

Abstract
Background
We retrospectively assessed the clinical outcomes and investigated risk factors influencing retear after arthroscopic suture bridge repair technique for rotator cuff tear through clinical assessment and magnetic resonance arthrography (MRA).
Methods
Between January 2008 and April 2011, sixty-two cases of full-thickness rotator cuff tear were treated with arthroscopic suture bridge repair technique and follow-up MRA were performed. The mean age was 56.1 years, and mean follow-up period was 27.4 months. Clinical and functional outcomes were assessed using range of motion, Korean shoulder score, Constant score, and UCLA score. Radiological outcome was evaluated with preoperative and follow-up MRA. Potential predictive factors that influenced cuff retear, such as age, gender, geometric patterns of tear, size of cuff tear, acromioplasty, fatty degeneration, atrophy of cuff muscle, retraction of supraspinatus, involved muscles of cuff and osteolysis around the suture anchor were evaluated.
Results
Thirty cases (48.4%) revealed retear on MRA. In univariable analysis, retear was significantly more frequent in over 60 years age group (62.5%) than under 60 years age group (39.5%; p = 0.043), and also in medium to large-sized tear than small-sized tear (p = 0.003). There was significant difference in geometric pattern of tear (p = 0.015). In multivariable analysis, only age (p = 0.036) and size of tear (p = 0.030) revealed a significant difference. The mean active range of motion for forward flexion, abduction, external rotation at the side and internal rotation at the side were significantly improved at follow-up (p < 0.05). The mean Korean shoulder score, Constant score, and UCLA score increased significantly at follow-up (p < 0.01). The range of motion, Korean shoulder score, Constant score, and UCLA score did not differ significantly between the groups with retear and intact repairs (p > 0.05). The locations of retear were insertion site in 10 cases (33.3%) and musculotendinous junction in 20 cases (66.7%; p = 0.006).
Conclusions
Suture bridge repair technique for rotator cuff tear showed improved clinical results. Cuff integrity after repair did not affect clinical results. Age of over 60 years and size of cuff tear larger than 1 cm were factors influencing rotator cuff retear after arthroscopic suture bridge repair technique.
Keywords: Rotator cuff tear, Suture bridge technique, Retear, Magnetic resonance arthrography
Arthroscopic rotator cuff repair is a currently popular treatment. While open repair has been a common surgical method for the treatment of rotator cuff tears, arthroscopic repair has recently been accepted widely, reporting equal or better results than the open repairs.1,2) Surgical rotator cuff repair is aimed at obtaining biological healing through the minimization of bone-tendon gap formation by high initial fixation strength and maintenance of mechanical stability against repetitive loads. For these purposes, various arthroscopic techniques have been introduced including the single-row, double-row suture and suture bridge repair technique. Double-row technique has a higher load to failure and a lower frequency of gap formation than single-row technique.3,4) Tear rates were found to be significantly lower in double-row than in single-row technique.5,6) Suture bridge technique led to improved pressurized contact area and mean pressure between tendon and foot print compared with double-row techniques in the laboratory.7) Several studies of suture bridge repair technique have been reported.8-10) Voigt et al.8) reported that suture bridge technique resulted in comparable patient satisfaction, functional outcome and rate of retear. Cho et al.9) reported suture bridge technique tended to better in preserving the cuff tissue repaired to the insertion site of the rotator cuff than the single-row technique. Although there are some limitations in these studies including retrospective analysis, short-term follow-up and lack of diverse cases, suture bridge technique continues to receive attention. Therefore, the purpose of this study is to assess the clinical outcomes of arthroscopic suture bridge technique and factors influencing rotator cuff retear through clinical and radiological follow-up with magnetic resonance arthrography (MRA).
METHODS
Between January 2008 and April 2011, there were 196 cases treated with arthroscopic suture bridge technique for rotator cuff tear. Follow-up MRA was performed for sixty-two cases. The mean age was 56.1 years (range, 29 to 73 years), and mean follow-up period was 27.4 months (range, 6 to 52 months). There were 26 males and 36 females.
Preoperative and Postoperative Evaluations
Examinations were made a day before operation and during the follow-up period. All the operative results were analyzed at the last follow-up. Active shoulder motions including forward flexion, external rotation at the side and internal rotation with the arm at 90° abduction were measured in the seated position. Functional outcome was assessed using Korean shoulder score (KSS), Constant score, and the shoulder rating scale of the University of California at Los Angeles (UCLA).
