

Abstract
There is little consensus on how to optimally reconstruct the posterior cruciate ligament (PCL) and the natural history of injured PCL is also unclear. The graft material (autograft vs. allograft), the type of tibial fixation (tibial inlay vs. transtibial tunnel), the femoral tunnel position within the femoral footprint (isometric, central, or eccentric), and the number of bundles in the reconstruction (1 bundle vs. 2 bundles) are among the many decisions that a surgeon must make in a PCL reconstruction. In addition, there is a paucity of information on rehabilitation after reconstruction of the PCL and posterolateral structures. This article focused on the conflicting issues regarding the PCL, and the scientific rationales behind some critical points are discussed.
Keywords: Knee, Posterior cruciate ligament, Biomechanics, Outcome, Rehabilitation
Despite advances in knowledge of the basic science of the posterior cruciate ligament (PCL), there are still some controversies and challenging areas in orthopedic practice. First, results of biomechanical studies are conflicting, and it is not clear whether double-bundle reconstruction provides superior biomechanical and clinical outcomes, compared with single-bundle reconstruction.1-8) The natural history of PCL deficiency is also unclear, and the operative indications for these injuries remain controversial.9-13) In addition, there is a paucity of information on rehabilitation after reconstruction of the PCL and posterolateral structures.14) This article focused on the conflicting issues regarding the PCL, and the scientific rationales behind some critical points are discussed.
BIOMECHANICS BASED ON ANATOMY
Understanding the biomechanics of the native PCL provides a framework for reconstruction by replicating the anatomy.15) Early biomechanical studies characterized the Rehabilitationindividual main bundles of the PCL as anterolateral (AL) and posteromedial (PM) bundles.16,17) The AL bundle is more taut in flexion and more lax in extension; the reverse is true for the PM bundle, which is more taut in extension and more lax in flexion.17,18) In this setting, the AL and PM bundles mainly function individually at the flexed and extended positions, respectively.
However, more recent biomechanical studies have suggested that, based on length and spatial orientation, the two bundles of the PCL may have a co-dominant relationship rather than a reciprocal one.15,19-21) This concept means that both bundles function through the range of motion (ROM) in a synergistic fashion rather than a reciprocal one. Mauro et al.19) reported no difference in the in situ forces between the AL and PM bundles at any of the flexion angles, using a robotic testing system. Ahmad et al.21) reported that the PM bundle becomes more horizontal with increasing knee flexion and this orientation increased the ability of the PM bundle to resist posterior tibial translation. Using magnetic resonance imaging (MRI) and a dual-orthogonal fluoroscopic system, Papannagari et al.20) reported that both bundles showed elongation and change of orientation of up to 120° of knee flexion.
The number of bundles has been a hot issue in PCL biomechanics. Race and Amis22) conducted the first biomechanical comparison between isometric single and double bundle reconstruction; their results showed over-constraint of the isometric single bundle reconstruction in extension with underconstraint at higher degrees of flexion. The double bundle reconstruction resulted in restoration of the posterior laxity from 0° to 120° to within 1 mm of the intact specimens. Harner et al.8) also reported that double bundle reconstruction resulted in better restoration of posterior stability, compared with single bundle reconstruction in cadaveric knees. However, in some studies,4-6,23,24) in terms of posterior stability, few differences were observed between single and double bundle PCL reconstruction, even though some different results were reported with different experimental settings.
The influence of the femoral attachment site, as well as the number of bundles, was further evaluated.1,2,7) In a study using variable femoral attachment sites, Mannor et al.7) reported that a shallow femoral insertion allows for better control of posterior translation. However, they could not prove the possibility of graft elongation resulting from high graft tension. Shearn et al.1) reported that the placement of a second bundle in the middle or distal position resulted in a significant reduction in AL bundle tension and in cooperative load-sharing (with the bundles functioning together). However, placement of the second bundle in a proximal position resulted in reciprocal loading (with one bundle functioning in flexion and one in extension).
OUTCOMES
The majority of studies have reported improved outcomes from preoperative level of function; however, when compared with the preinjury activity status, the results are less successful.15) The objective knee scores seem to lag behind those of subjective self-reported scoring after surgical reconstruction; one possible explanation is residual laxity, which has been demonstrated using many reconstructive techniques.15) Most studies have reported residual laxity ranging from 2 to 6 mm indicating that the surgical result will depend upon the surgical technique.25-33)
Few clinical studies comparing the outcomes between single and double bundle PCL reconstruction have been reported. Wang et al.34) reported no significant difference in the functional score or radiologic evaluation. Three studies (Houe and Jorgensen,35) Fanelli and Larson,36) and Kim et al.37)) also reported no difference in subjective and objective outcomes. Only one recent study, by Yoon et al.,38) reported better stability and International Knee Documentation Committee (IKDC) distribution; however, they also stated that it is unclear whether double bundle is definitely superior clinically and functionally because there was no difference in the subjective scores.
