

Abstract
This study assesses the effect of black-white differences in school quality on black-white differences in health in later life resulting from the racial convergence in school quality for cohorts born between 1910 and 1950 in southern states with segregated schools. Using data from the 1984 through 2007 National Health Interview Surveys linked to race-specific data on school quality, we find that reductions in the black-white gap in school quality led to modest reductions in the black-white gap in disability.
Keywords: Education, Health status, School quality, Health disparities
Introduction
It is well-documented that blacks have significantly poorer health outcomes than whites and that this pattern has persisted over an extended period of time, in spite of active policy attention to reducing racial differences in health (Levine et al. 2001; U.S. Department of Health and Human Services 2000; Williams and Jackson 2005). The racial differences in health are hypothesized to result largely from factors outside the health care system, such as racial differences in educational attainment (Williams and Jackson 2005). However, little is known about the impact of differences in educational quality on racial differences in health. In this article, we examine the influence of differences in school quality on black-white health differences, building on an emerging literature that suggests that school quality may be a significant determinant of later health outcomes. This article also contributes to the literature on the relationship between education and health more generally because school quality represents one dimension of education and because improvements in school quality can lead to increases in educational attainment.
To estimate the effects of school quality on black-white health differences, we build on Card and Krueger’s (1992) research on racial differences in earnings and examine changes in black-white differences in school quality for cohorts born between 1910 and 1950 in southern states with segregated schools. Pupil-teacher ratios dramatically decreased and length of the school year and average teachers’ wages increased in the schools attended by black students and schools attended by white students in the 18 southern states prior to desegregation in the mid-1960s. In this analysis, we construct an index of school quality based on these three measures—the pupil-teacher ratio, length of the school year, and average teachers’ wages—because these inputs plausibly influenced the increase of human capital during a year of completed schooling and these measures were the primary components of per pupil expenditures (Margo 1990). During this period, quality of white schools and black schools converged as the quality of black schools improved more than the quality of white schools (Card and Krueger 1992; Margo 1990).
Our empirical approach relies on the assumption that the racial convergence in school quality within states and over time was conditionally uncorrelated with unobserved variables that also affected the differences in the health status of blacks and whites later in life. This assumption is premised on previous research suggesting that the determinants of the convergence in school quality during this time were primarily the states’ historical demographics, which led to litigation and private philanthropy that improved the quality of schools attended by black students—all of which are plausibly unrelated to health disparities more than 30 years later except through changes in school quality (Card and Krueger 1992; Donohue et al. 2002; Margo 1990).
We model black-white differences in health outcomes measured between 1984 and 2007 using data from the National Health Interview Surveys (NHIS). Using the restricted-access files, we link the NHIS data to average measures of the pupil-teacher ratio, annual teacher pay, and length of the school year for black and white schools in southern states taken from Card and Krueger (1992). We use race-, state-, and birth cohort-specific data on infant mortality rates from vital statistics records and average family size and socioeconomic characteristics constructed from the decennial censuses to control for other factors that may have been correlated with changes in black-white school quality and black-white health outcomes later in life.
We find evidence suggesting that reductions in the black-white gap in school quality led to reductions in the black-white gap in disability. This result is robust to controlling for race-specific proxies for local health and socioeconomic conditions that prevailed when individuals were attending school. We do not find an effect on the black-white gap in terms of body mass index, smoking, or self-rated health. Our main set of models does not reveal a significant effect on the black-white mortality gap, although we do find some tentative evidence of an effect when we drop the oldest birth cohorts, which are most subject to selective mortality. This article provides some of the first evidence of the influence of improvements in school quality on long-run population health disparities.
Background
In the United States, blacks have significantly poorer outcomes than whites for most health and health behavior indicators. A number of factors are hypothesized to explain racial health differences, including racial differences in socioeconomic status.1 In particular, educational attainment explains a substantial proportion of racial differences in health, although the magnitude of that proportion varies depending on the health outcome and population (Guralnik et al. 1993). This article considers the relationship between racial differences in school quality and long-run racial differences in health.
Fundamental to understanding how racial differences in school quality affect racial differences in health is understanding how school quality might affect health in the first place. Conceptual models of health posit that more human capital makes individuals more knowledgeable about promoting and maintaining their health and more effective at acting on that knowledge (Grossman 1972). Within the context of this model, school quality may affect health through several distinct mechanisms. First, improvements in school quality may lead to increased educational attainment (Card and Krueger 1996), and evidence suggests a causal effect of educational attainment on health (Lleras-Muney 2005). We highlight three specific mechanisms through which educational attainment might affect health: employment, cognition, and social-psychological resources. Education influences employment opportunities, enabling individuals to choose jobs with higher wages, which allows individuals to purchase greater medical care (Cutler and Lleras-Muney 2008; Grossman 1972; Smith 1999). Individuals with higher education are also more likely to be employed and to choose occupations with higher social prestige, safer workplaces, greater control of work schedules, less stress, and more generous health insurance— all of which can influence health (Fletcher and Frisvold 2009; Ross and Wu 1995). Education may improve cognitive ability, enabling individuals to make better health care choices, respond more quickly to new information and technological advances, more effectively gather information, and more effectively communicate with medical care providers (Cutler and Lleras-Muney 2010; Glied and Lleras-Muney 2008; Lochner 2011). Education may also influence individual’s social-psychological resources, including a sense of personal control and social support, which are positively correlated with engaging in preventive behaviors and having fewer psychological problems (Ross and Mirowsky 1999; Ross and Wu 1995). Thus, as a result of these mechanisms through which educational attainment influences health, an increase in attainment because of improved school quality would be expected to affect health positively.
Second, improvements in school quality may increase the marginal health returns to schooling. In this case, among individuals with the same years of schooling, health outcomes will be greater for those who attended better-quality schools (Ross and Mirowsky 1999). This may occur if better-quality schooling leads to greater marginal improvements in cognitive or noncognitive skills (such as a personal sense of control) that matter for health outcomes, relative to lower-quality schooling. In addition, if better-quality schools increase the marginal returns to schooling in terms of wages or occupational status, there may also be increased marginal health returns if income and occupational conditions affect health as described earlier (Ross and Mirowsky 1999). For example, Frisvold and Golberstein (2011) found that for southern-born blacks, improvements in school quality increase the marginal health returns to schooling for a number of health and health behavior outcomes. Thus, to the extent that there are differences in quality between black and white schools, one might expect to see resulting health differences between blacks and whites.
Our research focuses on changes in school quality in the southern United States in the early to mid-twentieth century. This was an era of racially segregated schools: although Brown v. Board of Education in 1954 ruled that “separate but equal” schools were unconstitutional, schools remained segregated, for the most part, until the Civil Rights Act of 1964 (Ashenfelter et al. 2006). Three points about southern segregated schools are particularly salient. First, on average, white students attended schools that had far greater quality than black students. Between the Civil War and around 1915, blacks began to attend newly formed schools with black teachers, and blacks’ school attendance exceeded that of low-income whites (Anderson 1985). However, following Reconstruction, landowning whites regained control of the state governments and limited the expansion of black public schools through the South; the percentage of black children attending public schools decreased between 1880 and 1900 (Anderson 1985; Margo 1990). At the same time, whites appropriated more of their states’ total school resources to themselves, which increased the quality of white schools and increased the demand for schooling among whites (Margo 1990).
Second, between 1915 and 1966, the quality of black and white schools converged, overall. Although school quality in the South improved in white schools following the Reconstruction period in the late 1800s, it was not until around 1915 that school quality improved for black schools in the South (Margo 1990). After 1915, measures of school quality improved for both whites and blacks, and blacks experienced relatively greater improvements than whites. For example, Card and Krueger (1992) documented that in 1915, the average pupil-teacher ratio was 61 in black schools but 38 in white schools; by 1966, however, the average pupil-teacher ratios had nearly converged (26 for black schools and 24 for white schools). Based on data from Card and Krueger (1992), Fig. 1 displays the convergence in the average pupil-teacher ratio, teachers’ wages, and the length of the school year between 1915 and 1966, which are three commonly used proxies for school quality in the early and mid-twentieth century. As shown in the graph, the convergence in the pupil-teacher ratio was reasonably constant, with the largest decline occurring in the 1920s. The convergence in the length of the school year occurred most dramatically in the 1930s, and the majority of the convergence in teachers’ wages occurred in the 1940s.
