

Abstract
AIM: To examine trends of uncontrolled total serum cholesterol, treatment and control in a Mediterranean region (Campania).
METHODS: We considered and compared the data collected as part of “Montecorvino Rovella Project” 1988-1989 and cross-sectional data from the two phases of the “VIP Project-Valle dell’Irno Prevenzione”: 1998-1999 (1st phase) and 2008-2009 (2nd phase), in the 35-74-year-old-population.
RESULTS: Data show a reduction of mean cholesterolemia in the last twenty years of 7.3 mg/dL for men and unchanged values for women. In the three surveys the mean values for serum cholesterol are in men: 205.2 ± 47.1 mg/dL (1988/89), 200 ± 38.9 mg/dL (1998/99) and 197.9 ± 40.2 mg/dL (2008/09); in the women: 203.1 ± 42.5 mg/dL (1988/89), 198.9 ± 37.9 mg/dL (1998/99) and 203.3 ± 39.3 mg/dL (2008/09). Prevalence of uncontrolled high cholesterol ≥ 240 mg/dL for men decreased from 20.8% (1988/89) to 14.3% (1998/99) and 13.9% (2008/9), P = 0.002; for women the values decreased from 19.9% (1988/89), to 18.2% (1998/99) and 18.1% (2008/09), P = 0.007. Is statistically increased the number of patients treated and those treated to target.
CONCLUSION: Encouraging increases in awareness, treatment, and control of hypercholesterolemia occurred from 1988 through 2008. Nevertheless, control of hypercholesterolemia remains poor.
Keywords: Mediterranean diet, Hypercholesterolemia, Drug, Heart disease, Southern Italy
Core tip: Risk of cardiovascular disease (CVD) is directly related to blood cholesterol levels. CVD due to atherosclerosis is the foremost cause of premature mortality and of disability-adjusted life years in Europe, and is also increasingly common in developing countries. The objective of this study was to examine trends of high cholesterol, treatment and control in a Mediterranean region (Campania). Data show a reduction of mean cholesterol in the last twenty years of 7.3 mg/dL for men and unchanged values for women. Encouraging increases in treatment and control of hypercholesterolemia occurred from 1988 through 2008. However, control of hypercholesterolemia remains poor.
INTRODUCTION
Coronary heart disease (CHD) is now the leading cause of death worldwide. It remains the major cause of premature death in Europe, even though CHD mortality has fallen considerably over recent decades in many European countries[1,2] .
Raised serum total cholesterol is an important cardiovascular risk factor, which causes an estimated 4.4 million deaths every year worldwide[3,4]. Research from the World Health Organization highlights the importance of raised blood cholesterol as a risk factor for CHD. The World Health Report 2002[5] estimates that around 8% of all disease burden in developed countries is caused by raised blood cholesterol and that over 60% of CHD and around 40% of ischaemic stroke in developed countries is due to total blood cholesterol levels in excess of the theoretical minimum (3.8 mmol/L). Variations in diet, especially consumption of animal-based vs plant-based fats, adiposity, and use of drugs to lower cholesterol have led to differences in serum cholesterol concentrations across populations and over time[6-8]. Therefore, the focus on cardiovascular prevention must remain high. Our aim was to estimate trend in total serum cholesterol, in a Mediterranean area of southern Italy, in the last twenty years.
MATERIALS AND METHODS
We compared the results of three epidemiological surveys as far as cardiovascular risk factors are concerned, performed in Southern Italy, in a Mediterranean region (Campania), in two areas near the city of Salerno.
In particular we considered and compared the data collected as part of “Montecorvino Rovella Project”[9] (PMR) 1988-1989 and cross-sectional data from the two phases of the “ VIP Project-Valle dell’Irno Prevenzione”: 1988-1989 (first phase)[10] and 2008-09 (second phase).
In three investigations, a sample taken from people between 25-74 years (divided into 5 classes of age: 25-34, 35-44, 45-54, 55-64, 65-74) was studied. People were enlisted at random from the electoral rolls and subjected to blood tests after an overnight fast.
The methodology of data collection and conducting tests to which the population underwent during the three phases are standardized and comparable, they have been fully described in some other publications[9-11].
