

Abstract
Objectives.
Drawing upon a vulnerability model, this study tested whether low educational level would amplify the negative contribution of risky personality traits, such as high neuroticism and low conscientiousness, on older adults physical functioning.
Method.
Five hundred and thirteen French-speaking community-dwelling older adults aged 60–91 years (mean age = 66.37, SD = 5.32) completed measures of physical functioning, education, personality traits, chronic conditions, and demographic variables.
Results.
Results revealed that extraversion and conscientiousness were positively associated with physical functioning, whereas neuroticism was a negative predictor, beyond demographics, chronic conditions, and education. The negative relationship between neuroticism and physical functioning was stronger among individuals with low educational level and was nonsignificant among older people with higher level of education.
Discussion.
This study is the first to support a vulnerability model, which entails an amplification of neuroticism risk at low education, but a diminishment of neuroticism risk for activity limitations at high education. As a whole, it appears that a focus on either personality or education without taking into account each other provides only a partial account of the predictors of basic daily physical activities in old age.
Key Words: Aging, Education, Personality, Physical functioning.
Given that maintenance of physical functioning—such as walking, standing, climbing stairs, and other mobility-related activities of daily life—is a crucial component of older individuals’ quality of life, the identification of its predictors deserves particular attention. Beyond the deleterious effect of chronic conditions and disease, attention have been directed toward socioeconomic status (SES), indexed by level of educational attainment, with studies having found that a high level of education is related to better physical function, whereas controlling for objective health conditions (Sulander et al., 2006). Better health decision making, greater access to material and medical resources, as well as regular involvement in health preventive behavior, and less frequent risky behavior explain in part these educational differences (Chapman, Fiscella, Duberstein, & Kawachi, 2009).
However, considering education without sufficient attention to personality traits paints an incomplete picture of the correlates of older adults’ physical functioning. Among the traits defined by the Five-Factor Model (Digman, 1990), high neuroticism and low conscientiousness are risk factors for activity limitations in old age (Duberstein et al., 2003; Suchy, Williams, Kraybill, Franchow, & Butner, 2010), which may be explained by their consistent relationships with health-damaging behaviors (Rhodes & Smith, 2006; Terracciano, Löckenhoff, Zonderman, Ferrucci, & Costa, 2008). Conversely, higher extraversion and conscientiousness predict better physical function among older adults (Chapman, Duberstein, & Lyness, 2007; Duberstein et al., 2003), possibly through health-promoting behavior (Rhodes & Smith, 2006). Although less consistent, there is also evidence that openness to experience is related to lower likelihood of physical limitations in old age (Duberstein et al., 2003), and there is a trend toward a positive relationship between agreeableness and independent activities of daily living (Suchy et al., 2010).
To date, the extent to which both individuals’ personality traits and educational attainment may work in conjunction to predict older adults’ basic daily physical activities has been somewhat underdeveloped. The potential interaction between personality traits and education for the prediction of physical functioning among older adults is suggested by the vulnerability model (Chapman et al., 2009; Chapman, Roberts, & Duberstein, 2011; Kivimaki et al., 2003). According to this model, socioeconomic disadvantage engenders more health problems among individuals with vulnerable personality configurations. For example, in a nationally representative sample, Chapman et al. (2009) found that low education amplifies the risk of smoking associated with low conscientiousness. Therefore, the vulnerability model suggests that low educational attainment may amplify the risk of lower physical functioning associated with risky personality traits such as high neuroticism and low conscientiousness. Less educated individuals may have lower health decision-making skills and limited access to health information and to material and medical resources—conditions that encourage impact of maladaptive personality traits on physical functioning. In addition, lower education may involve sociocultural norms more permissive of health-damaging behavior, such as smoking or physical inactivity—conditions in which the maladaptive coping characteristic of high neuroticism and low conscientiousness may be particularly likely to express itself through health risk behaviors increasing the risk of activity limitations of older adults.
Drawing upon the vulnerability model, the aim of this study was to test whether personality may interact with educational attainment to predict physical functioning. In line with the tenets of this model and prior research, it was expected that low educational level would amplify the negative contribution of risky personality traits, such as high neuroticism and low conscientiousness, to older adults’ physical functioning.