Fig. 1.
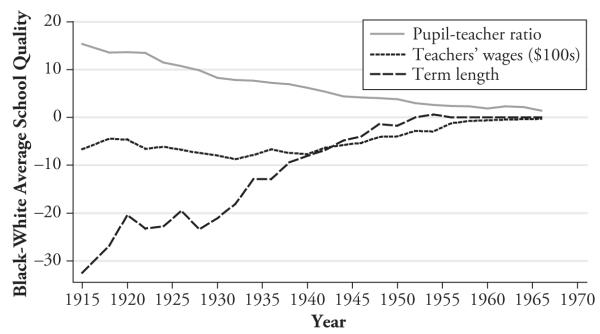
Convergence in school quality in the South. Source: Card and Krueger (1992)
Third, the aggregate trend of racial convergence in school quality masks considerable variation in black-white school quality both across southern states and over time (Card and Krueger 1992, 1996; Margo 1990). Figure 2 displays the variation in school quality differences across states and over time by showing the black minus white average pupil-teacher ratio for all southern states in 1920, 1940, and 1960. In 1920, Alabama, Florida, Louisiana, Mississippi, and South Carolina each averaged 20 more students per teacher in black schools than in white schools. By 1960, this difference was reduced almost to zero in Alabama and Florida. The difference in the pupil-teacher ratio in Arkansas, Georgia, and Virginia was about 15 students in each state in 1920, but by 1960, the difference had fallen to about 2 students in Georgia and Virginia and to 7 students in Arkansas. Thus, racial school quality differences vary considerably across states and over time, and this variation is the focus of our article.
Fig. 2.
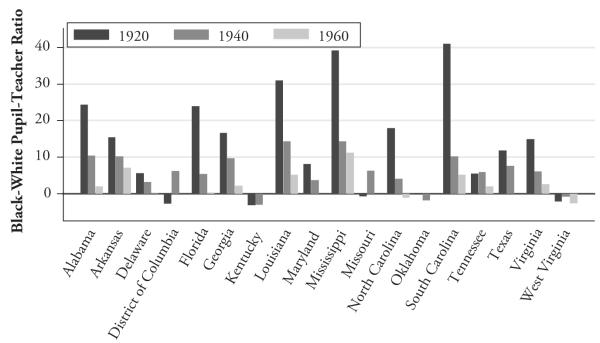
The black-white pupil-teacher ratio in 1920, 1940, and 1960 for each state in the South. Source: Card and Krueger (1992)
Key reasons for the convergence in school quality throughout the South were private philanthropy from the North (and specifically from the Rosenwald Fund) and the National Association for the Advancement of Colored People’s (NAACP) legal campaign to enforce “separate but equal” standards, both of which were directed toward states with the highest percentages of blacks in the population (Card and Krueger 1992; Donohue et al. 2002).2 In an effort to maximize the impact of the contributions, the Rosenwald Fund targeted states that provided the least amount of funding to black school districts (Donohue et al. 2002), which were the states with the historically highest proportion of blacks in the population.3 After achieving early victories in Maryland and Virginia, the NAACP targeted states with the most unequal financing between black schools and white schools, which violated the equality provisions of the separate-but-equal doctrine established in Plessy v. Ferguson (Donohue et al. 2002); these states were the seven states with the highest percentages of blacks in the population around the turn of the century.
Thus, as described by Margo (1990) and Card and Krueger (1992, 1996), the primary determinant of the variation in school quality both across states and within states over time was the relative historical size of the black population in the state, which influenced the timing and location of Northern philanthropy and the NAACP’s legal actions. For example, Card and Krueger (1996) noted that the percentage of the population that was black was nearly twice as high in South Carolina as it was in North Carolina. The relative size of the black population in southern states in the early 1900s was primarily determined by the differing use of slave labor across states based on the type of crops farmed, and thus the geography and weather of the state (Card and Krueger 1992, 1996; Cooper and Terrill 1991; Fogel and Engerman 1974; Wright 1986).4
Prior research investigated the role of school quality in explaining racial differences in income. Card and Krueger (1992) studied within-state over-time variation in state-level school quality and found that the convergence in school quality for blacks and whites born in the South between 1910 and 1950 led to a significant convergence in the racial wage gap for working males. Aaronson and Mazumder (2011) found that the expansion of Rosenwald schools led to gains in educational attainment, cognitive skills, and wages for blacks relative to whites. Johnson (2010) found that the racial convergence in school quality resulting from school desegregation for the 1950–1970 birth cohorts led to a convergence in years of schooling, earnings, and self-rated heath (the only health outcome he observed). We build on this previous research by examining the influence of the convergence in school quality among segregated schools in the South on a variety of long-run health behaviors and outcomes.
Econometric Strategy
To assess the impact of differences in the quality of schools attended, we compare the average health outcomes of blacks and whites who were born in the same state in different cohorts and experienced differences in school quality. Specifically, we estimate regression models with the following specification:
| (1) |
where is the average value of the health measure for blacks born in southern state s of cohort c measured at time t for sex g; is the corresponding measure for whites; is the average school quality for black schools in state s of cohort c; is the corresponding measure for white schools; γ represents state-of-birth fixed effects; ϕ represents cohort fixed effects; μ represents survey year fixed effects; δ represents a dummy variable for sex; and ε denotes random error. We focus on cohorts born between 1910 and 1950 in the 18 segregated states in the South and examine health outcomes measured between 1984 and 2007. The parameter of interest is β , which is identified from changes over time in state-specific and cohort-specific differences in quality between black and white schools. This parameter represents the reduced-form impact of improvements in school quality, which incorporates the impact of the resulting improvements in educational attainment.
By focusing on within-state and over-time variation in the difference in quality for black and white schools, we control for time-invariant state characteristics that influence health as well as all time-varying state characteristics that influence the health of blacks and whites similarly. As such, this approach accounts for permanent differences in health outcomes for blacks and whites born in different states. Additionally, as Card and Krueger (1992) noted, taking the black-white difference on both sides of Eq. (1) is equivalent to a specification that includes state-by-cohort-by–survey year fixed effects.
Nevertheless, given the social changes that occurred in the South during this period, black-white changes in school quality may have been correlated with black-white changes in contemporary conditions that may have affected health later in life. Thus, our models also include the black-white difference in state- and cohort-specific measures of infant mortality rates (IMR) when each cohort reached age 6 and thus would have started school as a measure of black-white differences in contemporaneous health conditions. IMR is a useful covariate for several reasons. First, IMR has been shown to be sensitive to changes in local health care resources (Almond et al. forthcoming) and environmental conditions (Chay and Greenstone 2003), implying that if there were changes in health care resources or environmental conditions that were correlated with changes in school quality and might affect health later in life, we would expect them to be reflected in IMR. Second, IMR is also responsive to social and economic conditions (Fishback et al. 2001), implying that if there were changes in social or economic conditions that may have been correlated with changes in school quality, we would also expect those changes to be reflected in IMR.
Further, we also include the black-white differences in state- and cohort-specific measures of socioeconomic status that might be correlated with the demand for school quality. Two interrelated trends occurring during this period in the South were the decline in child labor and the decline in family size (Tolnay 1999). These trends may relate to the demand for schooling and school quality as households sent their children to school in order to gain human capital while forgoing the short-term benefits of child labor, which declined during this period.5 We control for these trends and socioeconomic status more generally with black-white differences in state- and cohort-specific average family size and the average occupational education score, which is the percentage of individuals in each respondent in the state’s occupational category who completed at least one year of college, measured when each cohort would have been entering school at age 6. Thus, we augment Eq. (1):
| (2) |
where and are the state-specific and cohort-specific infant mortality rates for blacks and whites, and and are the state-specific and cohort-specific measures of socioeconomic status for blacks and whites.
