

Abstract
Laparoscopic adjustable gastric banding is a common and effective minimally invasive procedure in the treatment of morbid obesity. Common complications of the procedure include productive burping, ulceration, gastritis, erosion, slippage, problems with the port, bleeding and infection. We report a case of acute appendicitis caused by gastric banding in a female patient. Gastric band encircled the appendix causing lumen obstruction and infection. The patient developed symptoms of topical acute peritonitis and an appendisectomy was performed.
INTRODUCTION
Obesity is a medical condition in which excess body fat has accumulated to the extent that it may have an adverse effect on health, leading to reduced life expectancy and/or increased health problems. People are considered obese when their body mass index (BMI) exceeds 30 kg/m2 (Classification according to the ACS).
Obesity is one of the most common issues in modern medicine, especially among surgeons who develop methods for its treatment. Its global scale and the continuous growing number of obese people document the development of the global epidemic. Obese people have concurrent diseases such as diabetes, arterial hypertension, dyslipidaemia and diseases of the respiratory, circulatory and osteoarticular system. The relationship between obesity and numerous neoplasms has also been proven. Obesity is one of the leading preventable causes of death worldwide [1]. In the face of unsatisfactory conservative means, surgery plays an important part in obesity management. Advancing laparoscopic techniques, which are now a method of choice in bariatric surgery, led to development and increased popularity of bariatric procedures. Available treatment options include restrictive, malabsorptive or a combination of both. Many factors such as BMI, general performance status, age, concurrent diseases, operating theatre and ward equipment, and also the surgeon's skills and experience influence the decision about the technique. The surgery should be adjusted so that it guarantees the highest percentage of body weight loss with the minimal surgical risk. Laparoscopic adjustable gastric banding is still very popular among restrictive surgical techniques. At the moment, it is one of the most commonly performed bariatric procedures in the world.
The most commonly reported complications after gastric banding include productive burping, ulceration, gastritis, erosion, slippage, problems with the port, bleeding and infection [2, 3].
CASE REPORT
A 29-year-old female patient was admitted into the surgical department of Nicosia General Hospital because of a lower abdominal intermittent and cramping pain for the last 24 h. On physical examination, the patient had sensitivity during palpation at the lower abdomen, more predominant at the right iliac fossa. Rebound tenderness was absent during the first examination, as well as the rest of the signs of acute appendicitis. The patient had the following laboratory blood test results: WBC 9.25 × 109/l, neutrophils 69.3%, lymphocytes 20.0%, Mon 9.3%, HGB 9.7 g/dl, HcT 31.3%, MCV 69.4 fl, MCH 21.5 pg, MCHb 31.0 g/dl, PLT 220 × 109/l, glucose 116 mg/dl, urea 18 mg/dl, creatinine 0.8 g/l, Na 139 mmol/l, K 3.9 mmol/l, Tbil 0.81 mg/dl, ALP 61 U/l, γ-GT 8 U/l, AST 10 U/l, ALT 14 U/l, LDH 325 U/l and amylase 103 U/l. Urine test showed no urinary infection and pregnancy test was also negative. Plain chest and abdominal X-rays showed no pathology. Because of her persistent pain and the unclear symptoms that prevented a final diagnosis to be made, she had an ultrasound of the abdomen. The ultrasound revealed a small amount of fluid at the right iliac fossa, and revealed no other pathology of the appendix or any other internal organ. From her past medical history, a laparoscopic procedure for gastric band implantation due to obesity was recorded five years ago. The gastric band worked perfectly well and she lost about 30 kg. She did not complain for any abdominal pain that could be connected to the gastric band, and she did not have any symptoms from erosion or migration of the band. A small flip-over of the port of the gastric band was reported by the patient and it was noted on clinical examination.
After 2 days of hospitalization, observations and clinical examination, she developed acute peritonitis, so she was taken to the operating theatre. A sub-umbilical midline incision was executed to have a good access to the abdomen.
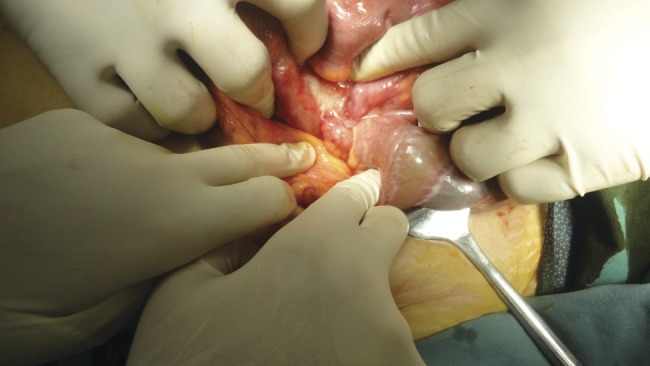
The peritoneal cavity was entered and the lower abdomen was thoroughly explored. Signs of infection were noted in the right iliac fossa. The appendix was attached to the ovary and pus was around them. During careful dissection, a strangulation of appendix's lumen from the tube of the gastric band was noted (Figs 1 and 2). The tube encircled the appendix and caused the intraluminal disruption that initiated the process of infection. We released the adhesions between the appendix and the tube and proceed to appendectomy. We then narrowed the length of the tube to prevent any future complications, e.g. intestinal obstruction, and thoroughly washed out the peritoneal cavity.