PMR and VIP were conducted by the same working group and the same coordinator. Areas over district level, are similar for geographic position, they both are about 20 km far from Salerno. Moreover the socio-economic status of the rural populations and their recent industrial development are similar.
PMR project design
PMR project had the following aims: to analyze the prevalence of cardiovascular risk factors in an area of the Campania region at the end of 1980s. This study was conducted between 1988 and 1989, inviting a randomized statistical sample to represent the area. Randomized samples included 1500 subjects, 300 (150 males and 150 females) for each decade. Only 1091 subjects (569 females and 522 males) were examined with a total participation of 72.7% (75.9% for females and 69.6% for males).
VIP project design
VIP project has the following aims: to conduct a program of cardiovascular prevention in a population of the Irno Valley controlled by Mercato S. Severino’s Hospital, to know the physiological limits and biohumoral parameters of the resident population, to know the trend of the main cardiovascular risk factors in the area near Salerno. This study has collected epidemiological data on cardiovascular risk factors in two phases: 1998/99 and 2008/09. The “VIP Project” is a part of CINDI program, WHO study[12,13] and has contributed to the Global Burden of Metabolic Risk Factors of Chronic Diseases Collaborating Group[14]. Both surveys include 1200 subjects, 600 males and 600 females, age ranging from 25 to 74 years, randomized from the electoral rolls of the towns of Mercato S Severino and Baronissi, near Salerno, in Southern Italy. In a randomized way, we compiled three lists, each one of 120 subjects divided into decades of sex and age. The recruitment from the first list was realized by letter of invitation, in the case of impossibility or refusal, the subject was replaced by a person of the same age and sex from the second list and in the case of failure, someone from the third list. This type of procedure for the recruitment was suggested by the manual of the rules of monica project-monica cardiovascular diseases[15]. During all phases the subjects underwent to: (1) General examination; (2) Ecording of blood pressure; (3) Anthropometric measurements (weight, height, waist-hip ratio); (4) Electrocardiogram; and (5) Laboratory tests (total cholesterol, LDL cholesterol, HDL cholesterol, triglycerides, blood glucose, blood count, platelets, plasma insulin, fibrinogen, creatinine, C3).
Fasting venous blood was taken in the seated position without stasis after an overnight fast. The laboratory has always made use of quality control: Biorad (in 1988/89 and 1998/99) and VEQ (University Hospital of Bologna, Policlinico S. Orsola Malpighi) in 2008/09.
In particular, with regard to the parameters analyzed, cholesterol, HDL cholesterol, triglycerides were determined through an enzymatic method (Fixed-time to 500 nanometer) installed on Cobas-ABX (Roche, Milan Italy) automatic line.
A history, with a focus on cardiovascular disease, was performed by a physician who, through a questionnaire, also evaluated: the habit of cigarette smoking, physical activity, occupation, and level of education, the educational qualification of the partners, civil status, and regular use of pharmacological therapy.
Statistical analysis
Results are expressed as mean ± SD for continuous variables and as frequency distributions for the categorical ones. The data have been standardized using the direct method considering the European population standards of reference. To compare the means among the three groups, we used one-way analysis of variance and Bonferroni’s test for the differences among the groups. χ2 analysis was used to compare prevalences. P < 0.05 was considered significant.
RESULTS
Table 1 show age-specific levels of lipid pattern in the VIP Study 2008/09. The data from the previous surveys were published in a previous work[16]. Mean values of cholesterolaemia are higher in women, with a statistically significant difference (P = 0.02). The values of HDL are, in all decades, higher in females (except in the 65-74 years), with more marked differences for age groups 35-44 and 45-54 years.
Table 1.