Equation (2) represents our preferred specification. For our estimates of β in Eq. (2) to be biased would require unobserved variables that affect health later in life, vary within states and over time in a way that is correlated with the changes in black-white school quality, and are uncorrelated with changes in the black-white difference in IMR or socioeconomic status. Historical evidence does not suggest that, based on these conditions, β will be biased. The geographic patterns of convergence in school quality are not correlated with the introduction of food programs in schools (Mazumder 2007), vaccination requirements for school attendance (Mazumder 2007), the establishment of state boards of health (Cooper and Terrill 1991), or increases in the number of black hospitals (Rice and Jones 1994). The introduction of water filtration and chlorination systems in major U.S. cities between 1900 and 1936 reduced infant mortality, and minority neighborhoods may have received clean water later than white neighborhoods, although there is no evidence to suggest that the local introduction of this technology mirrored local school quality changes (Cutler and Miller 2005; Troesken 2002). Nevertheless, we control for black-white differences in IMR to reduce the possibility that any improvements in public health bias our results.6
Four major diseases that were prominent in the South and were largely eradicated in the first half of the 1900s were yellow fever, pellagra, malaria, and hookworm (Humphreys 2009). Hookworm eradication affected human capital accumulation, with greater effects on black populations than on white populations (Bleakley 2007). Unfortunately, data on hookworm prevalence are not available at the state and race level over our study period, preventing us from directly including it as a covariate. To further examine whether our estimates of the influence of changes in school quality reflect changes in the health conditions among states, we examine the robustness of the results from Eq. (2) to excluding states that were most affected by the hookworm eradication campaign in the early 1900s. Because hookworm was largely eradicated by 1930, we exclude from these models the 1910–1929 birth cohort observations from the six states with estimates of hookworm prevalence in 1918 that were at least 25 %.7
We also examine the robustness of our results to bias from selective mortality. If the convergence in school quality affects racial differences in mortality, then the health of the surviving population would differ from the health of the population in the absence of the effect on mortality. Because the bias from selective mortality should be most severe among older cohorts, we examine the sensitivity of our results to excluding the 1910 cohort.
Further, as noted earlier, school quality can influence health through employment opportunities and income, and prior research has found that improvements in school quality for southern-born blacks relative to whites led to a convergence in the black-white difference in income (Aaronson and Mazumder 2011; Card and Krueger 1992). Because income is hypothesized to be an important determinant of health (Meer et al. 2003), we examine whether our results are mediated by family income. To do this, we modify Eq. (2) by adding a term for the black-white difference in average current family income (Y) as measured in the NHIS:
| (3) |
This exercise has several important limitations, including the potential endogeneity of average family income and the lack of a better measure of permanent income, such that we view the results of Eq. (3) as merely suggestive of the potential influence of income.8 Another potential mechanism that is salient in this historical context is migration. Both the quantity and quality of education were related to migrating to the North for southern blacks (Aaronson and Mazumder 2011; Tolnay 1998), and Black et al. (2011) suggested that migration from the South to the North during adulthood led to an increase in mortality. Thus, we also estimate a specification similar to Eq. (3) that controls for the black-white difference in the state-specific, cohort-specific percentage of individuals who currently reside outside of the South to examine whether emigration can partially explain the impact of school quality. In addition, we investigate whether black-white differences in health insurance coverage mediate the relationship between school quality and health outcomes by estimating a model that controls for the black-white difference in the state-specific and cohort-specific percentage of individuals with any health insurance.
As a final note, for each of our outcomes, our regression models are weighted by the inverse of the variance of each cell, where the variance for each cell is estimated as follows:
where N is the number of observations for each group in each cell. We estimate all models with heteroskedasticity-robust standard errors clustered on the state of birth.
Data
Our data come from the 1984 through 2007 National Health Interview Surveys (NHIS). The NHIS is conducted annually by the National Center for Health Statistics and collects extensive survey data on health status and sociodemographic information. The NHIS is nationally representative and contains large samples, collecting data from between 60,000 and 120,000 individuals per year between 1984 and 2007. We use the restricted-use versions of the NHIS, which allows us to link respondents with their state of birth and with detailed mortality information. The state-of-birth data are self-reported, and the mortality data track mortality status through the end of 2006 from the National Death Index. State of birth was not collected prior to 1984.
We restrict our sample to include only blacks and whites who were born between 1910 and 1950 in southern states.9 We aggregate the data into cells for analysis of black-white differences in health outcomes based on race, sex, state of birth, 10-year birth cohort (1910– 1920, 1921–1930, 1931–1940, and 1941–1950), and NHIS survey year (using four 6-year categories: 1984-1989, 1990–1995, 1996–2001, and 2002–2007). Within each cell, we calculate the mean of our health outcome variables, the IMR covariate, and our school quality variables (described later), and then take the difference between the analogous cell means between blacks and whites. After dropping cells with fewer than 10 blacks and 10 whites, 462 cells remain for our analyses.10
We focus on several domains of health outcomes. The first domain is mortality, for which the dependent variable is the black-white difference in the proportion of individuals who died by the end of 2006. Our second domain is general health status, for which the dependent variable is the black-white difference in the cell mean of the five-level self-rated health measure (1 = excellent health, 5 = poor health). Our third domain is disability, for which the dependent variable is the black-white difference in the proportion reporting any activity limitations resulting from chronic health conditions. Our fourth domain is weight-related outcomes. We look at the black-white difference in mean body mass index (BMI) and the black-white difference in proportion obese (BMI >30). Our final domain is smoking behavior; we look at black-white differences in the proportion reporting that they ever smoked (smoked at least 100 cigarettes in their lifetime) and in the proportion reporting being a current smoker.
We construct a single index of school quality using factor analysis that is derived from three measures of school quality: average pupil-teacher ratio, average term length (measured in days per school year), and average teacher wages (expressed in 1967 dollars) for grades K–12 in public schools.11 Card and Krueger (1992) used these measures, which were derived from data in the Biennial Surveys of Education, state education reports, and annual reports from the Southern Education Reporting Service.12 Because of the segregated nature of schools in the South between 1915 and 1966, these school quality measures are available separately for black and white students. To construct the individual measures of educational quality, we follow Card and Krueger (1992) and use data from the 1970 census to derive the average of the quality measures based on the years that each individual in each race-state-cohort attended school, which is determined based on the number of years of schooling attended, state of birth, and the year in which the individual was 6 years old. These values for individuals are then averaged to determine the school quality for each cohort within each state.13 We then construct an index of overall school quality based on these three measures using factor analysis. We retain the one factor with a positive eigenvalue, which has positive factor loadings for teachers’ wages and term length, has a negative factor loading for the pupil-teacher ratio, and is consistent with the factor variable reflecting an overall indicator of school quality. The magnitudes of the factor loadings for all three measures are similar (although the factor loading is slightly weaker for teachers’ wages than for pupil-teacher ratio and term length), implying that the three measures are reasonably correlated with one another and that the variation in the summary measure reflects the variation in all three measures. We report the results for this single index in the main tables.14 Using this summary measure of school quality has two main advantages: (1) it provides a less-noisy measure of the underlying school quality construct than the individual school quality measures, and (2) it reduces the number of statistical tests in our analyses by two-thirds. For transparency, we also include the regression results based on each separate quality measure in Table 5 in the appendix.
We also include the black-white differences in infant mortality rates (IMR) and socioeconomic status as covariates in our models. The IMR data are state-, cohort-, and race-specific; they are collected from U.S. vital statistics records and are publicly available in various years of the Statistical Abstracts of the United States and Vital Statistics of the United States. For cases with missing IMR data for which it was possible to interpolate, we did so using linear interpolation. In our analyses, we consider the state-, cohort-, and race-specific IMR when each cohort was 6 years old as a proxy for the stock of health resources that were available when cohorts were entering school, with the understanding that numerous inputs to health stock exist, including access and quality of health care as well as social, economic, and environmental inputs. We include the state-, cohort-, and race-specific average family size and average occupational education score as measures of socioeconomic status upon school entry at age 6 for each cohort; these variables are derived from decennial census data (Ruggles et al. 2010) and are constructed by linearly interpolating these measures for the years between the decennial censuses.
Table 1 presents summary statistics for the school quality and health measures for blacks and whites and the differences between the two races among individuals born between 1910 and 1950 in the segregated southern states. On average, blacks attended schools with five more students per teacher, with teachers who were paid almost $500 less (in 1967 dollars), and with a school year that was 6.5 days shorter than among schools attended by whites. The average summary measure of school quality is 0.566 lower for blacks than whites, and the standard deviation of the black-white difference in school quality is 0.726. Blacks are also disadvantaged, compared with whites, for nearly all health measures. For example, blacks are more likely to be limited in their daily activities, have a higher average BMI, have a BMI that is higher throughout the right side of the BMI distribution, currently smoke, and have lower quality self-reported health.
