

Abstract
Glial cell line-derived neurotrophic factor (GDNF) is a neurotrophic factor for dopaminergic neurons with promising therapeutic potential in Parkinson's disease. A few association analyses between GDNF gene polymorphisms and psychiatric disorders such as schizophrenia, attention deficit hyperactivity disorder and drug abuse have also been published but little is known about any effects of these polymorphisms on mood characteristics such as anxiety and depression. Here we present an association study between eight (rs1981844, rs3812047, rs3096140, rs2973041, rs2910702, rs1549250, rs2973050 and rs11111) GDNF single nucleotide polymorphisms (SNPs) and anxiety and depression scores measured by the Hospital Anxiety and Depression Scale (HADS) on 708 Caucasian young adults with no psychiatric history. Results of the allele-wise single marker association analyses provided significant effects of two single nucleotide polymorphisms on anxiety scores following the Bonferroni correction for multiple testing (p = 0.00070 and p = 0.00138 for rs3812047 and rs3096140, respectively), while no such result was obtained on depression scores. Haplotype analysis confirmed the role of these SNPs; mean anxiety scores raised according to the number of risk alleles present in the haplotypes (p = 0.00029). A significant sex-gene interaction was also observed since the effect of the rs3812047 A allele as a risk factor of anxiety was more pronounced in males. In conclusion, this is the first demonstration of a significant association between the GDNF gene and mood characteristics demonstrated by the association of two SNPs of the GDNF gene (rs3812047 and rs3096140) and individual variability of anxiety using self-report data from a non-clinical sample.
Introduction
Glial cell line-derived neurotrophic factor (GDNF), a member of the TGFβ superfamily that signals via cell-surface tyrosine kinase receptors, is considered an essential neuroprotective ligand for midbrain dopaminergic neurons [1] with promising clinical trials in Parkinson's disease [2]. As GDNF has also been shown to promote the development and differentiation of dopaminergic neurons [3] perturbed regulation of its expression has been supposed to underlie several neuropsychiatric diseases such as schizophrenia and depression via dysregulation of dopaminergic neural circuitries and impaired synaptic plasticity [4], [5].
Analysis of GDNF level changes in depressive disorders revealed contradictory results. Both elevated [11], [12] and reduced [13], [14] GDNF plasma concentrations have been reported in patients with late-onset depression, major depression or bipolar disorder. Antidepressants and electroconvulsive therapy seemed to enhance rat hippocampal [15] and human plasma GDNF levels [16], [17] possibly via altered epigenetic regulation of the GDNF promoter [18]. On the other hand, a recent post mortem analysis of human brain samples disclosed elevated GDNF protein levels in the parietal cortex but not in limbic areas and basal ganglia of patients with depressive disorder [19].
Recent genetic association studies on neurotrophic factors investigated the brain-derived neurotrophic factor (BDNF) and the neurotrophin-3 receptor gene demonstrating association with depression [6], anxiety disorders [7], [8] or attention deficit hyperactivity disorder [9]. Evidence was also provided for an interaction between dopaminergic (COMT) and neurotrophic (BDNF) gene variants influencing dysfunctional beliefs such as threat [10] which might be linked to anxiety. Interestingly, the potential etiopathological involvement of GDNF has rarely been addressed by genetic studies. A genome-wide linkage study has first shed light on the GDNF as potential candidate gene in schizophrenia [20], followed by contradictory results from case-control association studies [21], [22]. This issue has extensively been investigated later by Williams and co-workers [23]. They analyzed 9 SNPs (single nucleotide polymorphisms) encompassing the entire genetic locus as well as a poly-AGG repeat in the 3′ untranslated region, but neither of them proved to be significantly associated with schizophrenia. No associations have been found between GDNF SNPs and attention deficit hyperactivity disorder (ADHD) either [24], [25].
GDNF was also shown to have a protective effect against methamphetamine induced dopamine depletion related neurotoxicity [26]. In addition, a single nucleotide polymorphism (SNP) of GDNF (rs2910704) has recently been associated with methamphetamine dependence in a Japanese population [27]. Since mood disorders are often accompanied by drug abuse [28], and impaired dopaminergic signaling is a well-known factor in the pathogenesis of depression, we raised the question whether GDNF gene variants might be risk factors of depression or anxiety. To clarify this issue, here we present an association analysis between eight SNPs of the GDNF gene and mood characteristics assessed by the Hospital Anxiety and Depression Scale (HADS) questionnaire using data from 708 healthy Caucasians. To our best knowledge, this is the first study addressing the role of GDNF polymorphisms in anxiety and depression.
Subjects and Methods
Sample
Non related Caucasian (Hungarian) subjects participated on a voluntary basis from several educational facilities. They were recruited at the Institute of Psychology, Eötvös Loránd University. The study protocol was designed in accordance with guidelines of the Declaration of Helsinki, and was approved by the Scientific and Research Ethics Committee of the Medical Research Council (ETT TUKEB). The participants signed a written informed consent, provided buccal samples and filled out the Hospital Anxiety and Depression Scale (HADS). Selection criteria included no past or present psychiatric history (based on self-report), age between 18–35 years, valid GDNF SNP data for at least five of the eight analyzed SNPs and valid self-report data for the HADS subscales. A total of 837 independent samples were genotyped by the Open Array system, of which 767 subjects were between 18–35 years and 760 of them filled out the HADS self-report scale. All of these 760 subjects provided answers for at least six out of seven items in each HADS subscale, therefore valid scale data could be calculated. 708 of them had 5 or more GDNF genotypes providing the final study population. As a result, we analyzed data from 708 subjects (46.3% males, 53.7% females; mean age: 21.3±3.4 years). The sample comprised of 169 university students from the Institute of Psychology, Eotvos Lorand University, 217 college and university students from two law enforcement institutions in the Budapest area and 322 volunteers recruited on different occasions popularizing our research. Anxiety and depression scores (see Table S1 in File S1), as well as age and sex ratios (see Table 1) were different in these subgroups. On the other hand, genotype frequencies of GDNF SNPs were similar in the subgroups (see Table S2 in File S1), therefore the total sample was used for association analyses.
