

Abstract
Background:
The most common technique to anesthetize mandibular primary teeth is inferior alveolar (I.A) nerve block injection which induces a relatively sustained anesthesia and in turn may potentially traumatize soft-tissues. Therefore, the need of having an alternative technique of anesthesia with a shorter term but the same efficacy is reasonable. The aim of this study was a comparison of the efficacy of two anesthetic techniques of mandibular primary first molar.
Materials and Methods:
In this randomized crossover clinical trial, 40 children with ages ranged from 5 years to 8 years whose mandibular primary first molars were eligible for pulpotomy, were selected and divided randomly into two groups. The right and left mandibular first molars of group A were anesthetized with infiltration and I. A nerve block techniques in the first and second sessions respectively. The left and right mandibular first molars of group B were anesthetized with I.A nerve block and infiltration techniques in the first and second sessions respectively. The severity of pain were measured and recorded according to sound-eye-motor scale by a certain person. Data was analyzed using Wilcoxon Signed Rank and Mann-Whitney U tests (P > 0.05).
Results:
The severity of pain was lower in infiltration technique versus I.A nerve block. There were no significant differences between the severities of pain on pulpal exposure of two techniques.
Conclusion:
It seems that infiltration technique is more favorable to anesthetize the mandibular primary first molar compared to I.A nerve block.
Keywords: Anesthetics, local/administration, nerve block/methods, pain measurement, pulpotomy/methods
INTRODUCTION
One of the most important ways to manage the behavior of children is pain control. Since a deep anesthesia is necessary in all dental treatments, a comfortable injection with minimal pain and no injury has a considerable importance. In fact, a local anesthesia induced by a single injection not only provides the patient's comfort and decreases pain but also increases patient's trust to dentist.[1]
The most common method of inducing anesthesia for maxilla is infiltration or supra-periosteal injection technique.[2] In this method, needle is penetrated in deep vestibular mucosa above the apex of the tooth. Inferior alveolar (I.A) nerve block is the common technique of anesthetizing the mandible. The technique of block injection for adults and children is almost similar. The only difference is that the injection must be a little lower, and more posteriorly for children because the mandibular foramen is lower to occlusal surface of deciduous teeth.[2] One of the most common complaints following I.A nerve block is soft-tissue injury due to biting lips, tongue, and buccal mucosa. Therefore, the necessity of an alternative method is felt.[3,4] Today I.A nerve block is commonly used to treat the pulp of mandibular primary molar teeth.[2] Block injection for hemophilic patients who have not received recombinant factor may lead to cervical hematoma or even death. In these patients, infiltration may be used.[5] Infiltration technique because of direct vision of practitioner on it, less depth penetration of needle, less technical errors, less amounts of anesthetic solution, easier application, limited anesthesia of soft-tissues outside the operation field and shorter duration of being anesthetized might be used as an alternative to block. On the other hand because the anesthetized area is limited, bilateral anesthesia is possible.[6,7,8]
Sharaf selected pediatric patients who needed bilateral multiple dental treatments (amalgam filling, pulpotomy and tooth extraction). The researcher compared the effectiveness of infiltration to block techniques. Results showed that infiltration is an appropriate technique to anesthetize primary mandibular first molar for pulpotomy.[3]
Donohue et al. showed that anesthetizing primary mandibular molar region for tooth filling, pulpotomy and extraction with infiltration technique is possible.[9]
Jones et al. in a study on 308 patients concluded that block injection is significantly more painful than infiltration.[10]
Ram and Peretz evaluated the patients responses to pain during block and infiltration injections; they showed that children responded more severely in the form of crying to mandibular block injection.[11]
In a study by Oulis et al. it was shown that sufficiency of infiltration technique for mandibular tooth extraction and pulpotomy was less than a block.[12]