Mean ± SD of cholesterol, high density-cholesterol, low density lipoprotein-cholesterol and triglycerides
| Age (yr) | Cholesterol (mg/dL) | HDL-C (mg/dL) | LDL-C (mg/dL) | Triglycerides (mg/dL) | |
| Male | 25-34 | 191.9 ± 41.6 | 45.1 ± 10.1 | 125.2 ± 35.5 | 114.6 ± 78.9 |
| 35-44 | 206.8 ± 39.7 | 48.4 ± 12.5 | 131.3 ± 35 | 136.7 ± 77.3 | |
| 45-54 | 197.9 ± 40 | 55.7 ± 13.9 | 117.8 ± 34.6 | 122.2 ± 70.9 | |
| 55-64 | 195.6 ± 31.6 | 49.4 ± 12.6 | 120.2 ± 31.9 | 130.2 ± 62.7 | |
| 65-74 | 196 ± 45.5 | 52.4 ± 12.4 | 119.5 ± 39 | 118.9 ± 69.9 | |
| 25-741 | 197.9 ± 40.2 | 50 ± 12.3 | 123.3 ± 34.9 | 124.9 ± 72.6 | |
| Female | 25-34 | 201.1 ± 37.6 | 47.8 ± 11.4 | 131.0 ± 34.7 | 111.5 ± 71.7 |
| 35-44 | 206.7 ± 41.4 | 52.5 ± 14.9 | 130.3 ± 37.7 | 119.6 ± 65.3 | |
| 45-54 | 203.7 ± 38.3 | 59.7 ± 13.7 | 120.9 ± 33.1 | 115.8 ± 72.7 | |
| 55-64 | 206.2 ± 38.8 | 52.4 ± 12.7 | 125.3 ± 34.2 | 142.6 ± 74.7 | |
| 65-74 | 195.6 ± 41.4 | 51.9 ± 12.4 | 119.8 ± 34.7 | 119.2 ± 67.1 | |
| 25-741 | 203.3 ± 39.3 | 53.0 ± 13.1 | 126.1 ± 34.9 | 121.0 ± 70.5 |
Data standardized to the European population. VIP Study 2008/09 (120 subjects by age group). HDL: High density lipoprotein; LDL: Low density lipoprotein.
The values of LDL cholesterol are similar between men and women: 123.3 ± 34.9 and 126.1 ± 34.9 (P = NS) whereas for the age groups 25-34 and 55-64 years, are higher in women. Regarding triglycerides mean values were found to be higher for men in the first three age groups but less in the last two decades. The highest values are recorded in the 35-44 years for male and in the 55-64 years for women. Table 2 shows the percentiles of lipidic pattern.
Table 2.
Percentiles of cholesterol, high density-cholesterol, low density lipoprotein-cholesterol and triglycerides (mg/dL) for both sexes
| Percentiles |
Cholesterol |
LDL-C |
HDL-C |
Triglycerides |
||||
| M | F | M | F | M | F | M | F | |
| 5° | 136 | 137 | 70 | 70 | 32 | 34 | 47 | 49 |
| 25° | 169 | 175 | 98 | 101 | 40 | 43 | 75.5 | 76 |
| 50° | 196.5 | 201 | 121 | 123.5 | 49 | 52 | 105.5 | 104.5 |
| 75° | 222 | 229.5 | 143 | 146.5 | 57 | 60 | 151 | 145 |
| 95° | 267 | 270 | 189.5 | 182.5 | 72.5 | 79.5 | 256 | 235 |
M: Male; F: Female. HDL: High density lipoprotein; LDL: Low density lipoprotein.
Figure 1 show age-specific levels of total serum cholesterol for PMR (1988/89) and two phases of VIP studies (1998/99 and 2008/09). The mean values (standardized to the European population) are in the male: 205.2 ± 47.1 (1988/89), 200 ± 38.9 (1998/99) and 197.9 ± 40.2 (2008/09); in the female: 203.1 ± 42.5 (1988/89), 198.9 ± 37.9 (1998/99) and 203.3 ± 39.3 (2008/09). Is evident a reduction of cholesterol in the last twenty years of 7.3 mg/dL for men and unchanged values for female. In both of sexes it is clear a reduction in cholesterol values after 45 years.
Figure 1.
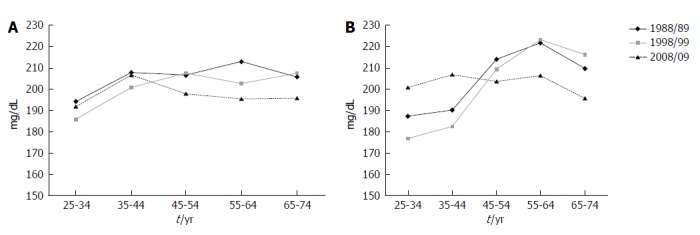
Cholesterolaemia between 25-74 years: 1988/89-2008/09. A: Male; B: Female.