Table 1. Anxiety and depression in the three subject groups.
| Subject groups | N | Age | Male/female |
| Psychology students | 169 | 18–35 (20.32±2.74) | 16.6%/83.4% |
| Students in law enforcement | 217 | 18–35 (20.27±2.08) | 73.3%/26.3% |
| Other volunteers | 322 | 18–35 (22.57±3.96) | 43.5%/56.5% |
| Total sample | 708 | 18–35 (21.33±3.39) | 46.3%/53.7% |
Note. Range, mean values and StDev are provided for age.
Phenotype measures
All subjects completed the Hungarian version [29] of the Hospital Anxiety and Depression Scale (HADS). This self-report tool was originally developed by Zigmond and Snaith [30]. The questionnaire contains 14 intermixed items of two scales for detecting levels of anxiety (7 items) and depression (7 items). Both scales contain straightforward and reversed items to ensure attentive responses. Items are scored from 0–3 based on the releated response category (e.g. most of the time – not at all). The final raw score of both scales range from 0–21, sum of the appropiate items' scores. In the paper describing the Hungarian translation and validation of the HADS questionnaire [29] high internal consistency and discriminating power was found based on a sample of 715 Hungarian cancer patients. Concurrent validity of the HADS depression and anxiety scales has been attested with the Symptom List and the Beck Depression Scale. HADS anxiety scores increased with the number of anxiety-related emotional problems, such as ‘fears’, ‘nervousness’, and ‘worry’ and similarly increased HADS depression scores were found in those reporting ‘depression’ and ‘sadness’. Correlation of the depression scale of the HADS and the Beck Depression Scale (r = 0.81) also indicate sufficient concurrent validity.
The SNP selection criteria
Single nucleotide polymorphisms (SNPs) with a minor allele frequency (MAF) greater than 0.05 were selected from the Single Nucleotide Polymorphism database of NCBI (dbSNP). The pairwise tagging method using r2 threshold of 0.8 by Haploview was used to determine tagging SNPs based on HapMap data to obtain a proper coverage of the GDNF gene. SNPs with a reference from previous association studies concerning neuropsychiatric disorders were preferred.
Sample preparation and SNP genotyping
Collection of buccal swabs and isolation of genomic DNA was carried out as described in [24] with some modifications. Briefly, swabs were incubated in 450 µL lysis solution containing 0.2 g/L Proteinase K, 0.1 M NaCl, 0.5% SDS and 0.01 M Tris buffer, pH = 8 at 56°C overnight followed by RNase treatment at room temperature. Proteins were removed with saturated NaCl (2∶1 volume ratio). After the standard procedure of DNA precipitation with isopropanol and ethanol, the pellet was resuspended in 100 µL of 5 mM Tris pH = 8, 0.5 mM EDTA. Concentration of double stranded DNA was measured by fluorometry applying an intercalation assay (AccuBlue Broad Range dsDNA Quantification Kit, Biotium, Hayward). The range of the DNA concentration was 15–200 ng/µL, samples with lower than 15 ng/µL were not used for the OpenArray analysis.
Genotypes were determined applying the TaqMan® OpenArray™ Genotyping System (Applied Biosystems, Forster City, CA) based on sequence-specific, fluorescent TaqMan probes in combination with a high-throughput PCR system using nanoliter-scale sample volume and post-PCR (endpoint) detection. Genotyping platforms were obtained from the manufacturer as immobilized target specific primers and fluorescent probes in a low density array format. Reaction mixtures containing approximately 100 ng DNA (range: 30–150 ng) and the 1× master mix (each deoxyribonucleoside triphosphate and the AmpliTaq Gold DNA-polymerase, provided by the manufacturer) were prepared on a 384-well sample plate and then loaded on the genotyping plates by the OpenArray™ Autoloader. PCR amplification was performed in the GeneAmp® PCR System 9700 (Applied Biosystems, Forster City, CA) following the manufacturer's instruction. Endpoint imaging of the allele specific FAM and VIC fluorescent intensities was made by the OpenArray™ NT Imager. Raw data were evaluated by the TaqMan Genotyper v1.2 software.
2% of the DNA samples were repeatedly applied on the OpenArray system, demonstrating a 98,2% reproducibility. In addition, a subsample was re-genotyped for two SNPs (rs3812047, rs3096140) were re-genotyped with a 7300 Real-Time PCR System (Applied Biosystems, Foster City, CA) for quality control also providing an increase in the call rate of these SNPs. Original call rates of OpenArray™ Genotyping System are presented in Table S3 in File S1, while the call rates calculated for the final study population is given in Table 2. As it can be seen in these Tables, all the genotypes were in Hardy-Weinberg equilibrium.
Table 2. Genotype distribution of the studied GDNF polymorphisms.
| dbSNP No | Genotype | N | % | HWE* | Call rate |
| rs1981844 | GG | 313 | 55.1 | p = 0.537 | 80.2% |
| CG | 224 | 39.4 | |||
| CC | 31 | 5.5 | |||
| rs3812047 | GG | 542 | 76.6 | p = 0.962 | 100,0% |
| GA | 154 | 21.7 | |||
| AA | 12 | 1.7 | |||
| rs3096140 | TT | 316 | 48.0 | p = 0.928 | 92.9% |
| TC | 283 | 43.0 | |||
| CC | 59 | 9.0 | |||
| rs2973041 | AA | 488 | 70.6 | p = 0.727 | 97.6% |
| AG | 182 | 26.4 | |||
| GG | 21 | 3.0 | |||
| rs2910702 | AA | 380 | 54.8 | p = 0.911 | 98.0% |
| GA | 270 | 38.9 | |||
| GG | 44 | 6.3 | |||
| rs1549250 | TT | 235 | 33.5 | p = 0.970 | 99.0% |
| TG | 339 | 48.4 | |||
| GG | 127 | 18.1 | |||
| rs2973050 | CC | 237 | 40.6 | p = 0.340 | 82.3% |
| TC | 282 | 48.4 | |||
| TT | 64 | 11.0 | |||
| rs11111 | AA | 535 | 75.9 | p = 0.321 | 99,6% |
| AG | 153 | 21.7 | |||
| GG | 17 | 2.4 |
Note. * Hardy-Weinberg equilibrium.