Table 1.
Summary statistics of school quality and health measures for blacks and whites
| Blacks | Whites | Black – White | ||||
|---|---|---|---|---|---|---|
|
|
||||||
| Variable | Mean | SD | Mean | SD | Mean | SD |
| School Quality Index | −0.251 | (1.061) | 0.315 | (0.490) | −0.566 | (0.726) |
| Pupil-Teacher Ratio | 33.935 | (6.925) | 28.774 | (2.805) | 5.161 | (5.509) |
| Teachers’ Wages (000s) | 2.828 | (1.484) | 3.315 | (1.183) | −0.487 | (0.459) |
| Term Length | 166.068 | (17.380) | 172.579 | (7.754) | −6.510 | (12.377) |
| Mortality | 0.268 | (0.198) | 0.219 | (0.196) | 0.049 | (0.065) |
| Self-reported Health | 2.972 | (0.285) | 2.603 | (0.318) | 0.369 | (0.197) |
| Excellent or Very Good Self-reported Health | 0.338 | (0.097) | 0.480 | (0.117) | −0.142 | (0.080) |
| Fair or Poor Self-reported Health | 0.339 | (0.104) | 0.229 | (0.090) | 0.109 | (0.069) |
| Any Limitations | 0.336 | (0.118) | 0.273 | (0.102) | 0.063 | (0.070) |
| Body Mass Index | 27.969 | (1.276) | 26.151 | (1.066) | 1.818 | (1.664) |
| Underweight | 0.013 | (0.015) | 0.021 | (0.018) | −0.008 | (0.020) |
| Overweight | 0.690 | (0.083) | 0.554 | (0.125) | 0.136 | (0.1410) |
| Obese | 0.295 | (0.102) | 0.183 | (0.058) | 0.113 | (0.102) |
| Morbidly Obesity | 0.102 | (0.062) | 0.049 | (0.024) | 0.053 | (0.056) |
| Ever Smoked | 0.575 | (0.163) | 0.580 | (0.148) | −0.005 | (0.098) |
| Currently Smoke | 0.312 | (0.140) | 0.261 | (0.097) | 0.051 | (0.099) |
| Infant Mortality Rate | 70.571 | (25.122) | 44.702 | (15.305) | 25.869 | (12.333) |
| Family Size | 4.636 | (0.694) | 4.393 | (0.299) | 0.243 | (0.631) |
| Duncan SEI Occupational Education Score | 331.369 | (35.417) | 422.337 | (26.625) | −90.968 | (40.701) |
| Income | 27,667.92 | (9,529.74) | 38,555.12 | (11,427.65) | −10,887.19 | (4,446.76) |
| Reside in the South | 0.618 | (0.217) | 0.799 | (0.157) | −0.181 | (0.157) |
| Number of Observations | 462 | 462 | 462 | |||
Notes: This table displays the means and standard deviations for blacks and for whites, and the mean for blacks minus the mean for whites in health and school quality for individuals born in the 18 southern states between 1910 and 1950.
Sources: National Health Interview Survey 1984–2007; Card and Krueger (1992).
Results
Table 2 displays the estimates of the effect of black-white school quality differences on black-white health outcomes as in Eq. (1), along with our preferred estimates of the effect net of trends in racial differences in infant health and socioeconomic status from Eq. (2).15 As shown in the first row of Table 2, the relationship between black-white school quality and black-white self-rated health is in the expected direction, but the estimate is small in magnitude and statistically insignificant in both specifications. Similarly, we do not find any significant relationship between racial differences in school quality and racial differences in BMI or obesity. The results for having ever smoked and current smoking status are also statistically insignificant. However, the signs of the coefficients in the smoking models would suggest that the convergence in school quality led to a divergence in ever smoking and, conditional on that divergence, a convergence in quitting among those who ever smoked. This pattern, although not statistically significant at conventional levels, is consistent with other research suggesting that more schooling is associated with more smoking for cohorts that completed their schooling before smoking risks were widely known, and the educational differences in smoking emerged only after the Surgeon General’s 1964 warning about the dangers of tobacco use (de Walque 2010).
Table 2.
The influence of black-white differences in school quality on black-white differences in health
| Eq. (1) | Eq. (2) | |
|---|---|---|
| Panel A: Self-rated Health | ||
| Black-white school quality | −0.00506 (0.0218) |
−0.00434 (0.0270) |
| R 2 | .459 | .459 |
| Panel B: Body Mass Index | ||
| Black-white school quality | 0.0224 (0.0843) |
0.0544 (0.0868) |
| R 2 | .829 | .830 |
| Panel C: Obesity | ||
| Black-white school quality | −0.00575 (0.0104) |
−0.00112 (0.00880) |
| R 2 | .671 | .675 |
| Panel D: Ever Smoked | ||
| Black-white school quality | 0.0226 (0.0189) |
0.0197 (0.0164) |
| R 2 | .345 | .356 |
| Panel E: Currently Smoke | ||
| Black-white school quality | −0.00627 (0.0100) |
−0.0102 (0.0113) |
| R 2 | .328 | .333 |
| Panel F: Any Limitations | ||
| Black-white school quality | −0.0158† (0.00783) |
−0.0208* (0.00873) |
| R 2 | .280 | .282 |
| Panel G: Mortality | ||
| Black-white school quality | −0.00645 (0.0121) |
−0.0143 (0.0150) |
| R 2 | .364 | .377 |
| Observations | 462 | 462 |
Notes: Heteroskedasticity-robust standard errors that allow for clustering within state of birth are in parentheses.
Each coefficient estimate is based on a separate regression. Additional covariates in Eq. (1) that are not shown include cohort fixed effects, survey-year fixed effects, and state fixed effects. Eq. (2) also includes the black-white difference in infant mortality rate, average family size, and the average Duncan SEI occupational education score.
Sources: National Health Interview Survey 1984–2007; Card and Krueger (1992).
p < .10;
p < .05
Relative improvements in school quality are related to differences in disability status, and this result is robust to controlling for black-white differences in the infant mortality rate and socioeconomic conditions. In the preferred specification, a one-unit increase in the school quality index of black schools relative to white schools reduces the likelihood of having a disability by .021 more for blacks than for whites. Although statistically significant (p = .029), this effect is modest in magnitude. A 1 standard deviation reduction in the black-white school quality gap leads to a 0.22 standard deviation decrease in the black-white disability gap. Finally, there is no statistically significant relationship between differences in school quality and differences in mortality, although the coefficient is suggestive of a decrease in racial differences in mortality as a result of the convergence in school quality.
The results presented in Table 3 allow us to examine the robustness of these relationships. The first column repeats the results from Eq. (2). The second column restricts the sample to exclude individuals born between 1910 and 1929 in states with high hookworm rates to examine whether these results are driven by the public health improvements resulting from the near eradication of hookworm. The third column restricts the sample to exclude the 1910–1920 cohorts to examine the potential influence of selective mortality, given that the oldest cohorts are most likely to be affected by any selective mortality. As shown in these three columns, the relationship between school quality and disability status is robust for these restricted samples and specifications. One other interesting result emerges from these analyses. When we exclude the 1910–1920 birth cohorts, which we expect to be the most affected by selective mortality, the estimate for black-white differences in mortality doubles in magnitude and is statistically significant at the 5 % level. This estimate, which we regard as a tentative finding, suggests that a 1 standard deviation improvement in relative school quality decreases black-white differences in mortality by 0.32 standard deviations among younger cohorts born between 1920 and 1950.
Table 3.