Radiological outcome was evaluated with preoperative and follow-up MRA. MRA was performed using a 1.5-Tesla scanner (Magnetom Vision, Siemens, Germany). All 62 patients underwent MRA at average 6 months postoperatively. According to Sugaya et al.11) classification, postoperative cuff integrity was classified into five categories using oblique, coronal, oblique sagittal and transverse views of T2-weighted images: type I, repaired cuff appeared to have sufficient thickness compared with normal cuff with homogeneously low intensity on each image; type II, sufficient thickness compared with normal cuff associated with partial high intensity area; type III, insufficient thickness with less than half the thickness when compared with normal cuff, but without discontinuity, suggesting a partial-thickness delaminated tear; type IV, presence of a minor discontinuity in only 1 or 2 slices on both oblique coronal and sagittal images, suggesting a small full-thickness tear; and type V, presence of a major discontinuity observed in more than 2 slices on both oblique coronal and sagittal images, suggesting a medium or large full-thickness tear. We defined a retear as type IV and type V.
The size of cuff tear was defined as the length of the greatest diameter measured with probes during surgery. The tear sizes were categorized into small (< 1 cm), medium (1 to 3 cm), large (3 to 5 cm), and massive (> 5 cm), according to the classification of DeOrio and Cofield.12)
Geometric patterns of cuff tear were classified by coronal length and sagittal width and assessed considering arthroscopic and MRA findings. The patterns were categorized into crescent tear, longitudinal tear, and massive contracted tear according to the classification of Davidson and Burkhart:13) crescent tear, coronal length that is less than or equal to sagittal width and length less than 2 cm; longitudinal tear, length greater than width and width less than 2 cm; and massive contracted tear, maximum length greater than or equal to 2 cm and maximum width greater than or equal to 2 cm.
According to the classification of Patte,14) the retraction of supraspinatus tendon was classified into three categories by the location of the medial edge of the tear: grade 1, the tendon edge was lying between greater tuberosity and apex of the humeral head; grade 2, the tendon edge was lying between apex of the humeral head and glenoid of the scapula; and grade 3, tears that were retracted medial to the glenoid. The retraction was measured by intraoperative finding.
Measurement of muscle atrophy is based on oblique sagittal plane image medial to coracoid process, according to the classification of Warner et al.15) (Fig. 1). A line is drawn from the edge of the coracoid to the inferior scapular tip, from the inferior tip of the scapula to the spine and from the scapular spine to the coracoid process. If the muscle is convex above the line, there is no atrophy. If the muscle contour is even with the line, mild atrophy exists. If the contour of the muscle is concave below the line, moderate atrophy is present. If there is barely any muscle visible, severe atrophy exists.
Fig. 1.

Measurement of muscle atrophy by Warner et al. is based on oblique sagittal plane image medial to coracoid process. A line is drawn from the edge of the coracoid to the inferior scapular tip, from the inferior tip of the scapula to the spine, and from the scapular spine to the coracoid process. If the muscle is convex above the line, there is no atrophy line, moderate atrophy is present. If there is barely any muscle visible, severe atrophy exists. Reprint from Warner et al.15) with permission from Elsevier.
The presence of fatty degeneration was evaluated for supraspinatus, infraspinatus and subscapularis muscle using the five-stage grading system with preoperative MRI16) developed by Goutallier et al.17) We evaluated fatty degeneration, not only in each cuff muscle individually but of all cuff muscles combined, by calculating the global fatty degeneration index (GFDI) as the mean value of the grades for the supraspinatus, infraspinatus and subscapularis.17) Evaluation of fatty degeneration was performed on the level showing the coracoid base, where the scapular forms a Y-shape, using T1-weighted oblique sagittal and coronal MRI.
To evaluate osteolysis around the suture anchor, patients underwent simple radiographs immediately after surgery and six months after the surgery. By comparing the two radiographs, patients were classified into a group with osteolysis and group without osteolysis.
All classifications using MRA were performed by two orthopedic surgeons. Interobserver reliability was evaluated with the intraclass correlation coefficient (ICC). ICC was interpreted as follows: 0-0.4 indicates poor agreement; 0.4-0.75 indicates fair to good agreement; and > 0.75 indicates excellent agreement.