Statistical Analysis
Statistical analyses were carried out using SPSS 20.0 for Windows. Chi-square analysis was used to test reliability of the measured genotype and allele frequencies. Lewontin's D' as well as R 2 values of linkage disequilibrium were determined using HaploView 4.2 [31]. Haplotypes were determined by the Phase program [32]–[34]. Independent-Samples t-test was used to assess sex differences; relationship with age has been tested by correlation analyses. One way analyses of covariance (ANCOVA) was used to test genetic associations of the single and multiple marker analyses in an allele-wise design. False positive results were ruled out by Bonferroni correction for multiple testing. The corrected level of significance was p<0.00313, as the nominal p (value 0.05) was divided by the number of analyses performed (8 SNPs ×2 HADS scales = 16). Two-way ANOVA was used for testing the effect of prior associations in males and females.
Genotypic and phenotypic data of the present study is publicly available through the NCBI dbGaP data repository: http://www.ncbi.nlm.nih.gov/gap.
Results
Reliability of the tested phenotypes and genotypes
Chronbach Alpha values were calculated to test the internal consistency of the self-report phenotypes. In the present sample reliability coefficients were satisfactory for both Anxiety (0.75) and Depression (0.68) scales. The Pearson's correlation coefficient was used to assess inter-correlation of the two scales: r = 0.54 (p<0.0001). Mean score of the anxiety scale was 5.80 (±3.54), with individual scores ranging from 0 to 19. Mean depression score was 2.75 (±2.55), with a range from 0 to 16. All polymorphisms were in Hardy-Weinberg equilibrium [35] as the p-values presented in Table 2 showed no significant differences between the distribution of observed and calculated genotype frequencies.
Age and sex as possible confounds
For testing sex differences on the two HADS scales Independent-Samples t-test was applied. Females showed significantly higher anxiety scores then males (6.47 compared to 5.02; t(706) = –5.55; p<0.001), thus sex was used as a covariant in all association analyses. Depression scores showed no significant sex difference. There was no significant correlation between HADS scales and age. This might be due to the relatively narrow age-range in our sample, as 90% of participants were between 18–25 years of age.
Association analyses of mood characteristics and GDNF polymorphisms
Table 3 summarizes results from the single marker analysis in both mood dimensions using one-way ANCOVAs with one of the GDNF SNPs as the grouping variable, with the HADS anxiety or the depression scale as the dependent variable and with sex as covariant. Association results for the 8 GDNF SNPs are represented in each row with the number of detected alleles, calculated MAF values, mean and standard deviation of anxiety and depression scores for carriers of the presented alleles and the corresponding p values from the ANCOVAs. Four SNPs (rs3812047, rs3096140, rs2910702, rs1549250) were associated with anxiety; scores were higher in the presence of the minor allele in all four cases. Corresponding statistical values for the above four SNPs labeled in bold in Table 3 were [F(1,1413) = 11.541, p = 0.0007, η2 = 0.008, power = 0.924]; [F(1,1313) = 10.282, p = 0.00138, η2 = 0.008, power = 0.893]; [F(1,1385) = 8.527, p = 0.00356, η2 = 0.006, power = 0.831]; and [F(1,1399) = 6.252, p = 0.01252, η2 = 0.004, power = 0.705], respectively. One GDNF SNP (rs1981844) showed association with the HADS depression scale, with higher scores in the presence of the minor allele [F(1,1133) = 5.086, p = 0.02431, η2 = 0.004, power = 0.615]. After correction for multiple testing, association of anxiety with rs3812047 and rs3096140 remained significant, labeled by single stars in Table 3. Mean anxiety was significantly higher in the presence of the minor (A) allele of the rs3812047 (6.68±3.72) as compared to the mean anxiety of major (G) allele carriers (5.68±3.50). The minor (C) allele of the rs3096140 was also a genetic risk factor of anxiety, as mean scores in the presence of this allele were higher (6.29±3.48) as compared to those with the major (T) allele (5.59±3.55). Both GDNF SNPs explained 0.8% of the variability of anxiety. Although the risk allele for anxiety was the minor allele for both SNPs, the number of participants in the study provided enough data points for association analyses with sufficient power (for rs3812047 MAF = 12.6%, N = 178; for rs3096140 MAF = 30.5%, N = 401).
Table 3. Association of GDNF polymorphisms and mood dimensions.
| Association analysis | |||||||
| dbSNP No | alleles | N | MAF** | Anxiety | p | Depression | p |
| rs1981844 | C | 286 | 0.252 | 6.16 (±3.87) | 0.07491 | 3.04 (±2.83) | 0.02431 |
| G | 850 | 5.71 (±3.41) | 2.64 (±2.53) | ||||
| rs3812047 | A | 178 | 0.126 | 6.68 (±3.72) | 0.00070* | 2.93 (±2.55) | 0.32941 |
| G | 1238 | 5.68 (±3.50) | 2.73 (±2.55) | ||||
| rs3096140 | C | 401 | 0.305 | 6.29 (±3.48) | 0.00138* | 2.80 (±2.51) | 0.76512 |
| T | 915 | 5.59 (±3.55) | 2.75 (±2.54) | ||||
| rs2973041 | G | 224 | 0.162 | 5.64 (±3.81) | 0.52321 | 3.01 (±2.81) | 0.08250 |
| A | 1158 | 5.80 (±3.50) | 2.69 (±2.51) | ||||
| rs2910702 | G | 358 | 0.258 | 6.27 (±3.62) | 0.00356 | 2.83 (±2.58) | 0.59415 |
| A | 1030 | 5.60 (±3.52) | 2.74 (±2.56) | ||||
| rs1549250 | G | 593 | 0.423 | 6.07 (±3.68) | 0.01252 | 2.90 (±2.67) | 0.05343 |
| T | 809 | 5.56 (±3.38) | 2.63 (±2.43) | ||||
| rs2973050 | T | 410 | 0.352 | 6.11 (±3.63) | 0.05656 | 2.85 (±2.69) | 0.39771 |
| C | 756 | 5.65 (±3.50) | 2.72 (±2.54) | ||||
| rs11111 | G | 187 | 0.133 | 5.78 (±3.86) | 0.84093 | 2.97 (±2.67) | 0.22126 |
| A | 1223 | 5.79 (±3.49) | 2.72 (±2.54) | ||||
Notes. *Significant after Bonferroni correction (p<0.00313) in single marker analyses. **MAF: minor allele frequency.