Table 3 shows prevalence of uncontrolled high cholesterol. The trend is decreasing for both men and women. The decrease was greater in men. Table 3 also shows the percentage of patients treated to target. The hypercholesterolemic to target increased, statistically significant, in both sexes.
Table 3.
Prevalence of ipercholesterolaemia
| Group1 1988-89 | Group2 1998-99 | Group3 2008-09 | P value | 1 vs 3 | 1 vs 2 | 2 vs 3 | |
| (n = 522) | (n = 600) | (n = 600) | |||||
| Male | |||||||
| Uncontrolled high cholesterol (≥ 240 mg/dL) | 20.80% | 14.30% | 13.9% | 0.002 | < 0.05 | < 0.05 | NS |
| Hypercholesterolemia | 20.80% | 16.40% | 21.1% | NS | |||
| Treated hypercholesterolaemia | - | 2.50% | 40.8% | 0.000 | |||
| Treated to target | - | 84% | 91.0% | 0.000 | |||
| Hypercholesterolaemia to target | - | 12.80% | 37% | 0.000 | |||
| Female | |||||||
| Uncontrolled high cholesterol (≥ 240 mg/dL) | 19.90% | 18.20% | 18.1% | 0.007 | < 0.05 | < 0.05 | NS |
| Hypercholesterolemia | 19.90% | 18.90% | 25.8% | NS | |||
| Treated hypercholesterolaemia | - | 7.90% | 39.1% | 0.000 | |||
| Treated to target | - | 46.70% | 80.2% | 0.000 | |||
| Hypercholesterolaemia to target | - | 3.70% | 37% | 0.000 |
Data standardized to the European population; Men and women. Uncontrolled high cholesterol (≥ 240 mg/dL): Subjects with Cholesterolaemia ≥ 240 mg/dL, may or may not have been taking medication; Hypercholesterolemia: Subjects with cholesterol ≥ 240 + cholesterol-lowering therapy subjects; Treated hypercholesterolaemia: Treated/Hypercholesterolemia; Treated to target: Treated to target (cholesterol < 240 mg/dL)/all subjects treated; Hypercholesterolaemia to target: (Hypercholesterolemia < 240 mg/dL/subject with hypercholesterolemia). NS: Non-significant.
DISCUSSION
Hypercholesterolemia is undoubtedly one of the major risk factors of cardiovascular disease. Knowing its trend is particularly important for prevention strategies and to evaluate the effectiveness of interventions.
In Southern Italy, the cholesterol value, in the years between 1950 and 1960, was one of the lowest in the world[17]. Our country is the place where the practice of the Mediterranean Diet was born and developed. Successively, high consumption of saturated fats and low use of vegetable fibres that had as a consequence an increase of cholesterol until the beginning of 1990[18]. In those years, a greater attention to risk factors, the return to a more balanced nutrition, and use of statins have led to important change in the trend. Our data show a favorable trend, similar to that registered in other parts of the world, including North America and Western European countries[7,14,19,20]. We have observed a more favorable trend in the male population, consequence of a difference between the two sexes in percentage of treated hypercholesterolemic (48% in male and 39.1% in female) and in reaching an acceptable target (91% in male and 80.2% in female). This can be explained probably by considering a more direct drug intervention in the male population than in the female one. A therapeutic attitude more aggressive in men than in women is clearly described in the literature[21,22].
Another interesting observation is that, in the period before the statins, the cholesterol curves showed a reduction only after 65 years, due to the fact that subjects with high cholesterol die more easily[9]. Today, with statins, the distribution of cholesterol is reduced already after 45 years to stay then essentially unchanged.
Recently, the Global Burden of Metabolic Risk Factors of Chronic Diseases Collaborating Group has published the trend at national, regional and global cholesterol[14].