Surgical Technique
All operations were performed by the senior author (KWL), with the patient under general anesthesia in a beach-chair position. All patients with rotator cuff tear were treated with arthroscopic suture bridge repair technique.
A posterior portal is established for the initial assessment of the glenohumeral joint. If there is subscapularis tendon tear, a suture for the subscapularis is performed first. Arthroscopy is moved to the subacromial space to assess the superoposterior cuff. Bursectomy and subacromial decompression are performed if needed. Then the torn cuff is debrided in order to confirm the margin and evaluate the mobility of the tendon. The tendon is released until the cuff is adequately mobilized. The tendon is then repaired to the prepared greater tuberosity with suture anchors. Suture bridge repair is then carried out by fixating one limb from each anchor to the lateral aspect of the greater tuberosity, using knotless suture anchors.
Rehabilitation
Identical rehabilitation protocol was applied to all patients. Pendulum exercises and active elbow range of motion (ROM) exercise were started immediately after surgery, and passive forward flexion was started at 3 days after surgery. Early ROM was permitted in a tolerable range. Immobilization was maintained with an abduction brace for 6 weeks, and then active joint exercise and muscle strength exercise were started. A return to recreational activity or manual labor was permitted six months after the operation.
Statistical Analysis
To compare preoperative and postoperative range of motion and shoulder scores, the paired t-test or Wilcoxon signed rank test was used. For the univariable analysis, Pearson chi-square test or likelihood ratio test was used to analyze the factors influencing the rotator cuff retear, such as age, gender, geometric patterns of tear, size of cuff tear, acromioplasty, fatty degeneration, atrophy of cuff muscle, retraction of supraspinatus, involved muscles of cuff and osteolysis around the suture anchor. Finally, multivariable analysis was performed with the significant factors of univariable analysis, using logistic regression with a backward elimination stepwise procedure. SPSS ver. 16.0 (SPSS Inc., Chicago, IL, USA) was used for all statistical analyses, with α level set at 0.05.
RESULTS
At the follow-up MRA, retear was observed in 30 of 62 cases (48.4%). The incidence of rotator cuff retear significantly increases in the group over 60 years old (62.5%) than below 60 years (39.5%; p = 0.043). However, there was no association between gender and retear (p > 0.05) (Table 1). Retear was observed in 13 of 26 males (50%) and 17 of 36 females (47.2%).
Table 1.
Results of Univariable Analysis for Potential Predictive Factors Influencing Retear
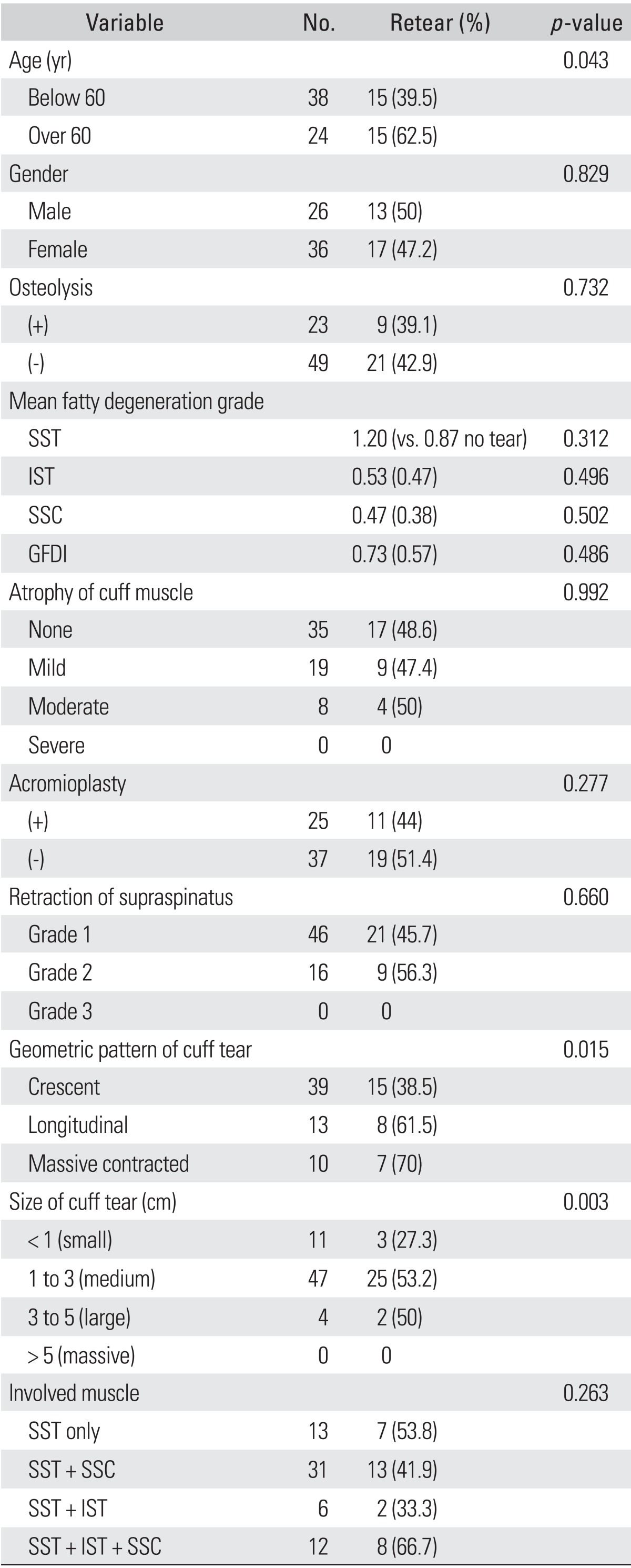
SST: supraspinatus, IST: infraspinatus, SSC: subscapularis, GFDI: global fatty degeneration index.
