998. Harrisons Principles of Internal Medicine; pp. 1692–7. [Google Scholar]
- 11.John S. 3rd ed. New York: Churchill Livingstone; 2003. Surface Anatomy; p. 103. [Google Scholar]