Since the law enforcement subgroup of our sample showed markedly lower anxiety mean scores than the subgroup of psychology students and other volunteers, we carried out two post-hoc analyses testing association of anxiety and the rs3812047 and rs3096140 GDNF polymorphisms without the law enforcement subgroup. Omitting this subgroup did not alter our previous findings using the total sample, the same pattern of risk alleles for increased anxiety was demonstrated: Mean anxiety score was higher (7.43±3.56) in the presence of the rs3812047 A allele as compared to 6.22(±3.38) in those carrying the rs3812047 G allele [F(1,903) = 12.358, p = 0.00046, η2 = 0.014, power = 0.940]. Similarly, in the presence of the rs3096140 C allele mean anxiety level was higher (6.74±3.25) than in the presence of the rs3096140 T allele (6.17±3.50), [F(1,837) = 4.682, p = 0.03077, η2 = 0.006, power = 0.580]. According to these results association of rs3812047 and rs3096140 GDNF polymorphisms with anxiety was consistent across participant subgroups.
Haplotype analysis
As the two SNPs (rs3812047 and rs3096140) significantly associated with anxiety after correction for multiple testing were not in linkage disequilibrium (D' = 13, r2 = 0; see Figure 1A and 1B), haplotype analysis was also performed. One-way ANCOVAs were applied on the two mood dimensions with the haploalleles as the grouping variable and sex as covariant (results are presented in Table 4). Effect of haplotypes on anxiety was significant [F(1,1415) = 6.323, p = 0.00029, η2 = 0.013, power = 0.967], while there was no significant differences in the mean scores of depression. Mean anxiety was lowest when formerly defined risk alleles were not present in the in the haplotype (5.49±3.45). When rs3096140C was present in the haploallele mean anxiety scores were notably higher (6.08±3.57). Anxiety scores were even higher when rs3812047A was present in the haploallele (6.50±4.04), and anxiety reached its highest average in the presence of both risk alleles in the haplotype (7.09±2.80).
Figure 1. Linkage disequilibrium plots for the studied GDNF SNPs.
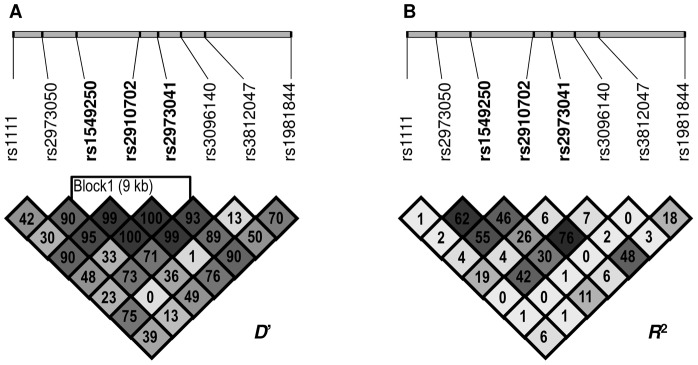
A: Lewontin's D' measure and B: R2 values of linkage disequilibrium. Higher values and darker squares indicate stronger pairwise linkage disequlibrium between two loci.
Table 4. Haplotype analysis of risk alleles.
| Haplotypes* | N | MAF** | Anxiety | p | Depression | p |
| rs3812047G_rs3096140T | 853 | 0,602 | 5.49 (±3.45) | 0.00029 | 2.72 (±2.60) | 0.804 |
| rs3812047G_rs3096140C | 385 | 0,272 | 6.08 (±3.57) | 2.74 (±2.46) | ||
| rs3812047A_rs3096140T | 125 | 0,088 | 6.50 (±4.04) | 2.90 (±2.53) | ||
| rs3812047A_rs3096140C | 53 | 0,037 | 7.09 (±2.80) | 2.98 (±2.64) |
Notes. *Risk alleles in the haplotypes are labeled by bold. **MAF: minor allele frequency.
Effect of GDNF risk alleles on male and female anxiety
There was a significant sex difference in HADS anxiety scores. In order to test if the significant genetic effects from our single marker analyses were different for males and females we used two-way ANOVAs on anxiety as the dependent variable and sex and presence or absence of the risk allele of one of the two SNP as grouping factors. Results are presented in Figure 2A and 2B. Main effect of the rs3812047 SNP was significant [F(1,1412) = 13.391, p = 0.0002, η2 = 0.009, power = 0.955] and as expected, we found a significant main effect of sex [F(1,1412) = 12.48, p = 0.0004, η2 = 0.009, power = 0.942]. Interestingly a significant interaction between sex and the rs3812047 SNP was also observed [F(1,1412) = 4.539, p = 0.033, η2 = 0.003, power = 0.567]. The effect of the minor (A) allele as a risk for higher anxiety was more pronounced in males as compared to females (Figure 2A).
Figure 2. Effect of GDNF risk alleles on male and female anxiety.

Mean HADS anxiety scores in females and males as a function of rs3812047 (A) and rs3096140 (B) alleles. Open markers denote females; closed markers denote males. Error bars represent standard errors of the mean.
Main effect of the rs3096140 SNP was also significant on anxiety [F(1,1312) = 9.664, p = 0.002, η2 = 0.007, power = 0.874], and we also found a significant sex effect [F(1,1312) = 49.233, p<0.0001, η2 = 0.036, power = 1.000]. However, for this GDNF SNP there was no significant gene-sex interaction. As presented in Figure 2B both males and females with the minor (C) allele showed higher anxiety.
Discussion
Evidence from twin studies confirms that mood characteristics have a considerable genetic component. Heritability of major depression is 37% [36], [37] and heritability of affective and anxiety disorders is around 45% [38]. The association between mood disorders and the monoamine system, especially the dopamine pathways, is well established [39]–[41], however, there are no prior reports on the effect of GDNF polymorphisms on mood characteristics in clinical or non-clinical populations.