In the classifications of DeOrio and Cofield,12) retear was observed in 3 of 11 small-sized tears (27.3%), 25 of 47 medium-sized tears (53.2%), and 2 of 4 large-sized tear (50%). There was no massive tear. There was significant difference between small-sized tear (< 1 cm) and medium to large-sized tear (> 1 cm; p = 0.003) (Table 1).
In the classification of Davidson and Burkhart,13) retear was observed in 15 of 39 crescent tears (38.5%), 8 of 13 longitudinal tears (61.5%), and 7 of 10 massive contracted tears (70%). There was statistically significant difference between the geometric patterns of tear and incidence of retear (p = 0.015) (Table 1).
In the classification of Patte,14) retear was observed in 21 of 46 grade 1 retraction (45.7%) and 9 of 16 grade 2 retraction (56.3%). There was no grade 3 retraction. There was no statistically significant difference between the retraction of supraspinatus tendon and incidence of retear (p > 0.05) (Table 1).
According to the classification of Warner et al.,15) retear was observed in 17 of 35 cases (48.6%) in no atrophy group, 9 of 19 cases (47.4%) in mild atrophy group, and 4 of 8 cases (50%) in moderate atrophy group. There was no severe atrophy. There was no statistically significant difference between atrophy of cuff and incidence of retear (p > 0.05) (Table 1).
According to the classification of Goutallier et al.,17) mean fatty degeneration grades for the supraspinatus were 1.20 in cuff with retear and 0.87 in intact cuff. Corresponding values were 0.53 and 0.47 for the infraspinatus and 0.47 and 0.38 for the subscapularis grades. GFDI was 0.73 in cuff with retear and 0.57 in intact cuff. There was no significant association between retear and fatty degeneration of each muscle, as well as between retear and GFDI (p > 0.05) (Table 1).
In order to assess the effect of acromioplasty affecting retear, we compared the results of group that underwent acromioplasty with the group which did not. Retear was found in 11 of 25 shoulders (44.0%) that underwent acromioplasty and in 19 of 37 shoulders (51.4%) which did not. There was no statistically significant difference (p > 0.05) (Table 1).
Retear was found in 7 of 13 (53.8%) isolated supraspinatus tendon tear, in 13 of 31 tears (41.9%) involving supraspinatus and subscapularis tendon, in 2 of 6 tears (33.3%) involving supraspinatus and infraspinatus tendon and in 8 of 12 tears (66.7%) involving supraspinatus, subscapularis and infraspinatus tendon. These findings did not reach statistically significant difference between the number or kinds of involved tendon and incidence of retear (p > 0.05) (Table 1).
Retear was found in 9 of 23 shoulders (39.1%) that showed osteolytic lesion around the suture anchor and in 21 of 49 shoulders (42.9%) that did not. There was no statistically significant difference (p > 0.05) (Table 1).