Aminabadi et al. by evaluating the relation between the site of injection and pain in 5-6 year old children showed that the most severe response was related to nasopalatine nerve block and the least was to posterior superior and I.A nerves block, and also maxillary injections, in general, was more painful than mandibular injections.[13]
Jung et al. evaluated the efficacy of block and infiltration injections anesthetizing mandibular first molars. They assessed tooth sensitivity by pulp tester at the end of 5, 8, 11, 15, 20, 25, and 30 min following injecting Articaine 4%. The results of their study showed the faster appearance of anesthesia with infiltration injection compared to block while the efficacy was identical.[14]
To assess the behavior and comprehensive response of a child to the dental office environment, it must be considered that what response is appropriate for his/her age. Therefore, suitable tests and certain methods have to be applied.[15] In the present study, the degree of pain during injection and on pulpal exposure of the two mandibular anesthetizing methods were assessed and compared. To assess the pain, sound-eye-motor (SEM) scale was used which is valid and easy to apply.[3]
MATERIALS AND METHODS
The protocol of this clinical trial was registered (IRCT201009084714N1) at the clinical trial administration office Research Vice Chancellor of Ministry of Health of Iran. The study was approved by the school of Dentistry Ethics committee at the Isfahan University of Medical Sciences, Iran. Among the patients referred to Isfahan specialized clinics for dental pediatric procedures, 40 pediatric patients candidate for bilateral pulpotomy of mandibular primary first molars were selected. Inclusion criteria were general health, lack of painful illness, able to be placed in the grades + or ++ of Frankl behavioral scale. According to this rating scale, grade + is referred to the children who negotiate first but accept dental treatment; grade (++) is referred to those who have a good relation with the dentist and are interested in dentistry with laughing and enjoying.17
In this crossover study, the patients were placed randomly into the groups A and B. On the first session, the children in the group A received infiltration for mandibular right first molar and in group B I.A nerve block for the left side.
On the second session, all the patients of group A received I.A nerve block on the left side and all patients of group B received infiltration technique on the right side. Thus, both infiltration and block techniques were performed for all patients separately.
All patients received lidocaine hydrochloride anesthetic (Darupakhsh, Tehran, Iran) using 27 gage needles (Supa, Tehran, Iran).
The sites of injection were anesthetized with topical benzocaine gel before injection. The duration of application of gel was 1 minute. Dental treatments were started 10 min after injection. All the injections were performed by an academic pedodontist.
Infiltration injection with the volume of 0.2 ml of lidocaine 2% was done at the depth of buccal vestibule between the roots of teeth. I.A nerve block injection was performed with the volume of 1 ml of lidocaine 2% in a standard manner at mandibular jaw.
The amount of pain was measured through patient's expressions, behaviors, or biologic markers. Vocal expressions, facial mimics and body movements are related to pain SEM. One of the valid indices to assess the pain is SEM scale, which is accepted to assess the comfort or existence of pain in children.[3] By reading the table of this four score scale for the recorded eye and body movements and also voice, the severity of child's pain was evaluated. For example, a child whose voice was the lack of the sign of pain earned grade 1, or would earn grade 4 if he/she was crying. Since all the variables of SEM scale are qualitative and also are not distributed normally, the non-parametric tests were used to analyze and compare the grade of variables. The amount of pain during injection and on pulpotomy was assessed using this scale and recorded by a calibrated and trained dentist who was blind. Then data were analyzed. Mann-Whitny test was used to compare the grades of SEM scale for different techniques in two groups independently, and Wilcoxon Signed Rank tests for each group and the total of patients. All the differences were considered significant at the level of P > 0.05.
RESULTS
The range and mean value of patients age were 5-8 and 6.25 years respectively. Eighteen out of 40 patients (45%) earned + and 22 (55%) ++ for cooperation.
The scores of SEM during injection and on pulpal exposure for infiltration technique and also I.A nerve block technique are summarized in Tables 1 and 2 respectively.
Table 1.