These data provide an interesting point of comparison to analyze the data of our study. Globally, mean total cholesterol changed little between 1980 and 2008, falling by less than 3.9 mg/dL per decade in both sexes. In our population the mean cholesterol was steadily declining in men (7.3 mg/dL) while substantially constant in women, with a decrease in the survey of the 1998/99 before recovering to the initial values. An exception is the age group 64-75 years, where there is a decrease of over 20 years, 14 mg/dL, and this is probably related to the increased use of statins in the population more adult. Doing an analysis for areas, total cholesterol decreased among high-income territories formed by Australia, North America, Western Europe, Central and Eastern Europe regional. The decreases were approximately 7.7 mg/dL per decade in both sexes. In the population of the VIP Project we find a smaller reduction: 3.7 mg/dL per decade in men and non-reduction for women. Despite this, serum total cholesterol in 2008 was higher in high-income countries; the regional mean was 202.2 mg/dL for men (in our population are slightly lower: 197 mg/dL) and 201.8 mg/dL for female (the values of the VIP project are slightly higher: 203.3 mg/dL). It was lowest in sub-Saharan Africa at 157.45 mg/dL in men and 164.8 mg/dL for female. Thus, there is evidence of a trend in the reduction of cholesterol levels in many areas of the world, as confirmed by our data, but we must undoubtedly increase interventions (particularly in women) because this result could be more obvious. The intervention must be conducted in two directions: encourage healthy diets, with unsaturated fats and extending and optimizing therapy with statins in the population at greatest risk[23-25].
COMMENTS
Background
Coronary heart disease (CHD) is now the leading cause of death worldwide. Raised serum total cholesterol is an important cardiovascular risk factor, which causes an estimated 4.4 million deaths every year worldwide. Therefore, the focus on cardiovascular prevention must remain high. The aim was to estimate trend in total serum cholesterol, in a Mediterranean area of southern Italy, in the last twenty years. In particular the authors considered and compared the data collected as part of “Montecorvino Rovella Project ” 1988-1989 and cross-sectional data from the two phases of the “VIP Project-Valle dell Irno Prevenzione”: 1988-1989 (1st phase) and 2008-2009 (2nd phase). Data show a reduction of mean cholesterol in the last twenty years of 7.3 mg/dL for men and unchanged values for women. Is statistically increased the number of patients treated and those treated to target.
Research frontiers
Research from the World Health Organization highlights the importance of raised blood cholesterol as a risk factor for CHD. In Southern Italy, the cholesterol value, in the years between 1950 and 1960, was one of the lowest in the world. The authors’ country is the place where the practice of the Mediterranean Diet was born and developed. Successively, high consumption of saturated fats and low use of vegetable fibres that had as a consequence an increase of cholesterol until the beginning of 1990. Successively, high consumption of saturated fats and low use of vegetable fibres that had as a consequence an increase of cholesterol until the beginning of 1990. In those years, a greater attention to risk factors, the return to a more balanced nutrition, and use of statins have led to important change in the trend. The data show a favorable trend, similar to that registered in other parts of the world, including North America and Western European countries.
Innovations and breakthroughs
The authors have observed a more favorable trend in the male population, consequence of a difference between the two sexes in percentage of treated hypercholesterolemics (48% in male and 39.1% in female) and in reaching an acceptable target (91% in male and 80.2% in female). This can be explained probably by considering a more direct drug intervention in the male population than in the female one. A therapeutic attitude more aggressive in men than in women is clearly described in the literature. Another interesting observation is that, in the period before the statins, the cholesterol curves showed a reduction only after 65 years, due to the fact that subjects with high cholesterol die more easily. Today, with statins, the distribution of cholesterol is reduced already after 45 years to stay then essentially unchanged.
Applications
There is evidence of a trend in the reduction of cholesterol levels in many areas of the world, as confirmed by our data, but the authors must undoubtedly increase interventions (particularly in women) because this result could be more obvious. The intervention must be conducted in two directions: encourage healthy diets, with unsaturated fats and extending and optimizing therapy with statins in the population at greatest risk.
Terminology
The World Health Report 2002 estimates that around 8% of all disease burdens in developed countries is caused by raised blood cholesterol and that over 60% of CHD and around 40% of ischaemic stroke in developed countries is due to total blood cholesterol levels in excess of the theoretical minimum (3.8 mmol/L). Variations in diet, especially consumption of animal-based vs plant-based fats, adiposity, and use of drugs to lower cholesterol have led to differences in serum cholesterol concentrations across populations and over time.
Peer review
The authors are dealing with an interesting topic, as the regulation of risk factors and the related communities planning are the best way to fight cardiovascular disease. The objective of this study was to examine trends of uncontrolled serum total cholesterol, treatment and control in a Mediterranean region (Campania). Data show a reduction of mean cholesterol in the last 20 years of 7.3 mg/dL for men and unchanged valves for women. Encouraging increases in awareness, treatment, and control of hypercholesterolemia occurred from 1988 through 2008.