ISOLATED INJURY (CONSERVATIVE VS. OPERATIVE TREATMENT)
PCL injuries have potential for intrinsic healing; several MRI studies have reported that the PCL healed with continuity but also with residual laxity.39-41) In most PCL injuries, some portion of the PCL, or at least the meniscofemoral ligament, is preserved, therefore, in an acute or subacute stage, the PCL has a higher likelihood of spontaneous healing than the anterior cruciate ligament (ACL) does.25) Many MRI studies have reported that because the ligament is surrounded by a thick synovial sheath that is hardly torn completely and the meniscofemoral ligament remains attached to the lateral meniscus, an injured PCL can heal itself.39-42)
Treatment of the isolated PCL injury should depend on the injury status, which is determined by the amount of posterior laxity, the patient's age and level of activity. In young patients, we can perform cylinder cast immobilization in order to prevent posterior sagging if the instability is less than 8 mm side to the side difference (which means that there is a stepping between the medial tibial and femoral condyles at 90° of flexion of the knee joint) and there is some continuity remaining according to the MRI.9,43) However, during cast immobilization, in order to prevent posterior sagging of the proximal tibia, the cast should be changed if the patient feels that his knee, especially the proximal tibia, is moving anteriorly and posteriorly in the cylinder cast. Cylinder cast immobilization is usually maintained for six weeks and then the brace is used with the attachment of two springs with a tibial supporter in order to prevent posterior translation of the tibia for another six weeks.9) Another option for conservative treatment of the isolated PCL injury is an immediate rehabilitation and quadriceps strengthening exercise program, especially for elderly patients.
We recommend PCL reconstruction in patients with more than grade II PCL injury, even for isolated PCL injury in young patients.25) The remnant PCL fibers would be helpful for the improvement of vascularization, and therefore, will promote healing of the graft, and the mechanoreceptors will provide mechanical stability. The center of the femoral tunnel was chosen so that the distal edge of the graft was 2 mm apart from the articular cartilage margin, by placing the guide pin 5-6 mm proximal to the articular cartilage at the 11 or 11:30 o'clock position (left knee), depending upon the graft diameter. A tibial tunnel could be created by placement of a guide pin just distal to the center of the tibial insertion or just lateral and distal to the center area in the remnant PCL. The graft can then pass along the medial border of the remnant PCL towards the femoral tunnel, which was located anteromedial to the PCL (Fig. 1).25,26,44)
Fig. 1.
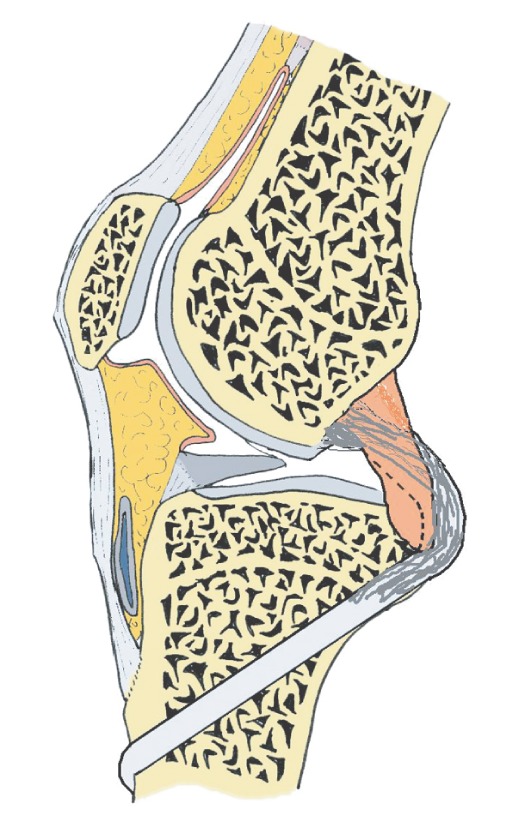
Schematic drawing: the remnant posterior cruciate ligament would work like a soft tissue cushion to prevent the killer turn effect at the tunnel orifice.