Method
Participants and Procedure
Participants were recruited throughout France using print advertisements in nonprofit organization newsletters, occupational settings, and clubs. To be eligible, they had to be at least 60 years old, living independently in the community, and free from severe mental or cognitive impairment. Six hundred and forty two individuals agreed to participate. The final sample consisted of 513 French-speaking community-dwelling individuals aged 60–91 years (mean age = 66.37, SD = 5.32; 65% women, 75% had a partner), who provided complete data on the variables of interest. Average years of education were 13.59 (SD = 3.24, range: 0–19 years).
Measures
Covariates.—
Age (in years), gender (coded as 0 for women and 1 for men), and marital status (coded as 0 for living with a partner and 1 for living alone) were included in the this study. Participants were also asked to report whether they currently suffered from any particular disease or conditions diagnosed by a physician in a preestablished list of common age-related conditions. The total number of diseases was computed, with higher scores indicating more health conditions.
Education.—
The level of education was operationalized as the total number of years of formal schooling.
Personality Traits.—
Personality traits were evaluated with the French version of the Big Five Inventory (Plaisant, Courtois, Réveillère, Mendelsohn, & John, 2010) initially developed by John, Donahue, and Kentle (1991). Participants rated their agreement on 45 self-descriptive easy-to-understand statements that assess the five personality traits of neuroticism, conscientiousness, extraversion, openness to experience, and agreeableness. Each item was rated on a 5-point Likert scale ranging from 1 “strongly disagree” to 5 “strongly agree.” In this study, Cronbach’s alpha for the five factors ranged from 0.74 to 0.84.
Physical Functioning.—
The physical functioning subscale of the French version of the SF-36 survey (Ware & Sherbourne, 1992) was used in this study. Participants were asked to answer 10 questions, which capture the extent to which the participants’ health level limits them in doing different activities (e.g., lifting or carrying groceries, climbing several flights of stairs), using a 3-point scale from 1 “limited a lot” to 3 “not limited at all.” Answers were averaged and were transformed so that the lowest possible score was 0 and the highest possible score was 100, indicating higher levels of functioning (= 0.85).
Data Analysis
A multiple regression analysis was computed to test for an interaction between personality and education in the prediction of physical functioning. Gender, age, marital status, and number of conditions were entered in the first step; education was entered in the second step; personality traits were added in the third step; and the personality by age interactions were entered in the fourth step. We ran collinearity diagnostics, and they revealed no problems with multicollinearity. When significant interactions emerged, the simple slopes for the association between the predictor and physical functioning at three levels of education, that is, average (the mean of the sample), lower education (1 SD below the mean), and higher education (1 SD above the mean), were plotted and tested for significance (see Aiken & West, 1991). Continuous variables were mean centered before running the analyses.
Results
Descriptive statistics and Pearson correlation coefficients among the variables of interest are presented in Table 1. Regression analysis revealed a significant contribution of gender ( β = 0.12, p < .01), age ( β = −0.28, p < .001), and number of conditions ( β = −0.36, p < .001) on physical functioning in the first step (R² = .27). In the second step, education significantly contributed to physical functioning ( β = 0.08, p < .05, ΔR² = .01, p < .05), whereas controlling for gender, age, and number of conditions. In the third step, extraversion ( β = 0.11, p < .01), neuroticism ( β = −0.12, p < .01), and conscientiousness ( β = 0.12, p < .01) added a significant amount of variance (ΔR² = .06, p < .001). In the final step, a significant interaction between education and neuroticism emerged ( β = 0.11, p < .01, ΔR² = .02, p < .05). The final equation was significant F(15, 497) = 19.05, p < .001, R² = .36 (see Table 2). Although no relationship between neuroticism and physical activity limitations emerged among older people with higher level of education, b = 0.04, t(497) = 0.04, ns, neuroticism was negatively related to physical functioning, for average, b = −1.86, t(497) = −2.56, p < .05, and low level of education, b = −3.76, t(497) = −3.75, p < .001 (see Figure 1).
Table 1.