Footnotes
P- Reviewers: LinHJ, Simkhovich B, Tagarakis G S- Editor: Qi Y L- Editor: A E- Editor: Wang CH
References
- 1.Nichols M, Townsend N, Scarborough P, Rayner M. Trends in age-specific coronary heart disease mortality in the European Union over three decades: 1980-2009. Eur Heart J. 2013;34:3017–3027. doi: 10.1093/eurheartj/eht159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Perk J, De Backer G, Gohlke H, Graham I, Reiner Z, Verschuren M, Albus C, Benlian P, Boysen G, Cifkova R, et al. European Association for Cardiovascular Prevention & Rehabilitation (EACPR); ESC Committee for Practice Guidelines (CPG). European Guidelines on cardiovascular disease prevention in clinical practice (version 2012). The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts) Eur Heart J. 2012;33:1635–1701. doi: 10.1093/eurheartj/ehs092. [DOI] [PubMed] [Google Scholar]
- 3.Lewington S, Whitlock G, Clarke R, Sherliker P, Emberson J, Halsey J, Qizilbash N, Peto R, Collins R. Blood cholesterol and vascular mortality by age, sex, and blood pressure: a meta-analysis of individual data from 61 prospective studies with 55,000 vascular deaths. Lancet. 2007;370:1829–1839. doi: 10.1016/S0140-6736(07)61778-4. [DOI] [PubMed] [Google Scholar]
- 4.Ezzati M, Lopez AD, Rodgers A, Vander Hoorn S, Murray CJ; Comparative Risk Assessment Collaborating Group. Selected major risk factors and global and regional burden of disease. Lancet. 2002;360:1347–1360. doi: 10.1016/S0140-6736(02)11403-6. [DOI] [PubMed] [Google Scholar]
- 5.World Health Organization. The World Health Report 2002 - Reducing Risks, Promoting Healthy Life. Geneva: WHO; 2002. [DOI] [PubMed] [Google Scholar]
- 6.Eliasson M, Janlert U, Jansson JH, Stegmayr B. Time trends in population cholesterol levels 1986-2004: influence of lipid-lowering drugs, obesity, smoking and educational level. The northern Sweden MONICA study. J Intern Med. 2006;260:551–559. doi: 10.1111/j.1365-2796.2006.01730.x. [DOI] [PubMed] [Google Scholar]
- 7.Carroll MD, Lacher DA, Sorlie PD, Cleeman JI, Gordon DJ, Wolz M, Grundy SM, Johnson CL. Trends in serum lipids and lipoproteins of adults, 1960-2002. JAMA. 2005;294:1773–1781. doi: 10.1001/jama.294.14.1773. [DOI] [PubMed] [Google Scholar]
- 8.Evans A, Tolonen H, Hense HW, Ferrario M, Sans S, Kuulasmaa K. Trends in coronary risk factors in the WHO MONICA project. Int J Epidemiol. 2001;30 Suppl 1:S35–S40. doi: 10.1093/ije/30.suppl_1.s35. [DOI] [PubMed] [Google Scholar]
- 9.Capuano V, Lamaida N, De Martino M, Punzi M, De Vita S, Riccio MD. The Montecorvino Rovella Project: prevalence of coronary disease risk factors in an area of Campania. G Ital Cardiol. 1994;24:399–408. [PubMed] [Google Scholar]
- 10.Capuano V, D’Arminio T, Bambacaro A, Lanzara C, D’Antonio V. The VIP Project: prevalence of risk factors for ischemic cardiopathy in an area of Campania. Ital Heart J Suppl. 2001;2:1201–1208. [PubMed] [Google Scholar]
- 11.Capuano V, D’Arminio T, La Sala G, Mazzotta G. The third component of the complement (C3) is a marker of the risk of atherogenesis. Eur J Cardiovasc Prev Rehabil. 2006;13:658–660. doi: 10.1097/01.hjr.0000224485.80349.76. [DOI] [PubMed] [Google Scholar]
- 12.World Health Organization. CINDI Programme-Protocol and Guidelines. Copenhagen: WHO Regional Office for Europe; 1996. [Google Scholar]