The aim of the present study was to investigate any possible association of the GDNF gene polymorphisms with non-clinical individual variations of anxiety and depression. Several methods have been proposed to date for measuring mood characteristics (for recent reviews see: [42], [43]. In the present study we used the HADS questionnaire which has been translated to several languages [44] and is applicable to measure anxiety and depression in somatic, psychiatric and non-clinical samples [45]. We also demonstrated applicability of the HADS questionnaire in our previous genetic association findings, e.g. reporting association between polymorphisms of the P2RX7 gene and depression scores of diabetic patients [46] and patients with major depression or bipolar disorder [47].
Here we explored the association of 8 GDNF polymorphisms with anxiety and depression (Table 3). After correcting for multiple testing, the genetic effect on depression did not remain significant; however, two of the studied GDNF SNPs (rs3812047A and rs3096140C) were identified as possible risk alleles of anxiety (level of significance for the two associations were p = 0.00070 and 0.00138, respectively). We replicated these association findings using a subsample without the law enforcement subgroup, since they showed markedly lower anxiety mean scores than the subgroup of psychology students and other volunteers. Mean anxiety scores were higher in the presence of the rs3812047 A and the rs3096140 C risk alleles. According to these results association of rs3812047 and rs3096140 GDNF polymorphisms with anxiety was consistent across participant subgroups.
Since the two risk-SNPs were not in linkage disequilibrium we also performed haplotype analysis of these SNPs. Results described in Table 4 underlie the significant genetic effect indicated by our single-marker analyses: mean anxiety scores raised according to the number of risk alleles present in the haplotypes (p = 0.00029). It should be noted that anxiety and depression scales of the HADS questionnaire correlate (r = 0.54, p<0.0001) implicating that these two constructs are in close relation. One possible reason for the lack of significant effects of GDNF polymorphisms on depression in the present study is that depression scores were quite low in our non-clinical sample. This floor effect [48] might have reduced individual variation, and diminished genetic effects.
Findings from previous studies also confirm sex differences in anxiety. Higher anxiety of females was consistent according to a meta-analysis [49] with studies using a wide range of subject pool and anxiety measures (e.g. State-Trait Anxiety Inventory, Children's Manifest Anxiety Scale, Minnesota Multiphasic Personality Inventory). Anxiety disorders are also more frequent in females and more anxiety symptoms characterize them [50]. Neurotransmitter systems probably play an important role in the background of these differences [51], for example through the estrogen system increasing monoamine synthesis (dopamine, serotonin, norepinephrine) and receptor sensitivity [52]. Our results support these findings, as female subjects reported higher anxiety scores. However, we also report an interaction effect of sex and rs3812047 SNP on anxiety (Figure 2A). Males with the minor (A) allele showed anxiety scores as high as females with the major (G) allele of this polymorphism. Females with the risk (A) allele reported even higher anxiety scores. Others [53] also reported interaction effect of sex and the BDNF Val66Met polymorphism on stress reactivity.
Limitations of the presented study involve the relatively low sample size, therefore the possibility of false positive findings could not be excluded despite the fact that the two reported significant findings survived the Bonferroni-correction for multiple testing. Therefore further replications with independent samples are necessary. Moreover, no functional data are available concerning the intronic SNPs shown here to associate with anxiety, however, it is important to note that both anxiety-linked SNPs are in the close proximity of critical sites of alternative splicing (Figure 3.A. and B). Nevertheless, the fact that only these two SNPs associate firmly with anxiety might imply their significance in the control of gene expression. As far as the molecular background of this novel association is concerned, it is tempting to assume that these polymorphisms might be involved in the regulation of alternative splicing of the GDNF gene. Importantly, there are two main types of alternatively spliced preproGDNF isoforms, alpha and beta, the latter possessing a significantly shorter propeptide sequence due to the presence of an alternative splicing site in exon 3 of the gene [54], resulting in four isoforms as shown on Figure 3 B. Although the functional differences of GDNF variants are not fully understood, altered processing and secretion of the protein isoforms have been demonstrated [55]. This assumption seems highly probable in the light of recent publications assigning a pivotal role to intronic polymorphisms in governing splicing processes via differential recruitment of key splicing factors. For instance, two intronic SNPs in the type 2 dopamine receptor gene (DRD2) have been found sufficient to affect alternative splicing and therefore susceptibility to cocaine abuse [56]. Similar interactions between intronic SNPs and alternatively spliced isoforms have also been described in case of the human myocilin [57] and insulin [58] as well as the human papilloma virus E6/E7 genes [59], just to mention but a few.
Figure 3.

A. Localization of the analyzed human GDNF gene polymorphisms. Exons are labeled by filled boxes, the approximate position of the studied SNPs by filled triangles. SNPs showing significant association with anxiety after correction for multiple testing are in bold. ATG 1,2,3 and 4: alternative start sites, TGA: stop signal. B. Fine map of the genomic location of GDNF isoforms. Chromosomal positions of exons in each transcription variant are indicated at the bottom. (Please note, that introns are longer than they appear in the figure.) Arrows pointing up indicate the start and stop codons of open reading frames in each isoform. Chromosomal localization of rs3812047 and rs3096140 are shown on the top. Distance between exon 1 of variant 2 and rs3812047 is 99 bp, whereas exon 2 is 474 bp away from the polymorphic locus. Similarly, distance between exon 2 of isoform 1 or 3 and rs3096140 is 1915 bp, and exon 3 is 16596 bp away from the SNP.
Albeit several lines of biochemical evidence argue for the role of GDNF in dopaminergic differentiation [1], relatively scarce and ambiguous data have been gained from association studies with regard to its involvement in the pathogenesis of neuropsychiatric disorders. To date, a cohort of association analyses has suggested that certain GDNF polymorphisms might be linked to schizophrenia, a pervasive neurodevelopmental disorder [20], [23]. Recent findings from Ahmadiantehrani and Ron [60] seem to corroborate these results by revealing that upregulated DRD2 signaling, a hallmark of schizophrenia, resulted in elevated GDNF expression levels.