In multivariable analysis with age, size and geometric pattern of rotator cuff tear, which analyzed the significant factors in univariable analysis, only age (p = 0.036) and size (p = 0.030) showed significant correlation with retear. The locations where retears occurred were the insertion site in 10 cases (32.2%) and musculotendinous junction in 20 cases (66.7%). There was statistically significant difference (p = 0.006).
A separate, independent study evaluating interobserver reliability was performed to determine the validity of our readings with ICC. We found that ICC was over 0.79 in all categories except fatty degeneration, representing an excellent agreement between observers. ICC on fatty degeneration was 0.64, representing a fair to good agreement.
Clinical Assessments
The mean preoperative range in active motion was 145.0° (range, 30° to 180°) in forward flexion, 127.2° (range, 30° to 175°) in abduction, 61.0° (range, 10° to 80°) of external rotation, and 45.1° (range, 30° to 80°) in internal rotation. At the last follow-up, the mean range of motion improved to 160.2° (range, 50° to 180°) in forward flexion, 146.5° (range, 50° to 175°) in abduction, 71.5° (range, 15° to 90°) in external rotation and 56.4° (range, 10° to 90°) in internal rotation. The postoperative improvement in all directional shoulder ROM was statistically significant (p < 0.05). The mean KSS score improved from 67.9 points (range, 42 to 96 points) preoperatively to 78.3 points (range, 51 to 93 points) at the last follow-up (p < 0.01). The mean UCLA score increased from 18.8 points (range, 6 to 29 points) preoperatively to 27.8 points (range, 15 to 35 points) at the last follow-up visit (p < 0.01). The mean Constant score rose from 63.6 (range, 10 to 90) preoperatively to 74.9 (range, 20 to 100) at the last follow-up (p < 0.01). The range of motion, KSS, Constant score, and UCLA score had no significant difference between the group with retear and group with intact cuff (p > 0.05).
DISCUSSION
Suture bridge technique has received recent attention, with several studies reporting good results from the technique.8,9) Anatomical failure rate of the single-row technique is reported at 22% to 25%.18,19) Studies on structural healing after double-row rotator cuff repair reported 11% to 17% of retear.20,21) Frank et al.22) first reported anatomical results of suture bridge technique with a retear rate of 12%, which is better than other arthroscopic repair techniques. However, there are some limitations due to the small sample size and with relatively small-sized tears mainly having been included. A recent clinical study of the suture bridge technique reported 28.1% to 33.3% of retear.8,10) However, retear rate after suture bridge technique showed 48.4% in the present study, which is higher than results of previous studies.8,10,22) It is possible that retear rate was measured higher, as patients with symptoms tended to agree with the MRA examination.
There has been a controversy of age being a predictive factor of cuff integrity. Boileau et al.23) reported that age was a factor influencing tendon-healing, and that the chance of tendon healing decreased to 43% when patients were over sixty-five years old. They suggested that an absence of tendon-to-bone healing after cuff repair may be secondary to mechanical factors and also presented potential biological factors (osteoporotic bone, weak degenerative tendons and decreased healing potential with increasing age). Voigt et al.8) reported that a patient age of over 60 years was found to influence tendon-healing significantly. However, Oh et al.24) advocated that age was not an independent determinant of anatomical outcome, but a confounding variable. In this study, age of more than 60 years was the independent determinant on the multivariable analysis as well as the univariable analysis. The results supported that patient's age at the time of operation affected the cuff integrity after rotator cuff repair.
Trantalis et al.25) first reported that retear occurred at the medial portion of the tendon after arthroscopic double row repair. This was another pattern of retear from those previously reported, which occurred at the footprint of the tendon. The causes of medial cuff failure were suggested to be tension overload of the suture-tendon interface, over-tensioning of the medial repair due to oblique path of suture passage, a relatively larger hole created by retrograde suture-passing instruments and the effect of the braided suture materials. Cho et al.9) reported that retear in cases using the suture bridge repair technique was observed at 74.1% at the musculotendinous junction and 25.9% at the insertion site, while in cases with a single-row repair was observed at 26.3% at the musculotendinous junction and 73.7% at the insertion site. Voigt et al.8) reported two different types of retears, which were the insufficiently healed and medially retorn supraspinatus tendons. The insufficiently healed tendon was at 54%, and medially retorn tendon was 46%. In the present study, retear occurred in 10 cases (33.3%) at the insertion site and 20 cases (66.7%) at the musculotendinous junction. Retear occurred more frequently at the musculotendinous junction with significance (p < 0.05). It is supposed that suture bridge repair technique facilitates the bone-tendon healing through the increased pressurized contact area over the previous suture techniques, but there may also arise a strangulation or disturbance of microcirculation due to tension overload at the medial row. Therefore, as suggested by Cho et al.,10) surgeons should try to choose an adequate placement of sutures at regular intervals and pay attention to the amount of tension used to tie them.