CHRONIC AND COMBINED INJURY
In the case of healed PCL with residual laxity, tensioning with an AL bundle reconstruction using a modified inlay technique could be used, and to get very good stability if the remnant PCL is thick and there is a normal signal in the MRI studies when the injury is chronic (more than 12 months). However, this technique is a technically demanding procedure and a bigger surgical scar may be produced.29,30,45,46) For AL bundle reconstruction for the single bundle reconstruction, the femoral tunnel should be made at a distal (shallow) and anterior portion. This means that the femoral tunnel should be placed distally (shallow), usually 5-6 mm, from the articular margin, and vertically. Remnant PCL fibers may provide a soft tissue cushion effect between the graft and the bone at the entrance to the tunnel, which is helpful to prevent the killer turn effect at the femoral and tibial tunnel orifice. If there is no remnant PCL or a very thin PCL remnant, we should do double bundle reconstruction (Fig. 2).47)
Fig. 2.
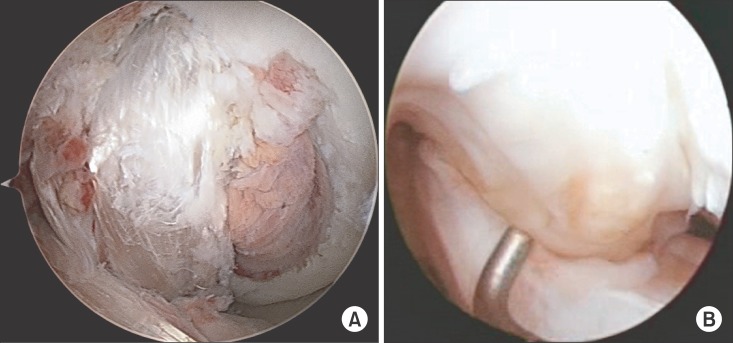
Remnant preserving posterior cruciate ligament (PCL) reconstruction. (A) The remnant PCL is preserved and the anterolateral bundle is reconstructed with autogenous hamstring 4 bundles. (B) Postoperative 2 years: the reconstructed PCL is well remodeled and it is difficult to differentiate between the graft and remnant PCL.
PCL injuries are frequently combined with posterolateral rotatory instability (PLRI), which occurs in about 43%-80% of cases.47,48) Although the causes of failure of PCL reconstruction are multifactorial, one of the most common causes is a neglected PLRI.49,50) Therefore, identification of concomitant injuries is important in order to obtain a good result. Currently, PLRI can only be evaluated through a physical examination. In particular, 1° to 2° PLRI (grade 1, external rotation [ER] using a dial test < 10° without varus instability; grade 2, ER ≥ 10° or posterolateral tibial subluxation with grade 0-2 varus instability; and grade 3, ER ≥ 20° or posterolateral tibial subluxation + grade 3 varus instability)48) often goes unnoticed, especially when the tests are performed with the muscle tensed in acute stage patients with pain. Therefore, PLRI assessment should be performed several times and should become a routine procedure before surgery for the patient under anesthesia.48,51)
Why is the PLRI misdiagnosed, especially in grade II PLRI? In our opinion, the reason is that in the PCL and posterolateral corner injured patient, the lateral tibial plateau is posterolatearally subluxed at 90° of knee flexion. If a dial test or posterolateral drawer test is performed in this situation, it is difficult to find more ER of the leg or subluxation of the posterolateral tibial plateau. Therefore, in PCL and posterolateral corner injured patients, reduction of the knee to the normal position using the dial test and posterolateral drawer test is important for making a diagnosis of PLRI.51) We determined that a reduction of the knee in the anteroposterior direction would increase the degree of tibial ER in combined PCL-posterolateral corner injuries.51) When we performed the dial test in the prone position, this position was also helpful for the same reason. In the prone position, posterior sagging of the proximal tibia would be reduced, which was better than the supine position.51,52) For treatment of PLRI, grade II injury could be managed with a posterolateral corner sling (PLCS) through the fibular head.48) However, in grade III PLRI, anatomical reconstruction would be preferable, as described by LaPrade and Wentorf.53)
REHABILITATION
In contrast to ACL rehabilitation, accelerated PCL postoperative rehabilitation is generally undesirable and more conservative methods are recommended than ACL reconstruction.54,55) However, the rehabilitation protocol of a PCL reconstruction is not well established and only a slow and conservative rehabilitation is proposed.14) For example, early weight bearing is believed to be hazardous to the PCL because PCL reconstruction is often associated with either a medial or lateral collateral ligament repair or reconstruction and it can cause over-stressing these structures.54,56)
Anatomically, the tibial plateau is inclined posteriorly and an axial load placed on the tibia by weight bearing at relatively extended positions produces an elemental force in the anterior direction. Therefore, the joint is stabilized somewhat by weight bearing.57,58) In addition, weight bearing can have several benefits. Firstly, the patient would have better static stability when standing on both legs, thereby minimizing the risk of falls. Secondly, it should stimulate tunnel healing and graft incorporation. Thirdly, it promotes the production of synovial fluid to bathe the articular cartilage. Fourthly, weight bearing itself can be a co-strengthening exercise and proprioceptive training.54,56,59) Finally, most patients have a tendency to flex their operated knee to prevent weight bearing.14) This means that a posteriorly directed force can be prevented if weight bearing is performed in the fully extended position.