Efficacy of infiltration technique, SEM scores during injection and pulpal exposure
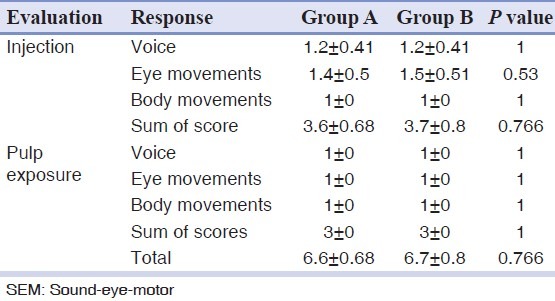
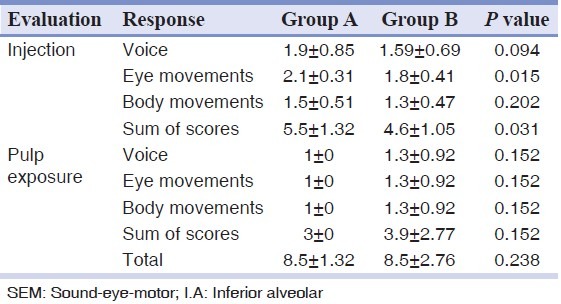
Table 2.
Efficacy of I.A nerve block technique, SEM scores during injection and on pulpal exposure
No significant differences were found between the scores of injections and also pulpal exposure of two groups when infiltration technique was applied (P = 0.766)
Comparing the results only showed a significant difference between two groups regarding eye movements and also the sum of SEM scores during injection. Thus in group B, which received block injection first, score of eye movements during block injection was higher. However, comparing the efficacy of block induced anesthesia between two groups did not show significant differences. The SEM score of infiltration injection was significantly lower than a block in both groups regardless the order of injections but was not significant on pulpal exposure.
The results of two techniques are compared in Table 3.
Table 3.
Comparison between the SEM scores of two different techniques in groups A and B
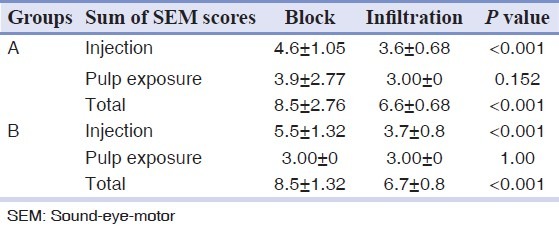
The scores of SEM in infiltration technique were significantly lower than block. Therefore, infiltration technique is more acceptable for children.
No significant difference was seen between block and infiltration induced anesthesia on pulpal exposure (P = 0.917)
DISCUSSION
In this study, the efficacy of infiltration and I.A nerve block induced anesthesia to perform mandibular primary first molars pulpotomy were compared. Since injection is known as a stressful phase in pediatric dentistry, well controlled pain during injection is an important effective factor in getting the cooperation of the child. Thus, the dentist who can perform an injection with minimum pain, stress, and anxiety is more successful. The most common technique for mandibular anesthetic injection in children is I.A nerve block. Considering that block injection induces relatively sustained anesthesia and may also cause soft-tissue traumatic injuries, the necessity of an alternative technique is felt.[3,4]
According to this study infiltration technique caused less pain during injection than block. This finding is consistent with the results of Sharaf,[3] Jones et al.,[10] and Ram and Peretz.[11]
In the study of Sharaf[3] with the use of SEM scale, it was revealed that block injection, especially in 3-7 year old children, was more painful than infiltration technique and caused negative behaviors. Jones et al.[10] although studied on a wider range of age (3-16) and used VAS scale to evaluate the severity of pain, but showed that block injection was more painful than infiltration technique.
The present study showed no significant difference between the efficacy of block and infiltration induced anesthesia during injection and on pulpotomy.
In the studies of Sharaf[3] and Donohue et al.[9] who used lidocaine, although the 3-9 year old children were evaluated the same results were demonstrated. Jung et al.[14] used Articaine 4% and tested the sensitivity of teeth by a pulp tester and reached the same results as the present study.
They revealed that the appearance of anesthesia in infiltration technique is earlier with the same efficacy.
The results of Oulis et al.[12] were different, although the efficacy of two techniques for restorative treatments of mandibular primary teeth was similar, but block technique was more efficient for pulpotomy. The difference between the results of theirs and present studies might be related to the difference in type of teeth. Their study was on mandibular first and second primary molar teeth while this study was on mandibular first primary molar.