The robustness of estimates of the influence of black-white differences in school quality on black-white differences in health
| Eq. (2) | Excluding States With High Hookworm Rates |
Excluding the 1910 Cohort |
|
|---|---|---|---|
| Panel A: Self-rated Health | |||
| Black-white school quality | −0.00434 (0.0270) |
−0.0146 (0.0280) |
0.00305 (0.0285) |
| R 2 | .459 | .472 | 0.463 |
| Panel B: Body Mass Index | |||
| Black-white school quality | 0.0544 (0.0868) |
0.0818 (0.108) |
0.0769 (0.101) |
| R 2 | .830 | .837 | .849 |
| Panel C: Obesity | |||
| Black-white school quality | −0.00112 (0.00880) |
−0.00372 (0.00871) |
−0.000539 (0.00955) |
| R 2 | .675 | .682 | .687 |
| Panel D: Ever Smoked | |||
| Black-white school quality | 0.0197 (0.0164) |
0.0294 (0.0184) |
0.0179 (0.0222) |
| R 2 | .356 | .359 | .338 |
| Panel E: Currently Smoke | |||
| Black-white school quality | −0.0102 (0.0113) |
−0.00942 (0.0145) |
0.00280 (0.0188) |
| R 2 | .333 | .333 | .313 |
| Panel F: Any Limitations | |||
| Black-white school quality | −0.0208* (0.00873) |
−0.0207† (0.0117) |
−0.0192† (0.0109) |
| R 2 | .282 | .296 | .294 |
| Panel G: Mortality | |||
| Black-white school quality | −0.0143 (0.0150) |
−0.0151 (0.0184) |
−0.0288* (0.0124) |
| R 2 | .377 | .394 | .415 |
| Observations | 462 | 392 | 406 |
Notes: Heteroskedasticity-robust standard errors that allow for clustering within state of birth are in parentheses.
Each coefficient estimate is based on a separate regression. Additional covariates that are not shown include black-white differences in infant mortality rate, average family size, and the average Duncan SEI occupational education score; cohort fixed effects; survey-year fixed effects; and state-of-birth fixed effects.
Sources: National Health Interview Survey 1984–2007; Card and Krueger (1992).
p < .10;
p < .05
In Table 4, we examine the mechanisms underlying our main results. As described earlier, the mechanisms through which black-white school quality differences lead to a reduction in black-white health differences include employment opportunities and occupational characteristics, cognition, and social-psychological resources. We focus on variables related to these mechanisms that are available in each of the NHIS survey waves, and we examine whether the results from Table 2 are mediated by family income, emigration from the South, or health insurance coverage. For most outcomes, including black-white differences in current income as measured in the NHIS does not attenuate the coefficients on the black-white school quality differences. A statistically significant relationship between school quality and disability status remains, and the estimate becomes slightly larger in magnitude. These results suggest that income does not play an important mediating role in the relationship between differences in school quality and disability status. Including black-white differences in the percentage of individuals who currently reside in the South shows that migration influences the estimates of the relationship between school quality and health in the opposite direction of income for disability status. These results suggest that black-white differences in school quality had a stronger impact on disability differences among individuals who emigrated from the South, although the change in the magnitude of the estimate is small (about 12 %).16 Finally, the results in Table 4 also suggest that health insurance coverage does not mediate the relationship between black-white differences in school quality and black-white differences in health.17
Table 4.
Potential mechanisms through which black-white differences in school quality influence black-white differences in health
| Eq. (2) |
Eq. (2) + Family Income |
Eq. (2) + Migration to the North |
Eq. (2) + Health Insurance |
|
|---|---|---|---|---|
| Panel A: Self-rated Health | ||||
| Black-white school quality | −0.00434 (0.0270) |
−0.0221 (0.0258) |
−0.00647 (0.0258) |
−0.00672 (0.0274) |
| R 2 | .459 | .505 | .461 | .473 |
| Panel B: Body Mass Index | ||||
| Black-white school quality | 0.0544 (0.0868) |
−0.0207 (0.0757) |
0.0240 (0.0859) |
0.0489 (0.0807) |
| R 2 | .830 | .836 | .835 | .831 |
| Panel C: Obesity | ||||
| Black-white school quality | −0.00112 (0.00880) |
−0.00794 (0.00807) |
−0.00239 (0.00841) |
−0.00139 (0.00851) |
| R 2 | .675 | .692 | .678 | .677 |
| Panel D: Ever Smoked | ||||
| Black-white school quality | 0.0197 (0.0164) |
0.0196 (0.0167) |
0.0200 (0.0160) |
0.0176 (0.0169) |
| R 2 | .356 | .356 | .356 | .369 |
| Panel E: Currently Smoke | ||||
| Black-white school quality | −0.0102 (0.0113) |
−0.0115 (0.0117) |
−0.00970 (0.0110) |
−0.00993 (0.0111) |
| R 2 | .333 | .335 | .334 | .333 |
| Panel F: Any Limitations | ||||
| Black-white school quality | −0.0208* (0.00873) |
−0.0244* (0.00845) |
−0.0183† (0.0100) |
−0.0213* (0.00897) |
| R 2 | .282 | .297 | .292 | .290 |
| Panel G: Mortality | ||||
| Black-white school quality | −0.0143 (0.0150) |
−0.0177 (0.0157) |
−0.0144 (0.0151) |
−0.0156 (0.0153) |
| R 2 | .377 | .389 | .379 | .382 |
| Observations | 462 | 462 | 462 | 462 |
Notes: Heteroskedasticity-robust standard errors that allow for clustering within state of birth are in parentheses.
Each coefficient estimate is based on a separate regression. The second column includes the estimates of Eq. (2) as shown in Tables 2 and 3. Additional covariates, as shown by the column headings, are included in each subsequent column. The third column displays the coefficients of black-white school quality from a specification that also includes family income as a control variable. A variable denoting whether the individual resides in the South in the NHIS survey year is included in the fourth column. The fifth column includes a variable denoting whether the individual has any form of health insurance. Additional covariates that are not shown include black-white differences in infant mortality rate, average family size, and the average Duncan SEI occupational education score; cohort fixed effects; survey-year fixed effects; and state-of-birth fixed effects.
Sources: National Health Interview Survey 1984–2007; Card and Krueger (1992).
p < .10;
p < .05
Conclusion
In this article, we present one of the first investigations of the effect of school quality on long-run racial differences in health. Because racial differences in health are a recalcitrant policy issue in the United States, it is important to understand how different social policy changes may affect health differences. Although there have been major changes in racial patterns of school quality in the United States, little evidence exists on the effect of school quality on racial health differences. Using within-state and over time variation in school quality from segregated southern states, we find that convergence in school quality between blacks and whites led to statistically significant, although modest, long-run effects of reducing racial gaps in disability. For example, the black-white gap in percentage with any disability for 60- to 64-year-olds grew from 0.059 in 1984–1987 to 0.091 in 2004–2007. The analogous black-white gap in the school quality index measure dropped from 1.56 in 1984–1987 to 0.38 in 2004–2007. Based on our regression results, the disability gap would have grown to 0.116 in 2004 if the average gap in the school quality index had stayed constant at the levels of the 1984–1987 cohorts. We find that the convergence in income, emigration from the South, and health insurance explains little of the relationship between differences in school quality and black-white differences in disability. A limitation of the NHIS data is that we are unable to examine other mechanisms related to occupational characteristics, cognition, and social-psychological resources.
One potential limitation of our analysis is that public health initiatives or other unobserved changes in family or individual characteristics could bias our results. For this to occur, these changes would have to mirror the changes within states and over time in the racial convergence in school quality and would have to be correlated with health later in life. To minimize this potential source of bias, we control for racial differences in the infant mortality rate and socioeconomic status that were contemporaneous with our school quality measure. We also examine the robustness of our results to excluding states with high hookworm rates that were most affected by the hookworm eradication campaign in the early 1900s. Our results suggest that the potential influences on our estimates for disability status from these concerns are likely to be minimal.