Means (M), Standard Deviations (SD), and Correlations for the Variables Under Study (N = 513)
| Variables | M/% | SD | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|---|---|
| 1. Gender (% female) | 65 | — | — | |||||
| 2. Marital status (% living with a partner) | 75 | — | −.23*** | — | ||||
| 3. Age | 66.37 | 5.32 | .00 | .16*** | — | |||
| 4. Education | 13.59 | 3.24 | .13** | −.09* | −.12** | — | ||
| 5. Number of conditions | 1.25 | 1.32 | .02 | .05 | .23*** | −.13** | — | |
| 6. Physical functioning | 87.88 | 14.32 | .12** | −.11* | −.37*** | .18*** | −.42*** | — |
| 7. Extraversion | 3.03 | 0.75 | −.03 | −.05 | −.01 | −.00 | .03 | .15*** |
| 8. Neuroticism | 2.69 | 0.84 | −.14** | .07 | −.08 | −.13** | .08 | −.21*** |
| 9. Openness to experience | 3.46 | 0.64 | .06 | .00 | −.02 | .23*** | −.04 | .12** |
| 10. Agreeableness | 4.07 | 0.51 | −.17*** | .03 | .08 | −.01 | −.01 | .05 |
| 11. Conscientiousness | 3.91 | 0.60 | −.12** | −.05 | −.11* | .09* | −.04 | .20*** |
Note. * p < .05. ** p < .01. *** p < .001.
Table 2.
Summary of Regression Analysis Predicting Physical Functioning (N = 513)
| Variables | Step 1 | Step 2 | Step 3 | Step 4 | ||||
|---|---|---|---|---|---|---|---|---|
| B (β) | SEB | B (β) | SEB | B (β) | SEB | B (β) | SEB | |
| Age | −0.77(−.28)*** | 0.10 | −0.75(−.28)*** | 0.10 | −0.76(−.28)*** | 0.10 | −0.75(−.28)*** | 0.10 |
| Gender | 3.79(.12)** | 1.16 | 3.48(.11)** | 1.17 | 3.92(.13)*** | 1.18 | 4.23(.14)*** | 1.18 |
| Marital status | −0.65(−.02) | 1.31 | −0.52(−.01) | 1.30 | 0.24(.00) | 1.26 | 0.69(.02) | 1.26 |
| Number of conditions | −3.91(−.36)*** | 0.42 | −3.81(−.35)*** | 0.42 | −3.72(−.34)*** | 0.40 | −3.54(−.32)*** | 0.40 |
| Education | . | 0.37(.08)* | 0.17 | 0.27(.06) | 0.17 | 0.26(.06) | 0.17 | |
| Extraversion | . | 2.02(.11)** | 0.76 | 2.30(.12)** | 0.77 | |||
| Neuroticism | −2.08(−.12)** | 0.72 | −1.86(−.11)** | 0.72 | ||||
| Openness to experience | −0.41(−.01) | 0.89 | −.56(−.02) | 0.89 | ||||
| Agreeableness | 0.63(.02) | 1.12 | .92(.03) | 1.13 | ||||
| Conscientiousness | 3.00(.12)** | 0.92 | 3.44(.14)** | 0.93 | ||||
| Extraversion × education | .03(.00) | 0.25 | ||||||
| Neuroticism × education | .58(.11)** | 0.22 | ||||||
| Openness × education | −.30(−.04) | 0.27 | ||||||
| Agreeableness × education | −.17(−.02) | 0.36 | ||||||
| Conscientiousness × education | .36(.05) | 0.28 | ||||||
| R² | .27 | .28 | .34 | .36 | ||||
Note. Coefficients in parentheses are standardized coefficients. SE = standard error.
* p < .05. ** p < .01. *** p < .001.
Figure 1.
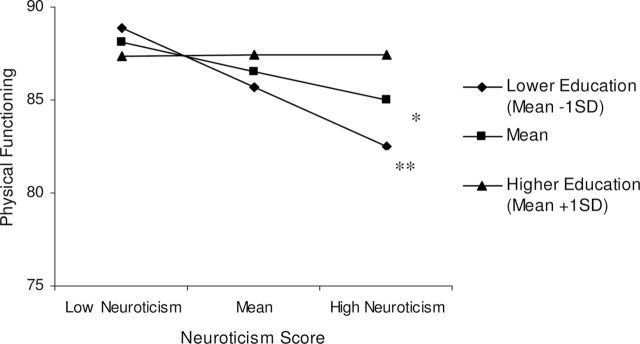
Interaction between neuroticism and education for the prediction of physical functioning. *p < .05 and **p < .001.