Accelerated rehabilitation does not mean rapid range of motion exercise.14) Within 0° to 30° of flexion, the hamstring cannot produce a posterior shear force and the anterior angle of the patellar tendon is always larger than that of the hamstring tendons.60,61) Therefore, within this range of motion, co-strengthening could be performed using calf raising and mini-squatting exercise. Daniel et al.62) described the concept of the quadriceps neutral angle. The quadriceps neutral angle occurs at approximately 60° to 75° of flexion. Quadriceps strengthening extension exercise at angles less than the quadriceps neutral angle produces anterior tibial translation, which is antagonistic to the ACL but synergistic to the PCL. Therefore, after a PCL reconstruction, quadriceps strengthening knee extension should be restricted to between 60° of flexion and full extension of the knee.62,63)
CONCLUSIONS
In current PCL studies, there has been a shift in biomechanics from reciprocal functioning to co-dominance. Surgical devices and reconstructive techniques of the PCL have been developing and a more active approach is used than the past. It is still uncertain whether single or double bundle reconstruction is superior, because of conflicting biomechanical studies and notable limitations of the clinical studies. The remnants of PCL fibers, placement of the femoral tunnel, and combined PLRI are other hot issues in reconstruction. After the reconstruction of the PCL, a more active and systemic exercise program and early weight-bearing training are increasingly being recognized as important.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Shearn JT, Grood ES, Noyes FR, Levy MS. Two-bundle posterior cruciate ligament reconstruction: how bundle tension depends on femoral placement. J Bone Joint Surg Am. 2004;86(6):1262–1270. [PubMed] [Google Scholar]
- 2.Kohen RB, Sekiya JK. Single-bundle versus double-bundle posterior cruciate ligament reconstruction. Arthroscopy. 2009;25(12):1470–1477. doi: 10.1016/j.arthro.2008.11.006. [DOI] [PubMed] [Google Scholar]
- 3.Apsingi S, Nguyen T, Bull AM, Unwin A, Deehan DJ, Amis AA. Control of laxity in knees with combined posterior cruciate ligament and posterolateral corner deficiency: comparison of single-bundle versus double-bundle posterior cruciate ligament reconstruction combined with modified Larson posterolateral corner reconstruction. Am J Sports Med. 2008;36(3):487–494. doi: 10.1177/0363546508314415. [DOI] [PubMed] [Google Scholar]
- 4.Wiley WB, Askew MJ, Melby A, 3rd, Noe DA. Kinematics of the posterior cruciate ligament/posterolateral corner-injured knee after reconstruction by single- and double-bundle intra-articular grafts. Am J Sports Med. 2006;34(5):741–748. doi: 10.1177/0363546505282615. [DOI] [PubMed] [Google Scholar]
- 5.Markolf KL, Feeley BT, Jackson SR, McAllister DR. Biomechanical studies of double-bundle posterior cruciate ligament reconstructions. J Bone Joint Surg Am. 2006;88(8):1788–1794. doi: 10.2106/JBJS.E.00427. [DOI] [PubMed] [Google Scholar]
- 6.Bergfeld JA, Graham SM, Parker RD, Valdevit AD, Kambic HE. A biomechanical comparison of posterior cruciate ligament reconstructions using single- and double-bundle tibial inlay techniques. Am J Sports Med. 2005;33(7):976–981. doi: 10.1177/0363546504273046. [DOI] [PubMed] [Google Scholar]
- 7.Mannor DA, Shearn JT, Grood ES, Noyes FR, Levy MS. Two-bundle posterior cruciate ligament reconstruction: an in vitro analysis of graft placement and tension. Am J Sports Med. 2000;28(6):833–845. doi: 10.1177/03635465000280061101. [DOI] [PubMed] [Google Scholar]