In previous studies,26,27) despite retears after rotator cuff repair, the technique was reported to represent satisfactory results for clinical and functional outcomes. Gerber et al.26) reported that although retear represented 34% in 3 years MRI follow-up after open rotator cuff repair, patients with retear had functional improvements. Galatz et al.27) reported that retear represented 94% in 1 to 2 years ultrasonography follow-up after arthroscopic rotator cuff repair, and that the patients with retear also had functional improvements. In the present study, the mean range of active motion after operation was improved in forward flexion, abduction, external rotation and internal rotation (p < 0.05). The mean KSS, UCLA score, and Constant score improved at the last follow-up (p < 0.01). However, the range of motion, KSS, Constant score, and UCLA score had no significant difference between group with retear and group with intact cuff (p > 0.05). In the present study, although there was 48.4% of retear rate after rotator cuff repair, the technique represented satisfactory clinical results as the previous studies.
In this study, MRA was performed at 6 months postoperatively for evaluation of cuff integrity after repair. The reason we had chosen the point was that we concluded it to give enough time to observe the structural state of rotator cuff. Recently, Miller et al.28) have reported retear of 41% with serial follow-up after arthroscopic repair. All retears occurred prior to 6 months, and no tears occurred between 6 and 24 months.
In the present study, the anatomical evaluation of the cuff repair was done with MRA as the investigation of choice for the assessment of cuff integrity. It has advantages over ultrasonography in terms of sensitivity and specificity.29) The follow-up using ultrasonography is easy to evaluate at the outpatient clinic and inexpensive. However, it has the disadvantages of less sensitivity, as postoperative shoulders show an abnormal echogenicity. As such, we did not use the results of ultrasonography due to the lower reliability than MRA. The postoperative changes of cuff are mimicked by the echogenic appearance of small rotator cuff tears. This is likely due to the nature of tendon healing. While there is a tendency for reorganization of the tendon fibers after repair, a significant disorganization and irregular collagen bundles persist.30) Abnormal echogenicity of the tendon would make the diagnosis of small new or recurrent tears impossible, although it is possible to diagnose cuff-thinning or large gap within the tendon.
There are some limitations in this study. First, this study is not a prospective randomized clinical trial. Second, there were no cases of severe category in some variables, such as severe atrophy, massive-sized tear and grade 3 retraction. It is due to other surgical techniques having been used in severe cases, such as mini-open repair with or without tendon augmentation, tendon transfer and reverse shoulder arthroplasty. Third, all patients who underwent rotator cuff repair did not all undergo an MRA. It is possible that the retear rate was measured higher, because patients who had the symptoms tended to agree with the MRA examination. As such, a precise retear rate might be unknown. Fourth, we did not evaluate exactly the cause of pain. Fifth, the outcome evaluation at a mean of 27.4 months was short. We suggest that studies involving a larger population and long-term follow-up be conducted in the future.
