

Abstract
INTRODUCTION
Osteoma is a benign slow growing bone tumor with a prevalence of 3% of all benign paranasal sinuses tumors, with a peak incidence between the fourth and sixth decades, mostly involving frontal sinuses.1
PRESENTATION OF CASE
We present a case of a large right ethmoidal sinus osteoma in a 12-year-old boy, complaining of frontal headaches and excessive lacrimation of the right eye. CT scan showed a very large tumor in the right anterior ethmoidal sinus (30 mm × 25 mm × 15 mm).
DISCUSSION
Large osteomas of the paranasal sinuses are usually resected by external approaches. However, the minimally invasive endonasal approach, which minimizes external facial scarring, is challenging for such large lesions in pediatrics. In the presented case, the osteoma was successfully resected exclusively by endoscopy-guided endonasal approach assisted by neuronavigation, with no peri or postoperative complications.
CONCLUSION
An endoscopic approach assisted with neuronavigation may be a minimally invasive and safe procedure for managing large osteoma of the ethmoidal sinus in pediatrics patients.
Keywords: Osteoma, Benign paranasal sinuses tumors, Ethmoidal sinus osteoma, Pediatric ethmoidal osteoma
1. Introduction
Osteoma is a benign slow growing bone tumor with a prevalence of 3% of all benign paranasal sinuses tumors, with a peak incidence between the fourth and sixth decades and mostly involves frontal sinuses.1
We present a case of a large right ethmoidal sinus osteoma in a 12-year-old boy, complaining of frontal headaches and excessive lacrimation of the right eye. The CT scan showed a very large tumor in the right anterior ethmoidal sinus (30 mm × 25 mm × 15 mm).
Large osteoma of the paranasal sinuses are usually resected by external approaches, as the minimally invasive endonasal approach is challenging for such large lesions in pediatrics. In the presented case, the osteoma was successfully resected by an endoscopic-guided endonasal approach assisted by neuronavigation, with no peri or postoperative complications.
2. Case presentation
A 12-year-old boy, without past medical history, complained of persisting right frontal headache associated with excessive lacrimation of the right eye. Clinical examination showed a hard swelling in the right inner canthal area. Nasal fibroscopy revealed a high-located hard lesion in the right anterior nasal cavity. Computed tomography (CT) revealed a large calcified dense mass measuring 30 mm × 25 mm × 15 mm in the right anterior ethmoidal sinus with orbital extension and evidence of lacrymal sac compression and grade 1 exophthalmia (Figs. 1–3). The upper level of the tumor was in contact with the skull base near the right nasofrontal recess and agenesis of the underlying right frontal sinus. Routine blood tests and a chest X-ray were normal.
Fig. 1.

Sagittal CT scan revealed a large calcified dense mass measuring 30 mm × 25 mm × 15 mm in the right anterior ethmoidal sinus.
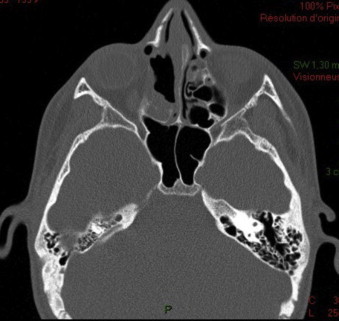
Fig. 2.
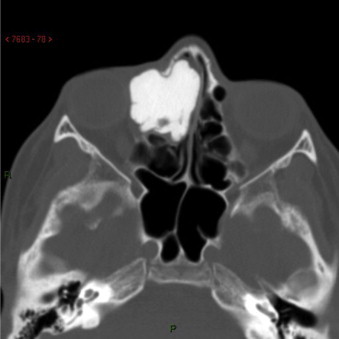
Axial CT revealed a large calcified dense mass measuring 30 mm × 25 mm × 15 mm in the right anterior ethmoidal sinus with orbital extension.
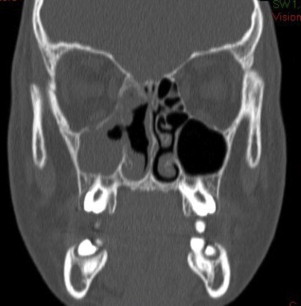
Fig. 3.
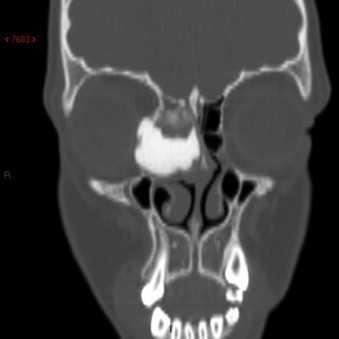
Coronal CT revealed a large calcified dense mass measuring 30 mm × 25 mm × 15 mm in the right anterior ethmoidal sinus with orbital extension and evidence of lacrymal sac compression.
The diagnosis of a large orbitoethmoidal osteoma was suspected and different surgical methods were discussed. A neuronavigation-guided endoscopic endonasal approach was planned.
The first step consisted in total excision of the nasal mucosa covering the tumor. The medial part of the osteoma was then carefully drilled using diamond burrs, notably at the level of the skull base. The orbitoethmoidal part of the osteoma was progressively dissected from the periorbit and then extracted in two pieces. Middle turbinectomy, radical ethmoidectomy and antrostomy of middle meatus were performed at the end of the operation. No cerebrospinal fluid (CSF) leakage was observed during the procedure (Figs. 4–6).
Fig. 4.
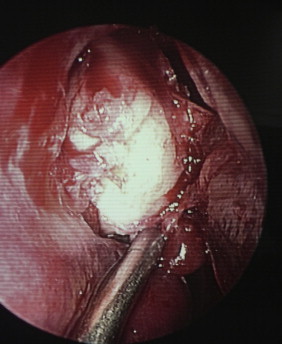
The beginning of the endoscopic dissection.
Fig. 5.