- 8.Harner CD, Janaushek MA, Kanamori A, Yagi M, Vogrin TM, Woo SL. Biomechanical analysis of a double-bundle posterior cruciate ligament reconstruction. Am J Sports Med. 2000;28(2):144–151. doi: 10.1177/03635465000280020201. [DOI] [PubMed] [Google Scholar]
- 9.Jung YB, Tae SK, Lee YS, Jung HJ, Nam CH, Park SJ. Active non-operative treatment of acute isolated posterior cruciate ligament injury with cylinder cast immobilization. Knee Surg Sports Traumatol Arthrosc. 2008;16(8):729–733. doi: 10.1007/s00167-008-0531-0. [DOI] [PubMed] [Google Scholar]
- 10.Zaki SH, Rafiq I, Kapoor A, Raut V, Gambhir AK, Porter ML. Medium-term results with the press fit condylar (PFC) Sigma knee prosthesis the Wrightington experience. Acta Orthop Belg. 2007;73(1):55–59. [PubMed] [Google Scholar]
- 11.Boynton MD, Tietjens BR. Long-term followup of the untreated isolated posterior cruciate ligament-deficient knee. Am J Sports Med. 1996;24(3):306–310. doi: 10.1177/036354659602400310. [DOI] [PubMed] [Google Scholar]
- 12.Skyhar MJ, Warren RF, Ortiz GJ, Schwartz E, Otis JC. The effects of sectioning of the posterior cruciate ligament and the posterolateral complex on the articular contact pressures within the knee. J Bone Joint Surg Am. 1993;75(5):694–699. doi: 10.2106/00004623-199305000-00008. [DOI] [PubMed] [Google Scholar]
- 13.Keller PM, Shelbourne KD, McCarroll JR, Rettig AC. Nonoperatively treated isolated posterior cruciate ligament injuries. Am J Sports Med. 1993;21(1):132–136. doi: 10.1177/036354659302100122. [DOI] [PubMed] [Google Scholar]
- 14.Lee YS, Kim NK. Rehabilitation after posterior cruciate ligament reconstruction. Minerva Ortop Traumatol. 2011;62(4):291–295. [Google Scholar]
- 15.Voos JE, Mauro CS, Wente T, Warren RF, Wickiewicz TL. Posterior cruciate ligament: anatomy, biomechanics, and outcomes. Am J Sports Med. 2012;40(1):222–231. doi: 10.1177/0363546511416316. [DOI] [PubMed] [Google Scholar]
- 16.Harner CD, Baek GH, Vogrin TM, Carlin GJ, Kashiwaguchi S, Woo SL. Quantitative analysis of human cruciate ligament insertions. Arthroscopy. 1999;15(7):741–749. doi: 10.1016/s0749-8063(99)70006-x. [DOI] [PubMed] [Google Scholar]
- 17.Girgis FG, Marshall JL, Monajem A. The cruciate ligaments of the knee joint: anatomical, functional and experimental analysis. Clin Orthop Relat Res. 1975;(106):216–231. doi: 10.1097/00003086-197501000-00033. [DOI] [PubMed] [Google Scholar]
- 18.Van Dommelen BA, Fowler PJ. Anatomy of the posterior cruciate ligament: a review. Am J Sports Med. 1989;17(1):24–29. doi: 10.1177/036354658901700104. [DOI] [PubMed] [Google Scholar]
- 19.Mauro CS, Sekiya JK, Stabile KJ, Haemmerle MJ, Harner CD. Double-bundle PCL and posterolateral corner reconstruction components are codominant. Clin Orthop Relat Res. 2008;466(9):2247–2254. doi: 10.1007/s11999-008-0319-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Papannagari R, DeFrate LE, Nha KW, et al. Function of posterior cruciate ligament bundles during in vivo knee flexion. Am J Sports Med. 2007;35(9):1507–1512. doi: 10.1177/0363546507300061. [DOI] [PubMed] [Google Scholar]
- 21.Ahmad CS, Cohen ZA, Levine WN, Gardner TR, Ateshian GA, Mow VC. Codominance of the individual posterior cruciate ligament bundles: an analysis of bundle lengths and orientation. Am J Sports Med. 2003;31(2):221–225. doi: 10.1177/03635465030310021101. [DOI] [PubMed] [Google Scholar]