In conclusions, suture bridge repair technique for rotator cuff tear shows improved clinical results. Cuff integrity after repair did not affect clinical results. Age over 60 years old and size of cuff tear larger than 1 cm were factors influencing rotator cuff retear after suture bridge repair technique.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Bennett WF. Arthroscopic repair of full-thickness supraspinatus tears (small-to-medium): a prospective study with 2- to 4-year follow-up. Arthroscopy. 2003;19(3):249–256. doi: 10.1053/jars.2003.50083. [DOI] [PubMed] [Google Scholar]
- 2.Murray TF, Jr, Lajtai G, Mileski RM, Snyder SJ. Arthroscopic repair of medium to large full-thickness rotator cuff tears: outcome at 2- to 6-year follow-up. J Shoulder Elbow Surg. 2002;11(1):19–24. doi: 10.1067/mse.2002.120142. [DOI] [PubMed] [Google Scholar]
- 3.Ozbaydar M, Elhassan B, Esenyel C, et al. A comparison of single-versus double-row suture anchor techniques in a simulated repair of the rotator cuff: an experimental study in rabbits. J Bone Joint Surg Br. 2008;90(10):1386–1391. doi: 10.1302/0301-620X.90B10.20862. [DOI] [PubMed] [Google Scholar]
- 4.Baums MH, Buchhorn GH, Spahn G, Poppendieck B, Schultz W, Klinger HM. Biomechanical characteristics of single-row repair in comparison to double-row repair with consideration of the suture configuration and suture material. Knee Surg Sports Traumatol Arthrosc. 2008;16(11):1052–1060. doi: 10.1007/s00167-008-0590-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Franceschi F, Ruzzini L, Longo UG, et al. Equivalent clinical results of arthroscopic single-row and double-row suture anchor repair for rotator cuff tears: a randomized controlled trial. Am J Sports Med. 2007;35(8):1254–1260. doi: 10.1177/0363546507302218. [DOI] [PubMed] [Google Scholar]
- 6.Sugaya H, Maeda K, Matsuki K, Moriishi J. Functional and structural outcome after arthroscopic full-thickness rotator cuff repair: single-row versus dual-row fixation. Arthroscopy. 2005;21(11):1307–1316. doi: 10.1016/j.arthro.2005.08.011. [DOI] [PubMed] [Google Scholar]
- 7.Park MC, Tibone JE, ElAttrache NS, Ahmad CS, Jun BJ, Lee TQ. Part II: Biomechanical assessment for a footprint-restoring transosseous-equivalent rotator cuff repair technique compared with a double-row repair technique. J Shoulder Elbow Surg. 2007;16(4):469–476. doi: 10.1016/j.jse.2006.09.011. [DOI] [PubMed] [Google Scholar]
- 8.Voigt C, Bosse C, Vosshenrich R, Schulz AP, Lill H. Arthroscopic supraspinatus tendon repair with suture-bridging technique: functional outcome and magnetic resonance imaging. Am J Sports Med. 2010;38(5):983–991. doi: 10.1177/0363546509359063. [DOI] [PubMed] [Google Scholar]
- 9.Cho NS, Yi JW, Lee BG, Rhee YG. Retear patterns after arthroscopic rotator cuff repair: single-row versus suture bridge technique. Am J Sports Med. 2010;38(4):664–671. doi: 10.1177/0363546509350081. [DOI] [PubMed] [Google Scholar]
- 10.Cho NS, Lee BG, Rhee YG. Arthroscopic rotator cuff repair using a suture bridge technique: is the repair integrity actually maintained? Am J Sports Med. 2011;39(10):2108–2116. doi: 10.1177/0363546510397171. [DOI] [PubMed] [Google Scholar]
- 11.Sugaya H, Maeda K, Matsuki K, Moriishi J. Repair integrity and functional outcome after arthroscopic double-row rotator cuff repair: a prospective outcome study. J Bone Joint Surg Am. 2007;89(5):953–960. doi: 10.2106/JBJS.F.00512. [DOI] [PubMed] [Google Scholar]
- 12.DeOrio JK, Cofield RH. Results of a second attempt at surgical repair of a failed initial rotator-cuff repair. J Bone Joint Surg Am. 1984;66(4):563–567. [PubMed] [Google Scholar]
- 13.Davidson J, Burkhart SS. The geometric classification of rotator cuff tears: a system linking tear pattern to treatment and prognosis. Arthroscopy. 2010;26(3):417–424. doi: 10.1016/j.arthro.2009.07.009. [DOI] [PubMed] [Google Scholar]
- 14.Patte D. Classification of rotator cuff lesions. Clin Orthop Relat Res. 1990;(254):81–86. [PubMed] [Google Scholar]