Another potential limitation of our analyses is the possibility that our results are biased by selective mortality. For the older cohorts in our sample, if racial differences in school quality led to differential mortality between blacks and whites, then we would expect that our results may actually understate the effects of school quality on racial differences in health. This direction of bias would emerge because we do not observe effects of racial differences in school quality among those who died prior to being interviewed in the NHIS and because the black survivors represented in the cells may be in relatively better health than the white survivors. Consistent with this expectation, after excluding the oldest cohorts, we find evidence that the convergence in school quality decreased racial differences in mortality. However, we also expect that our use of weights incorporating cell size minimizes differential mortality bias because the cells that experienced significant attrition prior to the NHIS are relatively less populated and thus receive relatively smaller weights in our analyses. Additionally, our main results show a small and statistically insignificant relationship between racial differences in school quality and mortality, and our disability results are robust to excluding the eldest cohort, suggesting that any bias from selective mortality is likely to be minimal.18
Our results imply that improving school quality for blacks relative to whites may lead to some modest reductions in black-white health differences later in life. Although our analysis focuses on a historical period and the external validity of the results may be limited by the social context of the period and the different alternatives to schooling during this period (primarily, child labor), it is necessary to examine changes in school quality that occurred in the past in order to understand the persistent influence of differences in school quality on racial differences in health. Although, on average, racial differences in school quality have dropped significantly from the period that we study, there is still room for improvement in current school quality. For example, Clotfelter et al. (2005) found that black students are more likely than white students to be in school districts with less-experienced teachers and, within districts, are more likely than whites to attend schools with less-experienced teachers. Although the magnitudes of our results are relatively modest, they remain important: in spite of considerable policy attention to reducing black-white differences in health, these disparities have not changed much.
Supplementary Material
Acknowledgements
This project was funded, in part, by the National Institute of Mental Health (T32 postdoctoral traineeship), the Robert Wood Johnson Foundation, Emory University Woodruff Funds, and the Emory Global Health Institute. We thank Al Headen, Ellen Meara, Frank Sloan, Jim Walker, and Ty Wilde; seminar participants at the Federal Reserve Bank of Atlanta and the University of Wisconsin; and participants at the American Society of Health Economists biennial conference, the Association for Public Policy Analysis and Management annual conference, the Census Restricted Data Center conference, and the Southeastern Health Economics Study Group for helpful comments. We thank David Card for sharing school quality data, Ken Chay for sharing hospital desegregation data, and Bhash Mazumder for sharing data about the Rosenwald schools. We are especially grateful to Patricia Barnes, Stephanie Robinson, and Deborah Rose at the National Center for Health Statistics for their assistance with the restricted-access National Health Interview Survey data. The findings and conclusions in this article are those of the authors and do not necessarily represent the views of the Research Data Center, the National Center for Health Statistics, or the Centers for Disease Control and Prevention.
Appendix
Table 5.
The influence of black-white differences in school quality on black-white differences in health measures
| Self-rated Health |
Body Mass Index |
Obesity | Ever Smoked | Currently Smoked |
Any Limitations | Mortality | |
|---|---|---|---|---|---|---|---|
| Pupil-Teacher Ratio | 0.000122 (0.00335) |
−0.00315 (0.0127) |
0.000404 (0.00132) |
−0.00388* (0.00182) |
−0.000112 (0.00167) |
0.00307* (0.00140) |
0.000671 (0.00219) |
| Observations | 462 | 462 | 462 | 462 | 462 | 462 | 462 |
| R2 | .459 | .830 | .675 | .359 | .331 | .283 | .373 |
| Teachers’ Wages | 4.92e-05 (4.14e-05) |
0.000315† (0.000178) |
2.61e-05† (1.25e-05) |
−3.21e-05 (3.28e-05) |
−4.17e-05 (3.27e-05) |
6.49e-08 (1.78e-05) |
−4.88e-05* (2.29e-05) |
| Observations | 462 | 462 | 462 | 462 | 462 | 462 | 462 |
| R2 | .461 | .831 | .677 | .356 | .337 | .276 | .391 |
| Term Length | −0.000422 (0.00130) |
0.00215 (0.00387) |
−7.91e-05 (0.000382) |
0.000595 (0.000829) |
−0.000780 (0.000618) |
−0.000889† (0.000467) |
−0.000776 (0.000632) |
| Observations | 462 | 462 | 462 | 462 | 462 | 462 | 462 |
| R2 | .459 | .830 | .675 | .354 | .334 | .281 | .378 |
Notes: Heteroskedasticity-robust standard errors that allow for clustering within state of birth are in parentheses.
Each coefficient estimate is based on a separate regression. Additional covariates that are not shown include the black-white differences in the infant mortality rate, average family size, and the average Duncan SEI occupational earnings score; cohort fixed effects; survey-year fixed effects; and state-of-birth fixed effects.
Sources: National Health Interview Survey 1984–2007; Card and Krueger (1992).
p < .10;
p < .05
Table 6.
The influence of black-white differences in school quality and exposure to Rosenwald schools on black-white differences in health
| Eq. (2) |
Eq. (2) + Exposure to Rosenwald Schools |
|
|---|---|---|
| Panel A: Self-rated Health | ||
| Black-white school quality | −0.00434 (0.0270) |
−0.00751 (0.02965) |
| Rosenwald schools | 0.00659 (0.00401) |
|
| R2 | .459 | .467 |
| Panel B: Body Mass Index | ||
| Black-white school quality | 0.0544 (0.0868) |
0.09448 (0.11489) |
| Rosenwald schools | 0.04026 (0.03201) |
|
| R2 | .830 | .839 |
| Panel C: Obesity | ||
| Black-white school quality | −0.00112 (0.00880) |
0.00245 (0.00956) |
| Rosenwald schools | 0.00323 (0.00197) |
|
| R2 | .675 | .698 |
| Panel D: Ever Smoked | ||
| Black-white school quality | 0.0197 (0.0164) |
0.01848 (0.01801) |
| Rosenwald schools | 0.00074 (0.00231) |
|
| R2 | .356 | .382 |
| Panel E: Currently Smoke | ||
| Black-white school quality | −0.0102 (0.0113) |
−0.00204 (0.01434) |
| Rosenwald schools | 0.00404 (0.00249) |
|
| R2 | .333 | .304 |
| Panel F: Any Limitations | ||
| Black-white school quality | −0.0208** (0.00873) |
−0.01801* (0.00786) |
| Rosenwald schools | 0.00747** (0.0013) |
|
| R2 | .282 | .296 |
| Panel G: Mortality | ||
| Black-white school quality | −0.0143 (0.0150) |
−0.01728 (0.01845) |
| Rosenwald schools | 0.00029 (0.00175) |
|
| R2 | .377 | .352 |
| Observations | 462 | 412 |
Notes: Heteroskedasticity-robust standard errors that allow for clustering within state of birth are in parentheses.
Additional covariates that are not shown include black-white differences in infant mortality rate, average family size, and the average Duncan SEI occupational earnings score; cohort fixed effects; survey-year fixed effects; and state-of-birth fixed effects. The variable measuring exposure to Rosenwald schools, which was first defined in Aaronson and Mazumder (2011), is the number of teachers in Rosenwald schools in the state multiplied by the average class size of 45 students and divided by the number of black school-aged individuals, which represents the likelihood that a black individual in a birth cohort in a state would have attended a Rosenwald school.
Sources: National Health Interview Survey 1984–2007; Aaronson and Mazumder (2011); Card and Krueger (1992).
p < .05;
p < .01
Footnotes
Many other explanations for the causes of racial differences have been explored, including physician discrimination (Balsa and McGuire 2003), the use of health care providers of differing quality (Baicker et al. 2005), the availability and type of insurance (Balsa et al. 2007; Currie et al. 2008), patient compliance with therapy (Simeonova 2008), medical knowledge (Aizer and Stroud 2010), residential segregation (Williams and Jackson 2005), and income (Williams and Jackson 2005).
As Donohue et al. (2002) noted, migration from urban to rural areas within the South explains little of the convergence in quality of black and white schools.
The Rosenwald Fund provided matching grants to build schools and required minimum standards for teachers’ wages and the length of the school year in order to receive funding (Donohue et al. 2002). Thus, the Fund required commitment from blacks in the local communities, which could reflect preferences for education. However, Aaronson and Mazumder (2011) found that the socioeconomic conditions of blacks were unrelated to the locations of Rosenwald schools. Because the Rosenwald Fund contributed to the building of new schools, the improved sanitation in these new schools could be correlated with the improvements in school quality for blacks during the 1920s. Although our primary measure of school quality was influenced by the Rosenwald Fund, this measure does not reflect the additional improvements in school quality specifically from the construction of new schools. To incorporate this additional component of school quality, we examine data, generously shared by Bhashkar Mazumder, on the construction of Rosenwald schools between 1919 and 1932. Because we do not have information on the total quantity of school buildings attended by white and black students, as opposed to just the number of Rosenwald schools, we add the average exposure to Rosenwald schools for black students for each state and for each cohort as a separate variable to the specification in Eq. (2). As shown in Table 6 in the appendix, we find that exposure to Rosenwald schools does not influence the primary result of the study, which is the influence of the convergence in school quality on racial differences in disability.