- 22.Race A, Amis AA. PCL reconstruction: in vitro biomechanical comparison of 'isometric' versus single and double-bundled 'anatomic' grafts. J Bone Joint Surg Br. 1998;80(1):173–179. doi: 10.1302/0301-620x.80b1.7453. [DOI] [PubMed] [Google Scholar]
- 23.Apsingi S, Nguyen T, Bull AM, Unwin A, Deehan DJ, Amis AA. The role of PCL reconstruction in knees with combined PCL and posterolateral corner deficiency. Knee Surg Sports Traumatol Arthrosc. 2008;16(2):104–111. doi: 10.1007/s00167-007-0444-3. [DOI] [PubMed] [Google Scholar]
- 24.Whiddon DR, Zehms CT, Miller MD, Quinby JS, Montgomery SL, Sekiya JK. Double compared with single-bundle open inlay posterior cruciate ligament reconstruction in a cadaver model. J Bone Joint Surg Am. 2008;90(9):1820–1829. doi: 10.2106/JBJS.G.01366. [DOI] [PubMed] [Google Scholar]
- 25.Jung YB, Jung HJ, Song KS, Kim JY, Lee HJ, Lee JS. Remnant posterior cruciate ligament-augmenting stent procedure for injuries in the acute or subacute stage. Arthroscopy. 2010;26(2):223–229. doi: 10.1016/j.arthro.2009.07.017. [DOI] [PubMed] [Google Scholar]
- 26.Lee KH, Jung YB, Jung HJ, et al. Combined posterolateral corner reconstruction with remnant tensioning and augmentation in chronic posterior cruciate ligament injuries: minimum 2-year follow-up. Arthroscopy. 2011;27(4):507–515. doi: 10.1016/j.arthro.2010.11.007. [DOI] [PubMed] [Google Scholar]
- 27.Ahn JH, Yang HS, Jeong WK, Koh KH. Arthroscopic transtibial posterior cruciate ligament reconstruction with preservation of posterior cruciate ligament fibers: clinical results of minimum 2-year follow-up. Am J Sports Med. 2006;34(2):194–204. doi: 10.1177/0363546505279915. [DOI] [PubMed] [Google Scholar]
- 28.Cooper DE, Stewart D. Posterior cruciate ligament reconstruction using single-bundle patella tendon graft with tibial inlay fixation: 2- to 10-year follow-up. Am J Sports Med. 2004;32(2):346–360. doi: 10.1177/0363546503261511. [DOI] [PubMed] [Google Scholar]
- 29.Jung YB, Jung HJ, Tae SK, Lee YS, Yang DL. Tensioning of remnant posterior cruciate ligament and reconstruction of anterolateral bundle in chronic posterior cruciate ligament injury. Arthroscopy. 2006;22(3):329–338. doi: 10.1016/j.arthro.2005.12.020. [DOI] [PubMed] [Google Scholar]
- 30.Jung YB, Tae SK, Jung HJ, Lee KH. Replacement of the torn posterior cruciate ligament with a mid-third patellar tendon graft with use of a modified tibial inlay method. J Bone Joint Surg Am. 2004;86(9):1878–1883. doi: 10.2106/00004623-200409000-00004. [DOI] [PubMed] [Google Scholar]
- 31.Kim SJ, Chang JH, Kang YH, Song DH, Park KY. Clinical comparison of anteromedial versus anterolateral tibial tunnel direction for transtibial posterior cruciate ligament reconstruction: 2 to 8 years' follow-up. Am J Sports Med. 2009;37(4):693–698. doi: 10.1177/0363546509333005. [DOI] [PubMed] [Google Scholar]
- 32.Kim SJ, Choi CH, Kim HS. Arthroscopic posterior cruciate ligament tibial inlay reconstruction. Arthroscopy. 2004;20(Suppl 2):149–154. doi: 10.1016/j.arthro.2004.04.023. [DOI] [PubMed] [Google Scholar]
- 33.Noyes FR, Barber-Westin S. Posterior cruciate ligament replacement with a two-strand quadriceps tendon-patellar bone autograft and a tibial inlay technique. J Bone Joint Surg Am. 2005;87(6):1241–1252. doi: 10.2106/JBJS.D.02272. [DOI] [PubMed] [Google Scholar]
- 34.Wang CJ, Weng LH, Hsu CC, Chan YS. Arthroscopic single-versus double-bundle posterior cruciate ligament reconstructions using hamstring autograft. Injury. 2004;35(12):1293–1299. doi: 10.1016/j.injury.2003.10.033. [DOI] [PubMed] [Google Scholar]