Discussion
The results partially confirm our hypothesis and revealed that the negative relationship between neuroticism and physical functioning is stronger among individuals with an educational level less than a high school diploma. This finding suggests that low education could amplify the risk of activity limitations resulting from individuals’ proneness to distress and anxiety, which supports the vulnerability model for the prediction of older people’s physical functioning. Education is a marker of one’s socioeconomic stratum, and different strata present different cultural norms and environmental constraints for healthy behavior. For instance, the burden of having to work long hours or at menial jobs may limit time and energy for exercise and healthy diet; in turn, more of one’s peers exhibit unhealthy behavior, engendering permissive social norms for such behavior. Such circumstances provide an environment in which unhealthy behavior as a coping response to distress (neuroticism) is likely to flourish. Over a lifetime, the cumulative impact on physical functioning in older age may be substantial. Conversely, an original result concerns the fact that high education, that is, over a bachelor’ degree, mitigates the risk of limitations in basic daily physical activities associated with neuroticism. The tendency of these individuals to adopt risky behavior may be counterbalanced by their higher educational level because they may have lived a lifetime in environmental scaffolding that discourages or minimizes the impact of poor health habits—for instance, encouraging healthy diet and physical activity, and frequent utilization of medical care. Thus, the vulnerability model also involves a protective element in which a higher level of education may ameliorate the risk associated with neuroticism.
Contrary to our hypothesis, the contribution of conscientiousness on physical functioning was independent of education. Our hypothesis was based on the increased smoking risk associated with low conscientiousness among less educated individuals previously noted (Chapman et al., 2009). The interaction we observed was in the same direction but not statistically significant. Because smoking and physical functioning are different outcomes, one result was in a general U.S. population of more than 2,000 and the other was an older French sample of around 500 persons, and different measures of conscientiousness were used, one might not expect rejection of the null. Possibly low education may interact with conscientiousness at the behavioral level to promote health risk behavior, with evidence for the interaction attenuated for distal health-related outcomes, such as physical functioning.
This study has several limitations that should be considered. The cross-sectional design precluded drawing causal inferences about the relationships among personality, education, and physical functioning. In addition, although the physical functioning measure used in this study has been well validated in relation to objective indicators of disability (Syddall, Martin, Harwood, Cooper, & Sayer, 2009), future research must consider using objective measures, such as walking speed (Tolea et al., 2010). In addition, further research is needed to identify the processes through which neuroticism contributes to physical functioning among older individuals with higher and lower level of education. Although SES is a multifaceted construct, it was only indexed by educational level in this study. However, unlike other markers such as income, wealth, and occupation, educational attainment is fixed early in life and thus relatively immune to reverse causality by personality in old age, is closely related to socioeconomic position, and does not change with age-related health decline (another possible avenue of reverse causality; Jagger, Matthews, Melzer, Matthews, & Brayne, 2007). However, future studies may consider including more sophisticated measure of education, for example, assessing categories of education levels reflecting the completion of different degrees, which may be more meaningfully reflective of the role education plays in personality and health. In addition, future research is needed to test whether our findings generalize to samples from other countries and whether the extent to which personality and education interact to predict that physical functioning depends upon individuals’ culture.
Through the identification of a synergistic relation between lower educational level and neuroticism, this work is the first to support the vulnerability model for the prediction of older adults’ physical functioning. Taken as a whole, it confirms that a focus on either personality or education without taking into account each other provides only a partial account of the predictors of basic daily physical activities in old age.