Cotton, which relied significantly on slave labor, was the primary crop in the states with relatively large black populations, while tobacco was the primary crop in states with relatively smaller black populations (Daniel 1985; Fogel and Engerman 1974; Wright 1986).
The emphasis on schooling and the decline in child labor was most pronounced among southern blacks, both in farm and nonfarm households (Tolnay 1999). For example, the percentage of black youths ages 10–14 and from southern farm households who were enrolled in school increased by 11 percentage points to 85 % between 1910 and 1940, while corresponding figures for white and northern black children remained constant (Tolnay 1999). The percentage of black adolescents in southern farm households who were working decreased by 37 percentage points to 43 % during this period; the decrease in child labor was most pronounced for females (Tolnay 1999). These trends reflected the changing labor market for blacks in the South: an increase in wage laborers instead of tenant farmers, an increase in agricultural productivity from technological advances, and an increase in off-farm employment (Tolnay 1999).
The desegregation of hospitals in the South in the 1960s improved access to medical care for blacks and decreased infant mortality (Almond et al. forthcoming). The integration of hospitals occurred very rapidly throughout the region because of the Civil Rights Act and the Medicare Act (Almond et al. forthcoming). Thus, variation in exposure to integrated hospitals is reflected in the cohort fixed effects.
The six excluded states are Alabama, Florida, Georgia, Louisiana, Mississippi, and North Carolina. The prevalence estimates, which were also used in Bleakley (2007) and reported by Kofoid and Tucker (1921), are based on a survey of U.S. Army recruits.
We also estimate a model using the specification described by Eq. (2) (not reported) in which black-white differences in family income is the outcome. Although our specification differs from Card and Krueger’s (1992), consistent with theirs, we find that a convergence in school quality results in a significant convergence in income.
The southern states in our sample are Alabama, Arkansas, Delaware, Florida, Georgia, Kentucky, Louisiana, Maryland, Mississippi, Missouri, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, Virginia, and West Virginia. The District of Columbia was also included; for simplicity, our references to “southern states” throughout the discussion of results also include the District of Columbia.
There are 18 states of birth, four birth cohort groups, four survey year groups, and two sexes, creating a potential total of 576 cells that would measure black-white differences. We excluded 109 cells with missing values for IMR, which we interpolated but did not extrapolate, and with fewer than 10 blacks and 10 whites. Of the 109 cells, 63 were cells with fewer than 10 blacks and 10 whites; and 60 cells had missing IMR values, 14 of which also had fewer than 10 blacks and 10 whites. Five additional cells did not have data because of the coverage of the NHIS. One of the states, Delaware, was nearly always excluded, contributing only four cells out of a potential 32 cells. Approximately three-quarters of the excluded cells are from the 1910–1919 birth cohorts.
The average number of days per school year could be viewed as a measure of the quantity of schooling; however, as noted earlier, we consider term length as a measure of school quality because the number of days per school year is a determinant of the amount of human capital gained within a year of completed schooling.
We thank David Card for providing the detailed data used to construct the 10-year averages published in Card and Krueger (1992), which include state averages for 1915 and biennially from 1918 to 1966.
Card and Krueger (1992) noted that the average teacher wages reported in the school quality data are nearly identical to the state- and race-specific average wages for teachers in the 1940, 1950, and 1960 censuses; however, the authors acknowledge the possibility of measurement error in these data, particularly in the early years. Because the school quality measures are assigned to individuals based on their years of schooling attended and then aggregated for each cohort in each state, the school quality measures are weighted averages of 20 years of school quality data, which reduces the influence of measurement error from a specific year. Related to measurement error concerns, the average pupil-teacher ratio is based on enrollment, instead of attendance, so that these reported statistics may not accurately reflect the number of students present in a classroom. As Card and Krueger (1996) and Heckman et al. (1996) noted, using state-level measures of school quality could reduce the attenuation bias from school-level measures of school quality that are potentially measured with error or that do not reflect the quality of schooling received throughout all years of schooling. Further, using state averages of school quality masks variation in school districts within states, which will lead to a downward bias in the estimated impact of school quality (Donohue et al. 2002).
The scoring coefficients for the summary measure of school quality indicate that term length receives the most weight (scoring coefficient = 0.45), followed by pupil-teacher ratio (scoring coefficient = –0.39), and teacher wages (scoring coefficient = 0.17). The “uniqueness” of the three individual school quality measures is 0.194 for pupil-teacher ratio, 0.396 for teacher wages, and 0.171 for term length, indicating that the summary factor measure explains most of the variance in all three individual school quality measures.
A complete set of the estimates for the specifications shown in each table is available in Online Resource 1.
Further supporting this claim are specifications that include an interaction term between the black-white difference in the proportion of the cell population that still lives in the South and the black-white difference in school quality.
We also investigate whether veteran’s status mediates the effects. However, the NHIS significantly changed its measure of veteran status in 1997, making it difficult to interpret an analysis similar to that using the other mediating variables. Nevertheless, we do not find evidence that veteran status mediates the effects that we observe.
We also investigated whether black-white differences in school quality were associated with aggregate mortality before we observed individuals in the NHIS data. Specifically, we used census data to look at death rates between 1960–1970 and 1970–1980 using the approach of Lleras-Muney (2005). We found no evidence that black-white differences in school quality were associated with black-white differences in mortality before we observed individuals in the NHIS data (results not shown), reducing concerns about selective mortality bias. On the other hand, it is interesting that differences in school quality are associated with disability but not with reductions in early mortality except when we exclude the oldest cohorts in the NHIS data. Possible explanations for this finding include measurement error in the calculation of death rates using successive censuses and advancements in medical care and medical technology that are relatively more likely to be used by individuals with greater education from higher-quality schools that extend longevity but do not reduce morbidity.
Contributor Information
David Frisvold, Emory University, Department of Economics, 1602 Fishburne Drive, Atlanta, GA 30322-2240, USA david.frisvold@emory.edu.
Ezra Golberstein, University of Minnesota, Division of Health Policy and Management, and Minnesota Population Center, 420 Delaware St. SE, MMC 729, Minneapolis, MN 55455, USA egolber@umn.edu.