- 35.Houe T, Jorgensen U. Arthroscopic posterior cruciate ligament reconstruction: one- vs. two-tunnel technique. Scand J Med Sci Sports. 2004;14(2):107–111. doi: 10.1111/j.1600-0838.2003.00318.x. [DOI] [PubMed] [Google Scholar]
- 36.Fanelli GC, Larson RV. Practical management of posterolateral instability of the knee. Arthroscopy. 2002;18(2 Suppl 1):1–8. doi: 10.1053/jars.2002.31779. [DOI] [PubMed] [Google Scholar]
- 37.Kim SJ, Jung M, Moon HK, Kim SG, Chun YM. Anterolateral transtibial posterior cruciate ligament reconstruction combined with anatomical reconstruction of posterolateral corner insufficiency: comparison of single-bundle versus double-bundle posterior cruciate ligament reconstruction over a 2- to 6-year follow-up. Am J Sports Med. 2011;39(3):481–489. doi: 10.1177/0363546510385398. [DOI] [PubMed] [Google Scholar]
- 38.Yoon KH, Bae DK, Song SJ, Cho HJ, Lee JH. A prospective randomized study comparing arthroscopic single-bundle and double-bundle posterior cruciate ligament reconstructions preserving remnant fibers. Am J Sports Med. 2011;39(3):474–480. doi: 10.1177/0363546510382206. [DOI] [PubMed] [Google Scholar]
- 39.Jung YB, Tae SK, Yang DL, Han JN, Song IS, Kang IK. Magnetic resonance imaging on posterior cruciate ligament injury: can the PCL hea. J Korean Knee Soc. 2000;12(2):172–179. [Google Scholar]
- 40.Shelbourne KD, Jennings RW, Vahey TN. Magnetic resonance imaging of posterior cruciate ligament injuries: assessment of healing. Am J Knee Surg. 1999;12(4):209–213. [PubMed] [Google Scholar]
- 41.Tewes DP, Fritts HM, Fields RD, Quick DC, Buss DD. Chronically injured posterior cruciate ligament: magnetic resonance imaging. Clin Orthop Relat Res. 1997;(335):224–232. [PubMed] [Google Scholar]
- 42.Jung YB, Jung HJ, Yang JJ, et al. Characterization of spontaneous healing of chronic posterior cruciate ligament injury: analysis of instability and magnetic resonance imaging. J Magn Reson Imaging. 2008;27(6):1336–1340. doi: 10.1002/jmri.21333. [DOI] [PubMed] [Google Scholar]
- 43.Clancy WG, Jr, Shelbourne KD, Zoellner GB, Keene JS, Reider B, Rosenberg TD. Treatment of knee joint instability secondary to rupture of the posterior cruciate ligament: report of a new procedure. J Bone Joint Surg Am. 1983;65(3):310–322. [PubMed] [Google Scholar]
- 44.Jung HJ, Kim JH, Lee HJ, et al. The isometry of two different paths for remnant-preserving posterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2013;21(5):1029–1035. doi: 10.1007/s00167-012-2111-6. [DOI] [PubMed] [Google Scholar]
- 45.Jung YB, Jung HJ, Tae SK, Lee YS, Lee KH. Reconstruction of the posterior cruciate ligament with a mid-third patellar tendon graft with use of a modified tibial inlay method. J Bone Joint Surg Am. 2005;87(Pt 2) Suppl 1:247–263. doi: 10.2106/JBJS.E.00203. [DOI] [PubMed] [Google Scholar]
- 46.Jung YB, Tae SK, Yum JK, Park KH. Retension of chronic posterior cruciate ligament injury: two cases reports. J Korean Knee Soc. 1999;11(2):226–230. [Google Scholar]
- 47.Jung YB. Recent evolution of cruciate ligament surgery of the knee. Clin Orthop Surg. 2012;4(2):103–106. doi: 10.4055/cios.2012.4.2.103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Jung YB, Jung HJ, Kim SJ, et al. Posterolateral corner reconstruction for posterolateral rotatory instability combined with posterior cruciate ligament injuries: comparison between fibular tunnel and tibial tunnel techniques. Knee Surg Sports Traumatol Arthrosc. 2008;16(3):239–248. doi: 10.1007/s00167-007-0481-y. [DOI] [PubMed] [Google Scholar]