Successful removal of orbito-ethmoidal osteoma endoscopically.
Fig. 6.

The specimen after endoscopic endonasal drilling.
The histopathology analysis revealed a compact bone tissue transversed by channels of Havers, with no evidence of malignancy (Fig. 7).
Fig. 7.
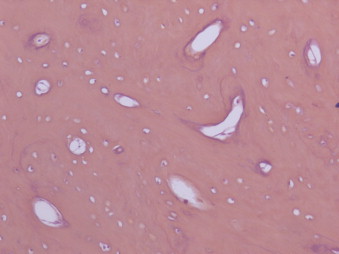
The histopathology analysis revealed a compact bone tissue.
There were no complications of bleeding or CSF leakage during the postoperative period. A CT scan was performed at six months, and showed no residual tumor (Figs. 8 and 9).
Fig. 8.
Postoperative coronal CT scan (6 months).
Fig. 9.
Postoperative axial CT scan (6 months).
3. Discussion
Different theories regarding the etiology of osteomas have been proposed including developmental, traumatic, and infective origins.2,3 The second most common area to be affected by osteomas is the ethmoidal sinuses.4 however osteomas are rare in pediatrics.1 Although CT scan may be used to make a preliminary diagnosis, a definitive diagnosis is obtained by histopathology analysis as osteoma could be misdiagnosed as displasic bone tumors.5 In our opinion, preoperative work-up and investigation should include an MRI for skull anatomical assessment and verification of any tumor extension causing skull base defects, in addition to CT scan.
Surgical excision of large osteomas is suggested when it causes chronic sinusitis, exceeding the sinuses’ boundaries or causing headaches after excluding all other possible causes, as in this case.6 Georgalas et al. recommend observation of small asymptomatic osteomas.1
Surgical approaches might vary from pediatric patient to another. Endoscopic procedures are known to be more difficult in children due to their narrow nasal cavity and thus require higher surgical experience.7 In this case, we decided to perform a neuronavigation-guided endoscopic endonasal approach, while being prepared to convert to an open approach (Lynch procedure) or lateral rhinotomy if needed. The neuronavigation-guided endoscopic endonasal approach is a minimally invasive and safe procedure for the management of some large osteoma of the ethmoidal sinus in pediatric patients.
Conflict of interest statement
None declared.
Funding
None.
Ethical approval
Consent obtained.
Author contributions
Naif Alotaibi helped in the conception, design and writing. Julien Hanss helped in design, writing and obtaining consent. Farida Benoudiba, Serge Bobin, Emmanuel Racy contributed equally in writing.
Footnotes
This is an open-access article distributed under the terms of the Creative Commons Attribution-NonCommercial-No Derivative Works License, which permits non-commercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
Contributor Information
Naif Alotaibi, Email: naif.alotaibi@u-psud.fr, dr.n.otaibi@gmail.com.
Julien Hanss, Email: julien.hanss@hotmail.fr.
Farida Benoudiba, Email: farida.benoudiba@bct.aphp.fr.
Serge Bobin, Email: serge.bobin@bct.aphp.fr.
Emmanuel Racy, Email: emmanuelracy@gmail.com.
References
- 1.Christos Georgalas, John Goudakos, Fokkens Wytske J. Osteoma of the skull base and sinuses. Otolaryngol Clin North Am. 2011;44:875–890. doi: 10.1016/j.otc.2011.06.008. [DOI] [PubMed] [Google Scholar]
- 2.Eller R. Common fibro-osseous lesions of the paranasal sinuses. Otolaryngol Clin North Am. 2006;39(3):585–600. doi: 10.1016/j.otc.2006.01.013. [DOI] [PubMed] [Google Scholar]
- 3.Hallberg O.E., Begley J.W. Origin and treatment of osteomas of the paranasal sinuses. Arch Otolaryngol. 1950;51(5):750–760. doi: 10.1001/archotol.1950.00700020775012. [DOI] [PubMed] [Google Scholar]
- 4.Earwaker J. Paranasal sinus osteomas: a review of 46 cases. Skeletal Radiol. 1993;22(August (6)):417–423. doi: 10.1007/BF00538443. [DOI] [PubMed] [Google Scholar]
- 5.Moretti A., Croce A., Leone O., D‘Agostino L. Osteoma of maxillary sinus: case report. Acta Otorhinolaryngol Ital. 2004;24(August (4)):219–222. [PubMed] [Google Scholar]
- 6.Savic D.L., Djeric D.R. Indications for the surgical treatment of osteomas of the frontal and ethmoid sinuses. Clin Otolaryngol Allied Sci. 1990;15(October (5)):397–404. doi: 10.1111/j.1365-2273.1990.tb00490.x. [DOI] [PubMed] [Google Scholar]
- 7.Ibrahim Ahmad A., Magdy Emad A., Mohamed Eid. Endoscopic endonasal multilayer repair of traumatic ethmoidal roof cerebrospinal fluid rhinorrhea in children. Int J Pediatr Otorhinolaryngol. 2012;76(4):523–529. doi: 10.1016/j.ijporl.2012.01.009. [DOI] [PubMed] [Google Scholar]