- 13.Tenconi MT, Gianti A, Carreri V, Capuano V, Dormi A, Giampaoli S, Muntoni S, Vanuzzo D. Il programma CINDI dell’OMS e la partecipazione italiana. Ig Sanita Pubbl. 2000;56:505–516. [Google Scholar]
- 14.Farzadfar F, Finucane MM, Danaei G, Pelizzari PM, Cowan MJ, Paciorek CJ, Singh GM, Lin JK, Stevens GA, Riley LM, et al. National, regional, and global trends in serum total cholesterol since 1980: systematic analysis of health examination surveys and epidemiological studies with 321 country-years and 3·0 million participants. Lancet. 2011;377:578–586. doi: 10.1016/S0140-6736(10)62038-7. [DOI] [PubMed] [Google Scholar]
- 15.Menotti A, Giampaoli S, Verdecchia A, Cesana GC, Feruglio GA, Righetti G, Ferrario M, Vanuzzo . DIl Progetto MONICA (monitoraggio malattie cardiovascolari): Protocollo e manuale delle aree italiane. Italia: Istituto superiore di sanità; 1989. [Google Scholar]
- 16.Capuano V, Bambacaro A, D’Arminio T, Del Regno B, Dantonio V, Lanzara C. Changes in total serum cholesterol for cardiovascular disease in a Mediterranean area, 1989-1999. Eur J Epidemiol. 2003;18:27–32. doi: 10.1023/a:1022533117139. [DOI] [PubMed] [Google Scholar]
- 17.Keys A. From Naples to seven countries--a sentimental journey. Prog Biochem Pharmacol. 1983;19:1–30. [PubMed] [Google Scholar]
- 18.Mancini M, Rubba P. The Mediterranean diet in Italy. World Rev Nutr Diet. 2000;87:114–126. doi: 10.1159/000059724. [DOI] [PubMed] [Google Scholar]
- 19.Kuklina EV, Yoon PW, Keenan NL. Trends in high levels of low-density lipoprotein cholesterol in the United States, 1999-2006. JAMA. 2009;302:2104–2110. doi: 10.1001/jama.2009.1672. [DOI] [PubMed] [Google Scholar]
- 20.Sjøl A, Grunnet K, Schroll M. Secular trends in serum cholesterol, high density lipoproteins and triglycerides 1964-1987. Int J Epidemiol. 1991;20:105–113. doi: 10.1093/ije/20.1.105. [DOI] [PubMed] [Google Scholar]
- 21.Krumholz HM, Douglas PS, Lauer MS, Pasternak RC. Selection of patients for coronary angiography and coronary revascularization early after myocardial infarction: is there evidence for a gender bias. Ann Intern Med. 1992;116:785–790. doi: 10.7326/0003-4819-116-10-785. [DOI] [PubMed] [Google Scholar]
- 22.Tofler GH, Stone PH, Muller JE, Willich SN, Davis VG, Poole WK, Strauss HW, Willerson JT, Jaffe AS, Robertson T. Effects of gender and race on prognosis after myocardial infarction: adverse prognosis for women, particularly black women. J Am Coll Cardiol. 1987;9:473–482. doi: 10.1016/s0735-1097(87)80038-4. [DOI] [PubMed] [Google Scholar]
- 23.Baigent C, Blackwell L, Emberson J, Holland LE, Reith C, Bhala N, Peto R, Barnes EH, Keech A, Simes J, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376:1670–1681. doi: 10.1016/S0140-6736(10)61350-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Brugts JJ, Yetgin T, Hoeks SE, Gotto AM, Shepherd J, Westendorp RG, de Craen AJ, Knopp RH, Nakamura H, Ridker P, et al. The benefits of statins in people without established cardiovascular disease but with cardiovascular risk factors: meta-analysis of randomised controlled trials. BMJ. 2009;338:b2376. doi: 10.1136/bmj.b2376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Reiner Z, Catapano AL, De Backer G, Graham I, Taskinen MR, Wiklund O, Agewall S, Alegria E, Chapman MJ, Durrington P, et al. ESC/EAS Guidelines for the management of dyslipidaemias: the Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS) Eur Heart J. 2011;32:1769–1818. doi: 10.1093/eurheartj/ehr158. [DOI] [PubMed] [Google Scholar]