CONCLUSION
Since block injection induces sustained anesthesia that is potentially traumatic to soft-tissues, it seems that infiltration anesthesia could be used as a suitable alternative technique for mandibular primary first molar pulpotomy. This technique is easier and induces moderate soft-tissue anesthesia.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Mcdonald RE, Avery DR. Dentistry for the Child and Adolescent.9 th ed. 9th ed. St Louis: Mosby Co; 2011. pp. 241–2. [Google Scholar]
- 2.Pinkham JR, Casamassimo PS, McTigue DJ, Fields HW, Nowak AJ. Pediatric Dentistry: Infancy Through Adolescence. 4th ed. St Louis: Elsevier; 2005. pp. 450–3. [Google Scholar]
- 3.Sharaf AA. Evaluation of mandibular infiltration versus block anesthesia in pediatric dentistry. ASDC J Dent Child. 1997;64:276–81. [PubMed] [Google Scholar]
- 4.Gbotolorun OM, Olojede AC, Afolabi-Bello M, Arotiba GT. Knowledge and practice of alternatives to the conventional inferior dental block amongst dentists in Lagos. Nig Q J Hosp Med. 2010;20:228–30. [PubMed] [Google Scholar]
- 5.Kumar JN, Kumar RA, Varadarajan R, Sharma N. Specialty dentistry for the hemophiliac: Is there a protocol in place? Indian J Dent Res. 2007;18:48–54. doi: 10.4103/0970-9290.32419. [DOI] [PubMed] [Google Scholar]
- 6.Malamed SF. The periodontal ligament (PDL) injection: An alternative to inferior alveolar nerve block. Oral Surg Oral Med Oral Pathol. 1982;53:117–21. doi: 10.1016/0030-4220(82)90273-0. [DOI] [PubMed] [Google Scholar]
- 7.Brännström M, Nordenvall KJ, Hedström KG. Periodontal tissue changes after intraligamentary anesthesia. ASDC J Dent Child. 1982;49:417–23. [PubMed] [Google Scholar]
- 8.Meechan JG. The use of the mandibular infiltration anesthetic technique in adults. J Am Dent Assoc. 2011;142(Suppl 3):19S–24. doi: 10.14219/jada.archive.2011.0343. [DOI] [PubMed] [Google Scholar]
- 9.Donohue D, Garcia-Godoy F, King DL, Barnwell GM. Evaluation of mandibular infiltration versus block anesthesia in pediatric dentistry. ASDC J Dent Child. 1993;60:104–6. [PubMed] [Google Scholar]
- 10.Jones CM, Heidmann J, Gerrish AC. Children's ratings of dental injection and treatment pain, and the influence of the time taken to administer the injection. Int J Paediatr Dent. 1995;5:81–5. doi: 10.1111/j.1365-263x.1995.tb00169.x. [DOI] [PubMed] [Google Scholar]
- 11.Ram D, Peretz B. Reactions of children to maxillary infiltration and mandibular block injections. Pediatr Dent. 2001;23:343–6. [PubMed] [Google Scholar]
- 12.Oulis CJ, Vadiakas GP, Vasilopoulou A. The effectiveness of mandibular infiltration compared to mandibular block anesthesia in treating primary molars in children. Pediatr Dent. 1996;18:301–5. [PubMed] [Google Scholar]
- 13.Aminabadi NA, Farahani RM, Oskouei SG. Site-specificity of pain sensitivity to intraoral anesthetic injections in children. J Oral Sci. 2009;51:239–43. doi: 10.2334/josnusd.51.239. [DOI] [PubMed] [Google Scholar]
- 14.Jung IY, Kim JH, Kim ES, Lee CY, Lee SJ. An evaluation of buccal infiltrations and inferior alveolar nerve blocks in pulpal anesthesia for mandibular first molars. J Endod. 2008;34:11–3. doi: 10.1016/j.joen.2007.09.006. [DOI] [PubMed] [Google Scholar]
- 15.Pinkham JR, Casamassimo PS, McTigue DJ, Fields HW, Nowak AJ. Pediatric Dentistry: infancy Through Adolescence. 4th ed. St Louis: Elsevier; 2005. pp. 102–3. [Google Scholar]