References
- Aiken L. S., West S. G. (1991). Multiple regression: Testing and interpreting interactions. Newbury Park, CA: Sage; [Google Scholar]
- Chapman B. P., Duberstein P., Lyness J. M. (2007). Personality traits, education, and health-related quality of life among older adult primary care patients. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 62, 343–352. 10.1093/geronb/ 62.6.P343 [DOI] [PubMed] [Google Scholar]
- Chapman B. P., Fiscella K., Duberstein P. R., Kawachi I. (2009). Education and smoking: Confounding or effect modification by phenotypic personality traits? Annals of Behavioral Medicine, 38, 237–248. 10.1007/s12160-009-9142-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chapman B. P., Roberts B., Duberstein P. (2011). Personality and longevity: Knowns, unknowns, and implications for public health and personalized medicine. Journal of Aging Research, 24. 10.4061/2011/759170 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Digman J. M. (1990). Personality structure: Emergence of the five-factor model. Annual Review of Psychology, 41, 417–440. 10.1146/annurev.ps.41.020190.002221 [Google Scholar]
- Duberstein P. R., Sörensen S., Lyness J. M., King D. A., Conwell Y., Seidlitz L., Caine E. D. (2003). Personality is associated with perceived health and functional status in older primary care patients. Psychology and Aging, 18, 25–37. 10.1037/0882-7974.18.1.25 [DOI] [PubMed] [Google Scholar]
- Jagger C., Matthews R., Melzer D., Matthews F., Brayne C. (2007. ). Educational differences in the dynamics of disability incidence, recovery and mortality: Findings from the MRC Cognitive Function and Ageing Study (MRC CFAS). International Journal of Epidemiology, 36, 358–365. 10.1093/ije/dyl307 [DOI] [PubMed] [Google Scholar]
- John O. P., Donahue E. M., Kentle R. L. (1991). The Big Five Inventory—Versions 4a and 54. Berkeley, CA: University of California, Berkeley, Institute of Personality and Social Research; [Google Scholar]
- Kivimaki M., Elovainio M., Kokko K., Pulkkinen L., Kortteinen M., Tuomikoski H. (2003). Hostility, unemployment and health status: Testing three theoretical models. Social Science and Medicine, 56, 2139–2152. 10.1016/S0277-9536(02)00219-8 [DOI] [PubMed] [Google Scholar]
- Plaisant O., Courtois R., Réveillère C., Mendelson G. A., John O. P. (2010). Analyse factorielle du Big Five Inventory français (BFI-Fr). Analyse convergente avec le NEO-PI-R [Factor structure and internal reliability of the French Big Five Inventory (BFI-Fr). Convergent and discriminant validation with the NEO-PI-R]. Annales Médico-Psychologiques, 168, 97–106. 10.1016/j.amp.2009.09.003 [Google Scholar]
- Rhodes R. E., Smith N. E. (2006). Personality correlates of physical activity: A review and meta-analysis. British Journal of Sports Medicine, 40, 958–965. 10.1136/bjsm.2006.028860 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Suchy Y., Williams P. G., Kraybill M. L., Franchow E., Butner J. (2010). Instrumental activities of daily living among community-dwelling older adults: Personality associations with self-report, performance, and awareness of functional difficulties. The Journals of Gerontology: Psychological Sciences and Social Sciences, 65, 542–550. 10.1093/geronb/gbq037 [DOI] [PubMed] [Google Scholar]
- Sulander T., Martelin T., Sainio P., Rahkonen O., Nissinen A., Uutela A. (2006). Trends and educational disparities in functional capacity among people aged 65–84 years. International Journal of Epidemiology, 35, 1255–1261. 10.1093/ije/dyl183 [DOI] [PubMed] [Google Scholar]
- Syddall H. E., Martin H. J., Harwood R. H., Cooper C., Sayer A. A. (2009). The SF-36: A simple, effective measure of mobility-disability for epidemiological studies. The Journal of Nutrition Health and Aging, 13, 57–62. 10.1007/s12603-009-0010-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Terracciano A., Löckenhoff C. E., Zonderman A. B., Ferrucci L., Costa P. T., Jr. (2008). Personality predictors of longevity: Activity, emotional stability, and conscientiousness. Psychosomatic Medicine, 70, 621–627. 10.1097/PSY.0b013e31817b9371 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tolea M., Costa P. T., Terracciano A., Griswold M., Simonsick E. M., Najjar S. S. … Ferrucci L. (2010). Sex-specific correlates of walking speed in a wide-age ranged population. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 65, 174–184. 10.1093/geronb/gbp130 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ware J. E., Sherbourne C. D. (1992). The MOS 36-item Short-Form Health Survey (SF-36): I. Conceptual framework and item selection. Medical Care, 30, 473–478. 10.1097/00005650-199206000-00002 [PubMed] [Google Scholar]