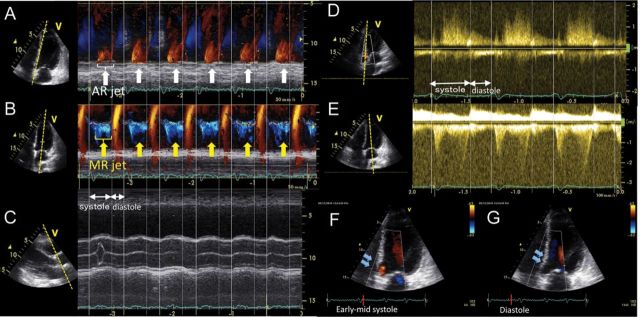
A 78-year-old male underwent continuous flow left ventricular assist device (LVAD) implantation due to ischaemic cardiomyopathy as a destination therapy. Routine echocardiogram performed 6 days after the surgery showed ‘systolic-phase’ aortic regurgitation (AR); the timing of regurgitation jet starting at the mid-systolic phase and ending at the early diastolic phase [Panel A, the colour Doppler M mode at the aortic valve (AV), white arrow]. The AR occurred slightly after the onset of mitral regurgitation (MR) (Panel B, the colour Doppler M mode at the mitral valve, yellow arrows), and both MR and AR timings were consistent with the systolic phase (See Supplementary data online, Videos S1 and S2). No remarkable AR jet was documented during the diastolic phase. The AV was mostly closed throughout the cycles, which opens once every 8–10 beats (Panel C). The mean pressure gradients of the trans-AV and trans-mitral valve based on the continuous wave Doppler measurements of AR (Panel D) and MR flow (Panel E) were 3.7 mmHg and 24.3 mmHg, respectively. The morphology of AV annulus changes through the cycles irrespective of the AV opening, with the AV annulus abnormally distorted and dilated during early mid-systole (Panel F), whereas the septum wall as well as the AV annulus edge slightly pushed towards the left ventricle during diastole (Panel G). The morphological change of the AV annulus during the systolic phase under LVAD support may result in impaired co-aptation of AV leaflets leading systolic-phase-limited AR in this patient. Imbalanced contraction between left and right ventricles under LVAD support may affect the abnormal distortion of AV annulus during systole.
Supplementary data are available at European Heart Journal – Cardiovascular Imaging online.