- 15.Warner JJ, Higgins L, Parsons IM, 4th, Dowdy P. Diagnosis and treatment of anterosuperior rotator cuff tears. J Shoulder Elbow Surg. 2001;10(1):37–46. doi: 10.1067/mse.2001.112022. [DOI] [PubMed] [Google Scholar]
- 16.Fuchs B, Weishaupt D, Zanetti M, Hodler J, Gerber C. Fatty degeneration of the muscles of the rotator cuff: assessment by computed tomography versus magnetic resonance imaging. J Shoulder Elbow Surg. 1999;8(6):599–605. doi: 10.1016/s1058-2746(99)90097-6. [DOI] [PubMed] [Google Scholar]
- 17.Goutallier D, Postel JM, Gleyze P, Leguilloux P, Van Driessche S. Influence of cuff muscle fatty degeneration on anatomic and functional outcomes after simple suture of full-thickness tears. J Shoulder Elbow Surg. 2003;12(6):550–554. doi: 10.1016/s1058-2746(03)00211-8. [DOI] [PubMed] [Google Scholar]
- 18.Cho NS, Rhee YG. The factors affecting the clinical outcome and integrity of arthroscopically repaired rotator cuff tears of the shoulder. Clin Orthop Surg. 2009;1(2):96–104. doi: 10.4055/cios.2009.1.2.96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Cole BJ, ElAttrache NS, Anbari A. Arthroscopic rotator cuff repairs: an anatomic and biomechanical rationale for different suture-anchor repair configurations. Arthroscopy. 2007;23(6):662–669. doi: 10.1016/j.arthro.2007.02.018. [DOI] [PubMed] [Google Scholar]
- 20.Huijsmans PE, Pritchard MP, Berghs BM, van Rooyen KS, Wallace AL, de Beer JF. Arthroscopic rotator cuff repair with double-row fixation. J Bone Joint Surg Am. 2007;89(6):1248–1257. doi: 10.2106/JBJS.E.00743. [DOI] [PubMed] [Google Scholar]
- 21.Lafosse L, Brozska R, Toussaint B, Gobezie R. The outcome and structural integrity of arthroscopic rotator cuff repair with use of the double-row suture anchor technique. J Bone Joint Surg Am. 2007;89(7):1533–1541. doi: 10.2106/JBJS.F.00305. [DOI] [PubMed] [Google Scholar]
- 22.Frank JB, ElAttrache NS, Dines JS, Blackburn A, Crues J, Tibone JE. Repair site integrity after arthroscopic transosseous-equivalent suture-bridge rotator cuff repair. Am J Sports Med. 2008;36(8):1496–1503. doi: 10.1177/0363546507313574. [DOI] [PubMed] [Google Scholar]
- 23.Boileau P, Brassart N, Watkinson DJ, Carles M, Hatzidakis AM, Krishnan SG. Arthroscopic repair of full-thickness tears of the supraspinatus: does the tendon really heal? J Bone Joint Surg Am. 2005;87(6):1229–1240. doi: 10.2106/JBJS.D.02035. [DOI] [PubMed] [Google Scholar]
- 24.Oh JH, Kim SH, Kang JY, Oh CH, Gong HS. Effect of age on functional and structural outcome after rotator cuff repair. Am J Sports Med. 2010;38(4):672–678. doi: 10.1177/0363546509352460. [DOI] [PubMed] [Google Scholar]
- 25.Trantalis JN, Boorman RS, Pletsch K, Lo IK. Medial rotator cuff failure after arthroscopic double-row rotator cuff repair. Arthroscopy. 2008;24(6):727–731. doi: 10.1016/j.arthro.2008.03.009. [DOI] [PubMed] [Google Scholar]
- 26.Gerber C, Fuchs B, Hodler J. The results of repair of massive tears of the rotator cuff. J Bone Joint Surg Am. 2000;82(4):505–515. doi: 10.2106/00004623-200004000-00006. [DOI] [PubMed] [Google Scholar]
- 27.Galatz LM, Ball CM, Teefey SA, Middleton WD, Yamaguchi K. The outcome and repair integrity of completely arthroscopically repaired large and massive rotator cuff tears. J Bone Joint Surg Am. 2004;86(2):219–224. doi: 10.2106/00004623-200402000-00002. [DOI] [PubMed] [Google Scholar]
- 28.Miller BS, Downie BK, Kohen RB, et al. When do rotator cuff repairs fail? Serial ultrasound examination after arthroscopic repair of large and massive rotator cuff tears. Am J Sports Med. 2011;39(10):2064–2070. doi: 10.1177/0363546511413372. [DOI] [PubMed] [Google Scholar]
- 29.Magee TH, Gaenslen ES, Seitz R, Hinson GA, Wetzel LH. MR imaging of the shoulder after surgery. AJR Am J Roentgenol. 1997;168(4):925–928. doi: 10.2214/ajr.168.4.9124141. [DOI] [PubMed] [Google Scholar]
- 30.Steiner M. Biomechanics of tendon healing. J Biomech. 1982;15(12):951–958. doi: 10.1016/0021-9290(82)90013-6. [DOI] [PubMed] [Google Scholar]