References
- Aaronson D, Mazumder B. The impact of Rosenwald schools on black achievement. Journal of Political Economy. 2011;119:821–888. [Google Scholar]
- Aizer A, Stroud L. Education, knowledge and the evolution of disparities in health. National Bureau of Economic Research; Cambridge, MA: 2010. (NBER Working Paper No. 15840) [Google Scholar]
- Almond D, Chay K, Greenstone M. Civil rights, the war on poverty, and black-white convergence in infant mortality in the rural South and Mississippi. American Economic Review. (Forthcoming) [Google Scholar]
- Anderson JD. The education of blacks in the South, 1860–1935. The University of North Carolina Press; Chapel Hill: 1985. [Google Scholar]
- Ashenfelter O, Collins WJ, Yoon A. Evaluating the role of Brown v. Board of Education in school equalization, desegregation, and the income of African Americans. American Law and Economics Review. 2006;8:213–248. [Google Scholar]
- Baicker K, Chandra A, Skinner JS. Geographic variation in health care and the problem of measuring racial disparities. Perspectives in Biology and Medicine. 2005;48(Suppl.):S42–S53. [PubMed] [Google Scholar]
- Balsa AI, McGuire TG. Prejudice, clinical uncertainty and stereotyping as sources of health disparities. Journal of Health Economics. 2003;22:89–116. doi: 10.1016/s0167-6296(02)00098-x. [DOI] [PubMed] [Google Scholar]
- Balsa AI, Cao Z, McGuire TG. Does managed health care reduce health care disparities between minorities and whites? Journal of Health Economics. 2007;26:101–121. doi: 10.1016/j.jhealeco.2006.06.001. [DOI] [PubMed] [Google Scholar]
- Black DA, Sanders SG, Taylor EJ, Taylor LJ. The impact of the Great Migration on mortality of African Americans: Evidence from the Deep South. Paper presented at the conference “Education and Employment” at the Federal Reserve Bank of Atlanta; Sep 30, 2011. Retrieved from http://www.frbatlanta.org/documents/news/conferences/11employment_education_black. pdf. [Google Scholar]
- Bleakley H. Disease and development: Evidence from hookworm eradication in the American South. Quarterly Journal of Economics. 2007;122:73–117. doi: 10.1162/qjec.121.1.73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Card D, Krueger AB. School quality and black-white relative earnings: A direct assessment. Quarterly Journal of Economics. 1992;107:151–200. [Google Scholar]
- Card D, Krueger AB. Labor market effects of school quality: Theory and evidence. In: Burtless G, editor. Does money matter? The effect of school resources on student achievement and adult success. Brookings Institution Press; Washington, DC: 1996. pp. 97–140. [Google Scholar]
- Chay KY, Greenstone M. The impact of air pollution on infant mortality: Evidence from geographic variation in pollution shocks induced by a recession. Quarterly Journal of Economics. 2003;118:1121–1167. [Google Scholar]
- Clotfelter CT, Ladd HF, Vigdor J. Who teaches whom? Race and the distribution of novice teachers. Economics of Education Review. 2005;24:377–392. [Google Scholar]
- Cooper WJ, Terrill TE. The American South: A history. Vol. II. McGraw Hill, Inc.; New York: 1991. [Google Scholar]
- Currie J, Decker S, Lin W. Has public health insurance for older children reduced disparities in access to care and health outcomes? Journal of Health Economics. 2008;27:1567–1581. doi: 10.1016/j.jhealeco.2008.07.002. [DOI] [PubMed] [Google Scholar]
- Cutler D, Miller G. The role of public health improvements in health advances: The twentieth-century United States. Demography. 2005;42:1–22. doi: 10.1353/dem.2005.0002. [DOI] [PubMed] [Google Scholar]
- Culter D, Lleras-Muney A. Education and health: Evaluating theories and evidence. In: House J, Schoeni R, Kaplan G, Pollack H, editors. Making Americans healthier: Social and economic policy as health policy. Russell Sage Foundation; New York: 2008. pp. 29–60. [Google Scholar]
- Cutler D, Lleras-Muney A. Understanding differences in health behaviors by education. Journal of Health Economics. 2010;29:1–28. doi: 10.1016/j.jhealeco.2009.10.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Daniel P. Breaking the land: The transformation of cotton, tobacco, and rice cultures since 1880. University of Illinois Press; Urbana: 1985. [Google Scholar]
- de Walque D. Education, information, and smoking decisions: Evidence from smoking histories in the United States, 1940–2000. Journal of Human Resources. 2010;45:682–717. [Google Scholar]
- Donohue JJ, Heckman JJ, Todd PE. The schooling of Southern blacks: The roles of legal activism and private philanthropy, 1910–1960. Quarterly Journal of Economics. 2002;117:225–268. [Google Scholar]
- Fishback PV, Haines MR, Kantor S. The impact of the New Deal on black and white infant mortality in the South. Explorations in Economic History. 2001;38:93–122. [Google Scholar]
- Fletcher J, Frisvold D. Higher education and health investments: Does more schooling affect preventive care use? Journal of Human Capital. 2009;3:144–176. doi: 10.1086/645090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fogel RW, Engerman SL. Time on the cross: The economics of American Negro slavery. Little, Brown and Company; Boston, MA: 1974. [Google Scholar]
- Frisvold D, Golberstein E. School quality and the education-health relationship: Evidence from blacks in segregated schools. Journal of Health Economics. 2011;30:1232–1245. doi: 10.1016/j.jhealeco.2011.08.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glied S, Lleras-Muney A. Technological innovation and inequality in health. Demography. 2008;45:741–761. doi: 10.1353/dem.0.0017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grossman M. On the concept of health capital and the demand for health. Journal of Political Economy. 1972;80:223–255. [Google Scholar]
- Guralnik JM, Land KC, Blazer D, Fillenbaum GG, Branch LG. Educational status and active life expectancy among older blacks and whites. New England Journal of Medicine. 1993;329:110–116. doi: 10.1056/NEJM199307083290208. [DOI] [PubMed] [Google Scholar]
- Heckman JJ, Layne-Farrar A, Todd P. Human capital pricing equations with an application to estimating the effect of schooling quality on earnings. Review of Economics and Statistics. 1996;78:562–610. [Google Scholar]
- Humphreys M. How four once common diseases were eliminated from the American South. Health Affairs. 2009;28:1734–1744. doi: 10.1377/hlthaff.28.6.1734. [DOI] [PubMed] [Google Scholar]
- Johnson R. Long-run impacts of school desegregation and school quality on adult attainments. National Bureau of Economic Research; Cambridge, MA: 2010. (NBER Working Paper No. 16664) [Google Scholar]
- Kofoid CA, Tucker JP. On the relationship of infection by hookworm to the incidence of morbidity and mortality in 22,842 men of the United States Army. American Journal of Hygiene. 1921;1:79–117. [Google Scholar]
- Levine RS, Foster JE, Fullilove RE, Fullilove MT, Briggs NC, Hull PC, Hennekens CH. Black-white inequalities in mortality and life expectancy, 1933–1999: Implications for Healthy People 2010. Public Health Reports. 2001;116:474–483. doi: 10.1093/phr/116.5.474. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lleras-Muney A. The relationship between education and adult mortality in the United States. Review of Economic Studies. 2005;72:189–221. [Google Scholar]
- Lochner L. Non-production benefits of education: Crime, health, and good citizenship. National Bureau of Economic Research; Cambridge, MA: 2011. (NBER Working Paper No. 16722) [Google Scholar]
- Margo RA. Race and schooling in the South, 1880–1950: An economic history. University of Chicago Press; Chicago, IL: 1990. [Google Scholar]
- Mazumder B. How did schooling laws improve long-term health and lower mortality? Federal Reserve Bank of Chicago; Chicago, IL: 2007. (Working Paper 2006-23) [Google Scholar]
- Meer J, Miller D, Rosen HS. Exploring the health-wealth nexus. Journal of Health Economics. 2003;22:713–730. doi: 10.1016/S0167-6296(03)00059-6. [DOI] [PubMed] [Google Scholar]
- Rice MF, Jones W., Jr. Public policy and the black hospital: From slavery to segregation to integration. Greenwood Press; Westport, CT: 1994. [Google Scholar]
- Ross CE, Mirowsky J. Refining the association between education and health: The effects of quantity, credential, and selectivity. Demography. 1999;36:445–460. [PubMed] [Google Scholar]
- Ross CE, Wu C. The links between education and health. American Sociological Review. 1995;60:719–745. [Google Scholar]
- Ruggles SJ, Alexander T, Genadek K, Goeken R, Schroeder M, Sobek M. Integrated Public Use Microdata Series: Version 5.0 [Machine-readable database] University of Minnesota; Minneapolis: 2010. [Google Scholar]
- Simeonova E. Doctors, patients, and the racial mortality gap: What are the causes? Department of Economics, Columbia University; New York: 2008. (Discussion Paper 0708-13) [Google Scholar]
- Smith J. Healthy bodies and thick wallets: The dual relation between health and economic status. Journal of Economic Perspectives. 1999;13:145–166. [PMC free article] [PubMed] [Google Scholar]
- Tolnay SE. Educational selection in the migration of Southern Blacks, 1880–1990. Social Forces. 1998;77:487–514. [Google Scholar]
- Tolnay SE. The bottom rung: African American family life on Southern farms. University of Illinois Press; Chicago: 1999. [Google Scholar]
- Troesken W. The limits of Jim Crow: Race and the provision of water and sewerage services in American cities, 1880–1925. The Journal of Economic History. 2002;62:734–772. [Google Scholar]
- U.S. Department of Health and Human Services . Healthy People 2010: Understanding and improving health. 2nd ed U.S. Government Printing Office; Washington, DC: 2000. [Google Scholar]
- Williams DR, Jackson PB. Social sources of racial disparities in health. Health Affairs. 2005;24:325–334. doi: 10.1377/hlthaff.24.2.325. [DOI] [PubMed] [Google Scholar]
- Wright G. Old South, new South: Revolutions in the Southern economy since the Civil War. Louisiana State University Press; Baton Rouge: 1986. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.