To our best knowledge, this is the first report shedding light on the significance of the rs3812047 and rs3096140 SNPs that have not been found to significantly associate with any known traits or disorders before. Previously, a study conducted on Japanese drug abusers identified a GDNF SNP associated with metamphetamine dependence [27]. It is widely known that anxiety disorders such as generalized anxiety disorder, phobias, panic- and compulsivity disorders are often accompanied by drug addiction, smoking and heavy drinking [61], [62]. In light of results presented here, GDNF might be one of the common factors that links anxiety to substance abuse.
This is the first report on association between anxiety and the polymorphisms of GDNF gene; however, since we used a non-clinical sample we could assess genetic background of individual variation in anxiety below the clinical threshold. Further studies are needed to reveal whether the genetic risk factors suggested here are related to higher vulnerability of mood disorders.
Supporting Information
Table S1. Anxiety and depression in the three subject groups. Table S2. Genotype frequencies of GDNF SNPs in the three subject groups. Table S3. Technical data of genotypes obtained by the OpenArray™ Genotyping System.
(DOCX)
Funding Statement
The Hungarian Scientific Research Funds (OTKA K81466 and K100845) and the Active Psychology Foundation has provided financial support. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- 1. Nitta A, Nishioka H, Fukumitsu H, Furukawa Y, Sugiura H, et al. (2004) Hydrophobic dipeptide Leu-Ile protects against neuronal death by inducing brain-derived neurotrophic factor and glial cell line-derived neurotrophic factor synthesis. J Neurosci Res 78: 250–258. [DOI] [PubMed] [Google Scholar]
- 2. Lang AE, Gill S, Patel NK, Lozano A, Nutt JG, et al. (2006) Randomized controlled trial of intraputamenal glial cell line-derived neurotrophic factor infusion in Parkinson disease. Ann Neurol 59: 459–466. [DOI] [PubMed] [Google Scholar]
- 3. Granholm AC, Reyland M, Albeck D, Sanders L, Gerhardt G, et al. (2000) Glial cell line-derived neurotrophic factor is essential for postnatal survival of midbrain dopamine neurons. J Neurosci 20: 3182–3190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Airaksinen MS, Saarma M (2002) The GDNF family: signalling, biological functions and therapeutic value. Nat Rev Neurosci 3: 383–394. [DOI] [PubMed] [Google Scholar]
- 5. Hudson J, Granholm AC, Gerhardt GA, Henry MA, Hoffman A, et al. (1995) Glial cell line-derived neurotrophic factor augments midbrain dopaminergic circuits in vivo. Brain Res Bull 36: 425–432. [DOI] [PubMed] [Google Scholar]
- 6. Cardoner N, Soria V, Gratacos M, Hernandez-Ribas R, Pujol J, et al. (2013) Val66met BDNF genotypes in melancholic depression: effects on brain structure and treatment outcome. Depress Anxiety 30: 225–233. [DOI] [PubMed] [Google Scholar]
- 7. Muinos-Gimeno M, Guidi M, Kagerbauer B, Martin-Santos R, Navines R, et al. (2009) Allele variants in functional MicroRNA target sites of the neurotrophin-3 receptor gene (NTRK3) as susceptibility factors for anxiety disorders. Hum Mutat 30: 1062–1071. [DOI] [PubMed] [Google Scholar]
- 8. Faludi G, Gonda X, Bagdy G, Dome P (2012) Pharmaco- and therapygenetic aspects in the treatment of anxiety disorders beyond the serotonergic system: a brief review. Neuropsychopharmacol Hung 14: 221–229. [PubMed] [Google Scholar]
- 9. Lasky-Su J, Neale BM, Franke B, Anney RJ, Zhou K, et al. (2008) Genome-wide association scan of quantitative traits for attention deficit hyperactivity disorder identifies novel associations and confirms candidate gene associations. Am J Med Genet B Neuropsychiatr Genet 147B: 1345–1354. [DOI] [PubMed] [Google Scholar]
- 10. Alonso P, Lopez-Sola C, Gratacos M, Fullana MA, Segalas C, et al. (2013) The interaction between Comt and Bdnf variants influences obsessive-compulsive-related dysfunctional beliefs. J Anxiety Disord 27: 321–327. [DOI] [PubMed] [Google Scholar]
- 11. Wang X, Hou Z, Yuan Y, Hou G, Liu Y, et al. (2011) Association study between plasma GDNF and cognitive function in late-onset depression. J Affect Disord 132: 418–421. [DOI] [PubMed] [Google Scholar]
- 12. Rosa AR, Frey BN, Andreazza AC, Cereser KM, Cunha AB, et al. (2006) Increased serum glial cell line-derived neurotrophic factor immunocontent during manic and depressive episodes in individuals with bipolar disorder. Neurosci Lett 407: 146–150. [DOI] [PubMed] [Google Scholar]
- 13. Tseng PT, Lee Y, Lin PY (2013) Age-associated decrease in serum glial cell line-derived neurotrophic factor levels in patients with major depressive disorder. Prog Neuropsychopharmacol Biol Psychiatry 40: 334–339. [DOI] [PubMed] [Google Scholar]