- 49.Noyes FR, Barber-Westin SD. Posterior cruciate ligament revision reconstruction, part 1: causes of surgical failure in 52 consecutive operations. Am J Sports Med. 2005;33(5):646–654. doi: 10.1177/0363546504271210. [DOI] [PubMed] [Google Scholar]
- 50.Lee SH, Jung YB, Lee HJ, Jung HJ, Kim SH. Revision posterior cruciate ligament reconstruction using a modified tibial-inlay double-bundle technique. J Bone Joint Surg Am. 2012;94(6):516–522. doi: 10.2106/JBJS.K.00030. [DOI] [PubMed] [Google Scholar]
- 51.Jung YB, Lee YS, Jung HJ, Nam CH. Evaluation of posterolateral rotatory knee instability using the dial test according to tibial positioning. Arthroscopy. 2009;25(3):257–261. doi: 10.1016/j.arthro.2008.10.007. [DOI] [PubMed] [Google Scholar]
- 52.Strauss EJ, Ishak C, Inzerillo C, et al. Effect of tibial positioning on the diagnosis of posterolateral rotatory instability in the posterior cruciate ligament-deficient knee. Br J Sports Med. 2007;41(8):481–485. doi: 10.1136/bjsm.2006.030767. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.LaPrade RF, Wentorf F. Diagnosis and treatment of posterolateral knee injuries. Clin Orthop. 2002;(402):110–121. doi: 10.1097/00003086-200209000-00010. [DOI] [PubMed] [Google Scholar]
- 54.Edson CJ, Fanelli GC, Beck JD. Postoperative rehabilitation of the posterior cruciate ligament. Sports Med Arthrosc. 2010;18(4):275–279. doi: 10.1097/JSA.0b013e3181f2f23d. [DOI] [PubMed] [Google Scholar]
- 55.Fanelli GC. Posterior cruciate ligament rehabilitation: how slow should we go? Arthroscopy. 2008;24(2):234–235. doi: 10.1016/j.arthro.2007.09.009. [DOI] [PubMed] [Google Scholar]
- 56.Edson CJ, Fanelli GC, Beck JD. Rehabilitation after multiple-ligament reconstruction of the knee. Sports Med Arthrosc. 2011;19(2):162–166. doi: 10.1097/JSA.0b013e31821918b2. [DOI] [PubMed] [Google Scholar]
- 57.Higgins H. Geniculate articular surfaces of the femur and tibia. J Anat Physiol. 1896;30(Pt 2):292–295. [PMC free article] [PubMed] [Google Scholar]
- 58.Iwamoto J, Takeda T, Suda Y, Otani T, Matsumoto H. Conservative treatment of isolated posterior cruciate ligament injury in professional baseball players: a report of two cases. Knee. 2004;11(1):41–44. doi: 10.1016/S0968-0160(03)00114-5. [DOI] [PubMed] [Google Scholar]
- 59.Katonis P, Papoutsidakis A, Aligizakis A, Tzanakakis G, Kontakis GM, Papagelopoulos PJ. Mechanoreceptors of the posterior cruciate ligament. J Int Med Res. 2008;36(3):387–393. doi: 10.1177/147323000803600302. [DOI] [PubMed] [Google Scholar]
- 60.Aalbersberg S, Kingma I, Ronsky JL, Frayne R, van Dieen JH. Orientation of tendons in vivo with active and passive knee muscles. J Biomech. 2005;38(9):1780–1788. doi: 10.1016/j.jbiomech.2004.09.003. [DOI] [PubMed] [Google Scholar]
- 61.Lutz GE, Palmitier RA, An KN, Chao EY. Comparison of tibiofemoral joint forces during open-kinetic-chain and closed-kinetic-chain exercises. J Bone Joint Surg Am. 1993;75(5):732–739. doi: 10.2106/00004623-199305000-00014. [DOI] [PubMed] [Google Scholar]
- 62.Daniel DM, Stone ML, Barnett P, Sachs R. Use of the quadriceps active test to diagnose posterior cruciate-ligament disruption and measure posterior laxity of the knee. J Bone Joint Surg Am. 1988;70(3):386–391. [PubMed] [Google Scholar]
- 63.Irrgang JJ, Fitzgerald GK. Rehabilitation of the multiple-ligament-injured knee. Clin Sports Med. 2000;19(3):545–571. doi: 10.1016/s0278-5919(05)70223-4. [DOI] [PubMed] [Google Scholar]