Figure 1:
The tube of the gastric band encircles the appendix causing obstruction and infection of the lumen.
Figure 2:

Removing the gastric band from the appendix.
DISCUSSION
Typical complications of gastric band implantation have already been frequently evaluated and presented. Among them, one can list erosion, fluid leakage, band slippage and migration. Additionally, there are complications associated with port and tube connection, for example, leakage, tubing rupture and disconnection. Last but not the least, we can encounter oesophageal dilatation, pouch dilatation and stomach stenosis [4].
In the literature, there are also a number of rare complications after implantation of gastric band. Salar et al. reported a single case of gastric band which caused gastric erosion, infection and migration through the pylorus-causing proximal jejunal obstruction [5].
Although intragastric migration of adjustable bands has widely been described, colonic erosion is extremely rare and has been described only in small case series [6]. Similarly, case studies have described band connection wire tubing constriction around small bowel or cecum causing bowel obstruction [7]. In one case study, a patient had severe diffuse abdominal pain in addition to port site pain as a result of traction by the band connection wire tube around the small bowel mesentery, pulling the mesentery into the right iliac fossa [8, 9,10].
We now report the first known acute appendicitis caused by the tube of the gastric band. The tube first encircled the appendix causing obstruction of its lumen. This was the first step that initiated the process of infection, due to the swelling of the lumen and bacterial overgrowth.
REFERENCES
- 1.Barness LA, Opitz JM, Gilbert-Barness E. Obesity: genetic, molecular, and environmental aspects. Am J Med Genet A. 2007;143A:3016–34. doi: 10.1002/ajmg.a.32035. doi:10.1002/ajmg.a.32035. [DOI] [PubMed] [Google Scholar]
- 2.Maggard M, Shugarman L, Suttorp M. LAP BAND Diet Guidelines. San Diego, CA: University of California, San Diego; UCSD Medical Center, Center for the Treatment of Obesity; 2007. [Google Scholar]
- 3.Cobourn C, Chapman MA, Ali A, Amrhein J. Five-year weight loss experience of outpatients receiving laparoscopic adjustable gastric band surgery. Obes Surg. 2013 doi: 10.1007/s11695-013-0881-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Zehetner J, Holzinger F, Triaca H, Klaiber Ch. A 6-year experience with the Swedish Adjustable Gastric Band: prospective long-term audit of laparoscopic gastric banding. Surg Endosc. 2005;19:21–8. doi: 10.1007/s00464-004-9015-6. doi:10.1007/s00464-004-9015-6. [DOI] [PubMed] [Google Scholar]
- 5.Salar O, Waraich N, Singh R, Awan A. Gastric band erosion, infection and migration causing jejunal obstruction. BMJ Case Rep. 2013 doi: 10.1136/bcr-2012-007737. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Liza BKT, Jimmy BYS, Shabbir A. Connection tubing causing small bowel obstruction and colonic erosion as a rare complication after laparoscopic gastric banding: a case report. J Med Case Rep. 2012;6:9. doi: 10.1186/1752-1947-6-9. doi:10.1186/1752-1947-6-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Strobos E, Antanavicius G, Josloff R. Unusual complication: small bowel obstruction caused by tubing of gastric band. Surg Obes Relat Dis. 2009;5:637–40. doi: 10.1016/j.soard.2009.04.013. [DOI] [PubMed] [Google Scholar]
- 8.Fass G, Simoens C, Mendes da Costa P. Diffuse abdominal and port site pain caused by the connecting tube in gastric banding. Obes Surg. 2008;20:1183–5. doi: 10.1007/s11695-008-9664-y. doi:10.1007/s11695-008-9664-y. [DOI] [PubMed] [Google Scholar]
- 9.Pischon T, Boeing H, Hoffmann K, Bergmann M, Schulze MB, Overvad K, et al. General and abdominal adiposity and risk of death in Europe. N Engl J Med. 2008;359:2105–20. doi: 10.1056/NEJMoa0801891. doi:10.1056/NEJMoa0801891. [DOI] [PubMed] [Google Scholar]
- 10.Haslam DW, James WP. Obesity. Lancet. 2005;366:1197–209. doi: 10.1016/S0140-6736(05)67483-1. doi:10.1016/S0140-6736(05)67483-1. [DOI] [PubMed] [Google Scholar]