- 14. Diniz BS, Teixeira AL, Miranda AS, Talib LL, Gattaz WF, et al. (2012) Circulating Glial-derived neurotrophic factor is reduced in late-life depression. J Psychiatr Res 46: 135–139. [DOI] [PubMed] [Google Scholar]
- 15. Liu Q, Zhu HY, Li B, Wang YQ, Yu J, et al. (2012) Chronic clomipramine treatment restores hippocampal expression of glial cell line-derived neurotrophic factor in a rat model of depression. J Affect Disord 141: 367–372. [DOI] [PubMed] [Google Scholar]
- 16. Golan M, Schreiber G, Avissar S (2011) Antidepressants elevate GDNF expression and release from C(6) glioma cells in a beta-arrestin1-dependent, CREB interactive pathway. Int J Neuropsychopharmacol 14: 1289–1300. [DOI] [PubMed] [Google Scholar]
- 17. Zhang X, Zhang Z, Sha W, Xie C, Xi G, et al. (2010) Effect of treatment on serum glial cell line-derived neurotrophic factor in bipolar patients. J Affect Disord 126: 326–329. [DOI] [PubMed] [Google Scholar]
- 18. Uchida S, Hara K, Kobayashi A, Otsuki K, Yamagata H, et al. (2011) Epigenetic status of Gdnf in the ventral striatum determines susceptibility and adaptation to daily stressful events. Neuron 69: 359–372. [DOI] [PubMed] [Google Scholar]
- 19. Michel TM, Frangou S, Camara S, Thiemeyer D, Jecel J, et al. (2008) Altered glial cell line-derived neurotrophic factor (GDNF) concentrations in the brain of patients with depressive disorder: a comparative post-mortem study. Eur Psychiatry 23: 413–420. [DOI] [PubMed] [Google Scholar]
- 20. Suarez BK, Duan J, Sanders AR, Hinrichs AL, Jin CH, et al. (2006) Genomewide linkage scan of 409 European-ancestry and African American families with schizophrenia: suggestive evidence of linkage at 8p23.3-p21.2 and 11p13.1-q14.1 in the combined sample. Am J Hum Genet 78: 315–333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Lee K, Kunugi H, Nanko S (2001) Glial cell line-derived neurotrophic factor (GDNF) gene and schizophrenia: polymorphism screening and association analysis. Psychiatry Res 104: 11–17. [DOI] [PubMed] [Google Scholar]
- 22. Michelato A, Bonvicini C, Ventriglia M, Scassellati C, Randazzo R, et al. (2004) 3′ UTR (AGG)n repeat of glial cell line-derived neurotrophic factor (GDNF) gene polymorphism in schizophrenia. Neurosci Lett 357: 235–237. [DOI] [PubMed] [Google Scholar]
- 23. Williams HJ, Norton N, Peirce T, Dwyer S, Williams NM, et al. (2007) Association analysis of the glial cell line-derived neurotrophic factor (GDNF) gene in schizophrenia. Schizophr Res 97: 271–276. [DOI] [PubMed] [Google Scholar]
- 24. Boor K, Ronai Z, Nemoda Z, Gaszner P, Sasvari-Szekely M, et al. (2002) Noninvasive genotyping of dopamine receptor D4 (DRD4) using nanograms of DNA from substance-dependent patients. Curr Med Chem 9: 793–797. [DOI] [PubMed] [Google Scholar]
- 25. Syed Z, Dudbridge F, Kent L (2007) An investigation of the neurotrophic factor genes GDNF, NGF, and NT3 in susceptibility to ADHD. Am J Med Genet B Neuropsychiatr Genet 144B: 375–378. [DOI] [PubMed] [Google Scholar]
- 26. Cass WA, Peters LE, Harned ME, Seroogy KB (2006) Protection by GDNF and other trophic factors against the dopamine-depleting effects of neurotoxic doses of methamphetamine. Ann N Y Acad Sci 1074: 272–281. [DOI] [PubMed] [Google Scholar]
- 27. Yoshimura T, Usui H, Takahashi N, Yoshimi A, Saito S, et al. (2011) Association analysis of the GDNF gene with methamphetamine use disorder in a Japanese population. Prog Neuropsychopharmacol Biol Psychiatry 35: 1268–1272. [DOI] [PubMed] [Google Scholar]
- 28. Conway KP, Compton W, Stinson FS, Grant BF (2006) Lifetime comorbidity of DSM-IV mood and anxiety disorders and specific drug use disorders: results from the National Epidemiologic Survey on Alcohol and Related Conditions. J Clin Psychiatry 67: 247–257. [DOI] [PubMed] [Google Scholar]
- 29. Muszbek K, Szekely A, Balogh EM, Molnar M, Rohanszky M, et al. (2006) Validation of the Hungarian translation of Hospital Anxiety and Depression Scale. Qual Life Res 15: 761–766. [DOI] [PubMed] [Google Scholar]
- 30. Zigmond AS, Snaith RP (1983) The hospital anxiety and depression scale. Acta Psychiatr Scand 67: 361–370. [DOI] [PubMed] [Google Scholar]
- 31. Barrett JC, Fry B, Maller J, Daly MJ (2005) Haploview: analysis and visualization of LD and haplotype maps. Bioinformatics 21: 263–265. [DOI] [PubMed] [Google Scholar]
- 32. Stephens M, Donnelly P (2003) A comparison of bayesian methods for haplotype reconstruction from population genotype data. Am J Hum Genet 73: 1162–1169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Stephens M, J. Smith N, Donnelly P (2003) Documentation for PHASE, version 2.0.2.
- 34. Stephens M, Smith NJ, Donnelly P (2001) A new statistical method for haplotype reconstruction from population data. Am J Hum Genet 68: 978–989. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Hardy GH (1908) Mendelian Proportions in a Mixed Population. Science 28: 49–50. [DOI] [PubMed] [Google Scholar]
- 36. Sullivan PF, Neale MC, Kendler KS (2000) Genetic epidemiology of major depression: review and meta-analysis. Am J Psychiatry 157: 1552–1562. [DOI] [PubMed] [Google Scholar]
- 37. McGuffin P, Katz R, Watkins S, Rutherford J (1996) A hospital-based twin register of the heritability of DSM-IV unipolar depression. Arch Gen Psychiatry 53: 129–136. [DOI] [PubMed] [Google Scholar]
- 38. Stein MB, Jang KL, Livesley WJ (1999) Heritability of anxiety sensitivity: a twin study. Am J Psychiatry 156: 246–251. [DOI] [PubMed] [Google Scholar]
- 39. Serretti A, Smeraldi E (1999) Dopamine D2 receptor gene not associated with symptomatology of mood disorders. Am J Med Genet 88: 294–297. [PubMed] [Google Scholar]
- 40. Greenwood TA, Alexander M, Keck PE, McElroy S, Sadovnick AD, et al. (2001) Evidence for linkage disequilibrium between the dopamine transporter and bipolar disorder. Am J Med Genet 105: 145–151. [DOI] [PubMed] [Google Scholar]
- 41. Serretti A, Lilli R, Lorenzi C, Lattuada E, Smeraldi E (2001) DRD4 exon 3 variants associated with delusional symptomatology in major psychoses: a study on 2,011 affected subjects. Am J Med Genet 105: 283–290. [DOI] [PubMed] [Google Scholar]
- 42. Furukawa TA (2010) Assessment of mood: guides for clinicians. J Psychosom Res 68: 581–589. [DOI] [PubMed] [Google Scholar]
- 43. Smarr KL, Keefer AL (2011) Measures of depression and depressive symptoms: Beck Depression Inventory-II (BDI-II), Center for Epidemiologic Studies Depression Scale (CES-D), Geriatric Depression Scale (GDS), Hospital Anxiety and Depression Scale (HADS), and Patient Health Questionnaire-9 (PHQ-9). Arthritis Care Res (Hoboken) 63 Suppl 11S454–466. [DOI] [PubMed] [Google Scholar]
- 44. Herrmann C (1997) International experiences with the Hospital Anxiety and Depression Scale–a review of validation data and clinical results. J Psychosom Res 42: 17–41. [DOI] [PubMed] [Google Scholar]
- 45. Bjelland I, Dahl AA, Haug TT, Neckelmann D (2002) The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J Psychosom Res 52: 69–77. [DOI] [PubMed] [Google Scholar]
- 46. Nagy G, Ronai Z, Somogyi A, Sasvari-Szekely M, Rahman OA, et al. (2008) P2RX7 Gln460Arg polymorphism is associated with depression among diabetic patients. Prog Neuropsychopharmacol Biol Psychiatry 32: 1884–1888. [DOI] [PubMed] [Google Scholar]
- 47. Hejjas K, Szekely A, Domotor E, Halmai Z, Balogh G, et al. (2009) Association between depression and the Gln460Arg polymorphism of P2RX7 gene: a dimensional approach. Am J Med Genet B Neuropsychiatr Genet 150B: 295–299. [DOI] [PubMed] [Google Scholar]
- 48.Everitt BS (2002) The Cambridge dictionary of Statistics. New York: Cambridge University Press; Second Edition.
- 49. Feingold A (1994) Gender differences in personality: a meta-analysis. Psychol Bull 116: 429–456. [DOI] [PubMed] [Google Scholar]
- 50. Lewinsohn PM, Gotlib IH, Lewinsohn M, Seeley JR, Allen NB (1998) Gender differences in anxiety disorders and anxiety symptoms in adolescents. J Abnorm Psychol 107: 109–117. [DOI] [PubMed] [Google Scholar]
- 51. Pigott TA (1999) Gender differences in the epidemiology and treatment of anxiety disorders. J Clin Psychiatry 60 Suppl 184–15. [PubMed] [Google Scholar]
- 52. Halbreich U (1997) Hormonal interventions with psychopharmacological potential: an overview. Psychopharmacol Bull 33: 281–286. [PubMed] [Google Scholar]
- 53. Shalev I, Lerer E, Israel S, Uzefovsky F, Gritsenko I, et al. (2009) BDNF Val66Met polymorphism is associated with HPA axis reactivity to psychological stress characterized by genotype and gender interactions. Psychoneuroendocrinology 34: 382–388. [DOI] [PubMed] [Google Scholar]
- 54. Lonka-Nevalaita L, Lume M, Leppanen S, Jokitalo E, Peranen J, et al. (2010) Characterization of the intracellular localization, processing, and secretion of two glial cell line-derived neurotrophic factor splice isoforms. J Neurosci 30: 11403–11413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Grimm L, Holinski-Feder E, Teodoridis J, Scheffer B, Schindelhauer D, et al. (1998) Analysis of the human GDNF gene reveals an inducible promoter, three exons, a triplet repeat within the 3′-UTR and alternative splice products. Hum Mol Genet 7: 1873–1886. [DOI] [PubMed] [Google Scholar]
- 56. Moyer RA, Wang D, Papp AC, Smith RM, Duque L, et al. (2011) Intronic polymorphisms affecting alternative splicing of human dopamine D2 receptor are associated with cocaine abuse. Neuropsychopharmacology 36: 753–762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Pandaranayaka PJ, Prasanthi N, Kannabiran N, Rangachari K, Dhivya M, et al. (2010) Polymorphisms in an intronic region of the myocilin gene associated with primary open-angle glaucoma–a possible role for alternate splicing. Mol Vis 16: 2891–2902. [PMC free article] [PubMed] [Google Scholar]
- 58. Kralovicova J, Gaunt TR, Rodriguez S, Wood PJ, Day IN, et al. (2006) Variants in the human insulin gene that affect pre-mRNA splicing: is -23HphI a functional single nucleotide polymorphism at IDDM2? Diabetes 55: 260–264. [DOI] [PubMed] [Google Scholar]
- 59. Lopez-Urrutia E, Valdes J, Bonilla-Moreno R, Martinez-Salazar M, Martinez-Garcia M, et al. (2012) A few nucleotide polymorphisms are sufficient to recruit nuclear factors differentially to the intron 1 of HPV-16 intratypic variants. Virus Res 166: 43–53. [DOI] [PubMed] [Google Scholar]
- 60.Ahmadiantehrani S, Ron D (2013) Dopamine D2 Receptor Activation Leads To An Upregulation Of Glial Cell Line-Derived Neurotrophic Factor Via Gbetagamma-Erk1/2-Dependent Induction Of Zif268. J Neurochem. [DOI] [PMC free article] [PubMed]
- 61. Breslau N (1995) Psychiatric sequelae of low birth weight. Epidemiol Rev 17: 96–106. [DOI] [PubMed] [Google Scholar]
- 62. Farrell M, Howes S, Bebbington P, Brugha T, Jenkins R, et al. (2001) Nicotine, alcohol and drug dependence and psychiatric comorbidity. Results of a national household survey. Br J Psychiatry 179: 432–437. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. Anxiety and depression in the three subject groups. Table S2. Genotype frequencies of GDNF SNPs in the three subject groups. Table S3. Technical data of genotypes obtained by the OpenArray™ Genotyping System.
(DOCX)